Translate this page into:
Targeted phototherapy
2 Department of Dermatology, Mandya Institute of Medical Sciences, Mandya, Karnataka, India
Correspondence Address:
Venkataram Mysore
Venkat Charmalaya - Centre for Advanced Dermatology, Bengaluru - 560 040, Karnataka
India
| How to cite this article: Mysore V, Shashikumar B M. Targeted phototherapy. Indian J Dermatol Venereol Leprol 2016;82:1-6 |
Abstract
Background: Targeted phototherapy is a new form of phototherapy which has many advantages and disadvantages over conventional phototherapy. This article reviews the different technologies and outlines recommendations based on current evidence. Methods: A literature search was performed on targeted phototherapy to collect data. Relevant literature published till March 2014 was obtained from PubMed, EMBASE, and the Cochrane Library. Keywords like “targeted phototherapy”, “excimer laser”, “excimer lamp”, “Nonchromatic ultraviolet light”, “vitiligo”, and “psoriasis”, were used for literature search. All systematic reviews, meta-analysis, national guidelines, randomized controlled trials (RCT), prospective open label studies and retrospective case series in English were reviewed. Results: Three hundred and forty studies were evaluated, 24 of which fulfilled the criteria for inclusion in the guidelines. Conclusions and Recommendations: All forms of targeted phototherapy are useful in vitiligo. Good responses were seen in localized involvement, resistant lesions and in children in whom their use is more accepted and convenient (Level of evidence 2+, Grade of recommendation B). Similarly it is useful in psoriasis, either alone or in combination with drugs, even in resistant forms such as palmoplantar psoriasis. In view of expense and practical application, their use is limited to resistant lesions and localized disease. (Level of evidence 2+, Grade of recommendation B). But in other conditions there is no convincing evidence for its use. (Level of evidence 3+, Grade of recommendation C).Introduction
Targeted phototherapy (also called concentrated phototherapy, focused phototherapy and microphototherapy) is a new form of phototherapy which seeks to overcome some of the disadvantages with conventional phototherapy.[1],[2],[3],[4] This modality involves application of light energy directly focused on or targeted at the lesion through special delivery mechanisms such as fiberoptic cables. The term “targeted phototherapy” includes different technologies such as excimer laser (308 nm), intense pulse light systems and non-laser ultraviolet light sources with improved hand-held delivery systems.
Several advantages have been claimed for targeted phototherapy:[3],[5]
- Exposure of involved areas only and sparing of uninvolved areas, thus minimizing acute side effects such as erythema and long-term risk of skin cancer on unaffected skin
- Quick delivery of energy and thereby shortened duration of treatment
- Delivery of higher doses (supererythemogenic doses) of energy because uninvolved areas are not exposed. Higher doses of energy can be delivered selectively to the lesions thereby enhancing efficacy and achieving faster response
- This has been claimed to shorten duration of treatment leading to less frequent visits to the clinic and thereby lessening inconvenience for the patient
- The maneuverable handpiece allows treatment of difficult areas such as the scalp, nose, genitals, oral mucosa and ear
- Easy administration for children as delivery is hand-held
- Targeted phototherapy machines occupy less space.
However, targeted phototherapy devices have certain disadvantages. They are more expensive. Furthermore, they are not adequate to treat extensive areas given the cost of treatment and time involved. They are not recommended for use if lesions occur over more than 10% of the body area.
