
Translate this page into:
Symmetrical peripheral gangrene secondary to septic shock induced by Streptococcus dysgalactiae subspecies equisimilis infection
-
Received: ,
Accepted: ,
How to cite this article: Kondo A, Terashima-Murase C, Hidaka Y, Fukaura R, Kanematsu T, Matsushita T, et al. Symmetrical peripheral gangrene secondary to septic shock induced by Streptococcus dysgalactiae subspecies equisimilis infection. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_576_2023
Dear Editor,
A 72-year-old man presented to the emergency department with a 5-day history of a slight fever and haematochezia. The patient had a past medical history of acquired haemophilia A and hepatocellular carcinoma. On physical examination, he was febrile and in shock (temperature 38.5 degrees, heart rate 110 bpm, systolic blood pressure 50 mmHg). Gastrointestinal endoscopy and a contrast-CT of the abdomen and pelvis were performed but they failed to identify the source of the bleeding or infection. During the endoscopy, he developed aspiration pneumonia and was intubated and admitted to the medical intensive care unit (ICU). He was treated for sepsis empirically with piperacillin–tazobactam. Initial blood examination showed a white blood cell count of 2.4 × 103/μL, red blood cell count of 351 × 104/μL, platelet count of 4.7 × 104/μL, CRP of 15.81 mg/dL, lactate of 5.72 mmol/L, PT INR of 2.4 and fibrinogen of 154 mg/dL. He was given fluid resuscitation, intravenous norepinephrine and vasopressin and a blood transfusion. Continuous veno-venous haemodialysis was necessary by the eighth day of admission due to acute renal failure. Blood cultures and a urine culture both grew Streptococcus dysgalactiae subspecies equisimilis (SDSE). It was noticed that his left shoulder was swollen within the first few days of admission and a shoulder joint aspirate fluid culture also grew SDSE. Piperacillin–tazobactam was substituted with penicillin G and clindamycin. On the sixth day of admission, he developed skin necrosis on the tips of all the fingers and toes [Figures 1a–1d]. Serum protein C activity was 41% (normal range, 64–146%) and protein S activity was 71% (normal range, 67–164%). A biopsy was attempted from the digits; however, a satisfactory sample could not be obtained due to the degree of necrosis. His general condition gradually improved with the treatment and he had his fingers and toes amputated 2 months after admission [Figures 2a–2d and 2e–2h].

- Seventy two-year-old man presenting with peripheral symmetrical gangrene involving all fingers and toes.
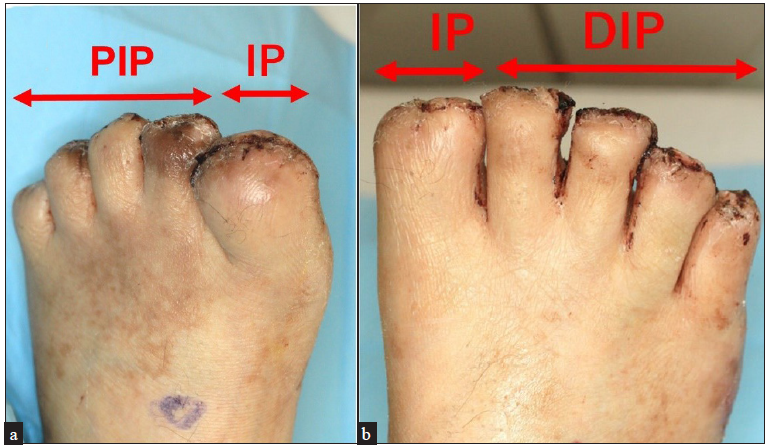
- Photographs of both feet following amputation, two weeks after the surgery. The great toe was amputated at the interphalangeal joint and the rest of the toes were amputated at the proximal or distal interphalangeal joints. IP: Interphalangeal joint; DIP: Distal interphalangeal joint.