Different technologies can deliver targeted phototherapy and these include:
- Excimer laser (xenon chloride laser 308 nm)
- Excimer light (non-coherent monochromatic light source 304–308 nm)
- Non-chromatic ultraviolet light sources (either broadband, 290–310 nm or narrowband, 313 nm).[5]
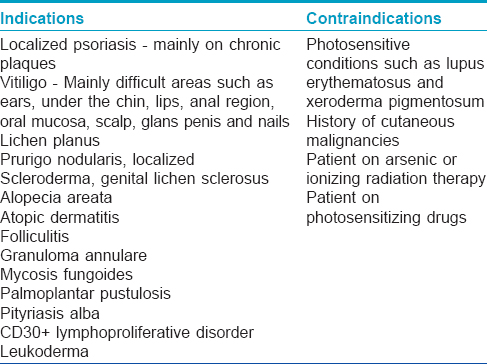
The advantages of the light sources over excimer laser include smaller size, lesser maintenance problems and lower cost. Some machines also include the ultraviolet A spectrum and this is an added advantage. [Table - 1] shows the various indications and contraindications of targeted phototherapy.[6],[7]
Methods
Relevant literature published until March 2014 was obtained from PubMed, EMBASE and the Cochrane Library. Keywords such as “targeted phototherapy,” “excimer laser,” “excimer lamp,” “non-chromatic ultraviolet light,” “vitiligo” and “psoriasis” were used for literature search. All systematic reviews, meta-analysis, national guidelines, randomized controlled trials, prospective open-label studies and retrospective case series in English were reviewed. The levels of evidence and grades of recommendations for each guideline were according to the format suggested by the British Association of Dermatologists. The studies selected were assessed for their methodology as per the NICE Technical Manual and graded using a code “++,” “+” or '”−,” based on the extent to which potential biases were minimized. Thereafter, the grade of recommendation was made.
Results
Three hundred and forty studies were evaluated, 24 of which fulfilled the criteria for inclusion in the guidelines.
Therapeutic efficacy in different conditions
Targeted phototherapy has been shown to be effective in several indications [Table - 1] wherever conventional phototherapy has been previously used. Some of these indications are discussed below.
Vitiligo
Excimer laser
Low fluencies (50–200 mJ/cm 2) were used in vitiligo compared to psoriasis. An initial dose of 200 mJ (150 mJ for women and men under 16 years of age) was used by Shi et al.[8] The subsequent dose was determined as follows: dose increased 20% from treatment 1 to 10, 10% from treatment 11 to 13, 5% from treatment 14 to 16 and 2% from treatment 17 to 20 sessions. If symptomatic erythema or blistering developed, one or two treatments were withheld until resolution of phototoxicity; when treatment was resumed, the dose was reduced to the last well-tolerated dose. Sessions were performed once, twice or 3 times a week. Although administering treatments more frequently (i.e. 2 or 3/week) appears to trigger earlier repigmentation of vitiligo patches, the start of repigmentation appears to depend ultimately on the total number of laser treatment sessions.[9]
Several studies have demonstrated the efficacy of excimer laser in vitiligo. A pilot study in 2002 showed significant benefits among vitiligo patients in 29 patches of vitiligo from 18 patients. Twenty three vitiligo patches from 12 patients received at least 6 treatments and resulted in some repigmentation in 57% of the treated patches. Eleven vitiligo patches from 6 patients received 12 treatments and resulted in some repigmentation in 82% of the treated patches, with parameters 120 ns, 20 Hz pulse with a 10 mm × 10 mm spot size and a power output of 60 mW of laser light. The study concluded that “the degree of repigmentation in a period of 2–4 weeks is much higher than that achieved with any other present vitiligo therapy”. The xenon chloride excimer laser may represent a new treatment modality for the management of stable vitiligo.[4] These results were confirmed by other studies which showed benefit with excimer laser in patients of localized vitiligo that had been unsuccessfully treated with other modalities of treatment.[10] A large study of 140 patients with vitiligo treated by excimer laser showed excellent results in ultraviolet-sensitive areas while ultraviolet-resistant areas such as acral lesions and lesions on joint areas responded poorly.[11] However, these and other studies were small studies in some patients and uncontrolled.[12] A meta-analysis comprising seven randomized controlled studies with 390 vitiligo patients showed no significant differences between 308-nm excimer laser and 308-nm excimer lamp when evaluating either ≥75% or ≥50% repigmentation rate, or between 308-nm excimer laser and narrowband ultraviolet B on either 100% or ≥75% repigmentation rate. However, more lesions achieved ≥50% repigmentation when treated with 308-nm excimer laser than with narrowband ultraviolet B (level of evidence 1+).[13]
Excimer light
Several studies have been published which demonstrate the efficacy of excimer light (intense pulsed light). In a pilot study of excimer light in 37 patients of vitiligo, Leone et al. obtained initial repigmentation in the first eight treatments and excellent repigmentation in 50% of patients at 6 months.[14] Some patients who had not previously responded to narrow band ultraviolet B therapy were also found to respond. The results were comparable to excimer laser and superior to narrowband phototherapy. Studies have suggested that combination with topical immunomodulators and fluticasone could enhance the clinical response in vitiligo, especially in more resistant anatomical sites and in segmental vitiligo (level of evidence 1+).[15],[16],[17]
Non-coherent targeted ultraviolet B phototherapy devices
Several non-coherent light sources have been shown to be effective in vitiligo.[18],[19] A study by Akar et al. in 32 patients using Daavlin T500x high-dose targeted phototherapy system showed that therapeutic effectiveness is limited and depends on the locations of vitiligo lesions. In this study, only 4 (12.5%) of 32 patients showed visible repigmentation. All the lesions responsive to treatment were facial lesions.[20] Welsh et al. too demonstrated that extremities did not respond satisfactorily.[21] In a prospective intra-patient placebo-controlled randomized trial, 20% of the lesions treated with narrowband ultraviolet B achieved repigmentation scores above 50% but none of the lesions treated with monochromatic excimer light achieved a repigmentation higher than 50% after 24 sessions (level of evidence 1+).[22] In a similar multicenter controlled study comparing 308-nm monochromatic excimer light and narrowband ultraviolet B phototherapy, results with 308-nm monochromatic excimer light were superior (level of evidence 1+).[23]
Summary of recommendations in vitiligo
Evidence suggests that all forms of targeted phototherapy are useful in vitiligo. They can be used in combination with other drugs. However, response is limited to hairy areas and acral, resistant areas are resistant to these new and expensive treatment modalities, too. Hence, these devices may be used in localized areas, in resistant lesions and in children in whom their use is more acceptable and convenient (grade of recommendation B).
Targeted phototherapy in psoriasis
Excimer laser
The initial dose can be calculated by determining the minimal erythema dose for each plaque or fixed doses can be calculated from the thickness of the lesions which are then decreased depending on the clinical improvement. Usually, treatment is started with a dose of light 1–3 times the minimal erythema doses with progressive increase in doses depending on clinical results and tolerance. Selectivity of the laser allows doses to be adapted to each lesion rather than calculated from the minimal erythema dose. The initial dose was maintained until plaques thinned or flattened considerably or pigment appeared. Once plaques thinned or became hyperpigmented (or both), the dose was reduced by 1 minimal erythema dose.[24],[25],[26],[27] Frequency of therapy varied from 1 to 3 sessions per week.
In psoriasis, the efficacy of excimer laser has been confirmed by several reports.[11],[28],[29] Localized resistant lesions of psoriasis on elbow and knees were reported to be cleared in as few as 1–3 exposures with moderately long remissions.[28] Scalp psoriasis was also shown to respond well.[3] In another study which evaluated patient satisfaction, 55% of patients reported overall satisfaction and 25% reported that laser treatments were better than any other treatment they had tried.[30] Side effects reported, though usually mild, included burning pain during and after treatment, severe erythema and blistering of the skin.
After a period of initial excitement, subsequent studies have led to a reappraisal of the role of excimer laser in psoriasis.[31],[32] Comparison of excimer laser, excimer lamp and 311-nm narrowband ultraviolet B in patients with psoriasis showed similar clearance and no statistically significant difference in results after 10 weeks of treatment.[31] The study did show enhanced clearance in the group of patients treated with the excimer laser when they were treated using an accelerated scheme of administration but these patients also had a higher rate of side effects such as blistering and crusting. The study concluded that “the only advantage of laser seems to be the ability to treat exclusively the affected skin and with a reduced cumulative dose, thus perhaps reducing the long term risk of carcinogenicity.” This experience has been confirmed in another similar study.[33] A study evaluated seven published reports on the use of excimer laser and concluded that there is no consensus for a single excimer laser therapy protocol and as a result, patient preferences should continue to be an important consideration for phototherapy regimen planning (level of evidence 1+).[34]
Non-laser light sources
Non-laser light sources have proven popular because of their small size and lower costs. Some studies have demonstrated the safety and efficacy of these machines in psoriasis. Both ultraviolet B (narrowband and broadband) and ultraviolet A therapies, alone and in combination with drugs such as calcipotriol and dithranol have been shown to be effective (level of evidence 2+).[35],[36],[37],[38],[39],[40],[41],[42]
Summary of recommendations
All forms of targeted phototherapy are useful in psoriasis, either alone or in combination with drugs, even in resistant forms such as palmoplantar psoriasis. Given expense and practical application, their use is limited to resistant lesions and localized disease (grade of recommendation B).