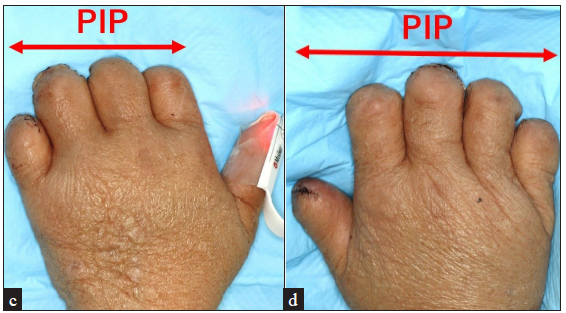
- Photographs of both hands following amputation, two weeks after the surgery. The fingers were amputated at the proximal interphalangeal joints. PIP: Proximal interphalangeal joint.

- Photographs of the extremities following amputation, seven weeks after the amputation surgery.
Given the clinical presentation over the extremities accompanied by a history of septic shock and evidence of acute clotting disturbance, a diagnosis of symmetrical peripheral gangrene (SPG) was made.
SPG is a life-threatening condition characterised by a triad of shock, disseminated intravascular coagulation (DIC) and anticoagulant depletion.1 It has been speculated that a reduction in protein C is involved in the aetiopathogenesis.1 SPG is associated with a high mortality and it has been reported that more than half of the surviving patients required amputations of the limbs.2,3 In the present case, fortunately, the necrotic area was localised and amputation at the level of interphalangeal joints was adequate.
Many causes for SPG have been identified. Non-infectious causes include acute or chronic liver disease and iatrogenic causes including vasopressor use and colloidal transfusions.1,2 Various infective agents have been reported to be associated with SPG, including common agents such as Pneumococci, and E. coli and rare agents such as Serratia marcescens and SARS-CoV-2.3–6 The exact incidence of these causative factors cannot be determined due to the rarity of SPG, but it has been suggested that pneumococcal sepsis is the most common infectious cause of SPG with one study reporting its association with 28.5% of cases.4 In the same study, E. coli was found to be associated with 14.3% of cases.4 Our patient had SDSE infection which has not been reported to be associated with SPG previously. SDSE is a group C or G β-hemolytic streptococci that resides in the human nasopharynx, skin and perineum. Several clinical case series have reported SDSE infections to be more common among elder adults and in individuals with underlying chronic illnesses. SDSE has been implicated in a wide variety of human infections and the incidence of invasive disease due to SDSE may be increasing.7 Because of these characteristics, we envisage SDSE infections to become a significant health burden in the near future, given the ageing population in developed countries. The present case highlights the importance of rapid identification of SDSE, as it has the potential to cause extremely serious complications with high mortality like SPG.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr Matsushita declares COI from Chugai, NOVO Nordisk, Takeda, Bayer, Sanofi, CSL, JB, KMB, Fujimoto, Sysmex, JSTH and JSTMCT. Dr Kanematsu declares COI from Sanofi, Bayer, Chugai, NOVO Nordisk and JB.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Symmetrical peripheral gangrene in critical illness. Transfus Apher Sci. 2021;60:103094.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors of vasopressor-induced symmetrical peripheral gangrene. Ann Plast Surg. 2018;80:622-627.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Symmetrical peripheral gangrene caused by septic shock. Case Reports Plast Surg Hand Surg. 2015;28:53-56.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Symmetrical peripheral gangrene: A prospective study of 14 consecutive cases in a tertiary-care hospital in eastern India. J Eur Acad Dermatol Venereol. 2010;24:214-218.
- [CrossRef] [PubMed] [Google Scholar]
- Symmetrical peripheral gangrene in a patient with septic shock due to Serratia marcescens. J Dermatol. 2022;49:e181-e182.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19 associated symmetrical peripheral gangrene: A case series. Diabetes Metab Syndr. 2022;16:102356.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Clonal clusters and virulence factors of group C and G streptococcus causing severe infections, Manitoba, Canada, 2012–2014. Emerg Infect Dis. 2017;23:1079-1088.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