Other conditions
Excimer laser has been reported to be effective in other dermatoses also such as oral lichen planus, alopecia areata, atopic dermatitis, mycosis fungoides and lymphomatoid papulosis.[43],[44],[45],[46] Interestingly, excimer laser has been found to be effective in hypopigmented striae, hypopigmented scars, acne vulgaris and other diseases and conditions generally considered difficult to treat.[47],[48],[49],[50],[51] Increase in melanin pigment, hypertrophy of melanocytes and an increase in melanocytes within striae leading to darkening of striae were reported after use of excimer laser.[52] These results, if confirmed by larger studies, will open up exciting new avenues for the treatment of these important and common cosmetic problems.
Summary of recommendations
Most of these studies are isolated reports in a small number of cases. Hence, the therapy needs to be used after a careful consideration of cost and benefit (grade of recommendation C).
Summary
Targeted phototherapy is an exciting new technology in the management of several dermatological conditions. Their main advantages are safety, ease of administration and suitability for difficult to treat areas and in children. There is no conclusive evidence that they are superior to existing technologies and are also more expensive. Hence, their use may be undertaken in selected cases as outlined.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Hamzavi I, Lui H. Using light in dermatology: An update on lasers, ultraviolet phototherapy, and photodynamic therapy. Dermatol Clin 2005;23:199-207.
[Google Scholar]
|
| 2. |
Spencer JM, Hadi SM. The excimer lasers. J Drugs Dermatol 2004;3:522-5.
[Google Scholar]
|
| 3. |
Grimes PE. Advances in the treatment of vitiligo: Targeted phototherapy. Cosmet Dermatol 2003;16:18-22.
[Google Scholar]
|
| 4. |
Spencer JM, Nossa R, Ajmeri J. Treatment of vitiligo with the 308-nm excimer laser: A pilot study. J Am Acad Dermatol 2002;46:727-31.
[Google Scholar]
|
| 5. |
Mysore V. Targeted phototherapy. Indian J Dermatol Venereol Leprol 2009;75:119-25.
[Google Scholar]
|
| 6. |
Mehraban S, Feily A. 308 nm excimer laser in dermatology. J Lasers Med Sci 2014;5:8-12.
[Google Scholar]
|
| 7. |
Dogra S, De D. Narrowband ultraviolet B in the treatment of psoriasis: The journey so far! Indian J Dermatol Venereol Leprol 2010;76:652-61.
[Google Scholar]
|
| 8. |
Shi Q, Li K, Fu J, Wang Y, Ma C, Li Q, et al. Comparison of the 308-nm excimer laser with the 308-nm excimer lamp in the treatment of vitiligo – A randomized bilateral comparison study. Photodermatol Photoimmunol Photomed 2013;29:27-33.
[Google Scholar]
|
| 9. |
Hofer A, Hassan AS, Legat FJ, Kerl H, Wolf P. Optimal weekly frequency of 308-nm excimer laser treatment in vitiligo patients. Br J Dermatol 2005;152:981-5.
[Google Scholar]
|
| 10. |
Taneja A, Trehan M, Taylor CR. 308-nm excimer laser for the treatment of localized vitiligo. Int J Dermatol 2003;42:658-62.
[Google Scholar]
|
| 11. |
Choi KH, Park JH, Ro YS. Treatment of vitiligo with 308-nm xenon-chloride excimer laser: Therapeutic efficacy of different initial doses according to treatment areas. J Dermatol 2004;31:284-92.
[Google Scholar]
|
| 12. |
Hadi S, Tinio P, Al-Ghaithi K, Al-Qari H, Al-Helalat M, Lebwohl M, et al. Treatment of vitiligo using the 308-nm excimer laser. Photomed Laser Surg 2006;24:354-7.
[Google Scholar]
|
| 13. |
Sun Y, Wu Y, Xiao B, Li L, Li L, Chen HD, et al. Treatment of 308-nm excimer laser on vitiligo: A systemic review of randomized controlled trials. J Dermatolog Treat 2015;26:347-53.
[Google Scholar]
|
| 14. |
Leone G, Iacovelli P, Paro Vidolin A, Picardo M. Monochromatic excimer light 308 nm in the treatment of vitiligo: A pilot study. J Eur Acad Dermatol Venereol 2003;17:531-7.
[Google Scholar]
|
| 15. |
Nisticò S, Chiricozzi A, Saraceno R, Schipani C, Chimenti S. Vitiligo treatment with monochromatic excimer light and tacrolimus: Results of an open randomized controlled study. Photodermatol Photoimmunol Photomed 2011;27:108-10.
[Google Scholar]
|
| 16. |
Coelho JD, Ferreira A. Association of targeted intense pulse light system, UVA1-UVB and fluticasone in the treatment of vitiligo: Prospective study of 10 patients. Photodermatol Photoimmunol Photomed 2009;25:161-3.
[Google Scholar]
|
| 17. |
Lee DY, Kim CR, Lee JH. Targeted phototherapy in combination with drug therapy for segmental vitiligo. Photodermatol Photoimmunol Photomed 2011;27:108-10.
[Google Scholar]
|
| 18. |
Lotti TM, Menchini G, Andreassi L. UV-B radiation microphototherapy. An elective treatment for segmental vitiligo. J Eur Acad Dermatol Venereol 1999;13:102-8.
[Google Scholar]
|
| 19. |
Menchini G, Tsoureli-Nikita E, Hercogova J. Narrow-band UV-B micro-phototherapy: A new treatment for vitiligo. J Eur Acad Dermatol Venereol 2003;17:171-7.
[Google Scholar]
|
| 20. |
Akar A, Tunca M, Koc E, Kurumlu Z. Broadband targeted UVB phototherapy for localized vitiligo: A retrospective study. Int J Dermatol 2009;48:529-34.
[Google Scholar]
|
| 21. |
Welsh O, Herz-Ruelas ME, Gómez M, Ocampo-Candiani J. Therapeutic evaluation of UVB-targeted phototherapy in vitiligo that affects less than 10% of the body surface area. Int J Dermatol 2009;48:529-34.
[Google Scholar]
|
| 22. |
Verhaeghe E, Lodewick E, van Geel N, Lambert J. Intrapatient comparison of 308-nm monochromatic excimer light and localized narrow-band UVB phototherapy in the treatment of vitiligo: A randomized controlled trial. Dermatology 2011;223:343-8.
[Google Scholar]
|
| 23. |
Casacci M, Thomas P, Pacifico A, Bonnevalle A, Paro Vidolin A, Leone G. Comparison between 308-nm monochromatic excimer light and narrowband UVB phototherapy (311-313 nm) in the treatment of vitiligo – A multicentre controlled study. J Eur Acad Dermatol Venereol 2007;21:956-63.
[Google Scholar]
|
| 24. |
Feldman SR, Mellen BG, Housman TS, Fitzpatrick RE, Geronemus RG, Friedman PM, et al. Efficacy of the 308-nm excimer laser for treatment of psoriasis: Results of a multicenter study. J Am Acad Dermatol 2002;46:900-6.
[Google Scholar]
|
| 25. |
Trehan M, Taylor CR. Medium-dose 308-nm excimer laser for the treatment of psoriasis. J Am Acad Dermatol 2002;47:701-8.
[Google Scholar]
|
| 26. |
Taneja A, Trehan M, Taylor CR. 308-nm excimer laser for the treatment of psoriasis: Induration-based dosimetry. Arch Dermatol 2003;139:759-64.
[Google Scholar]
|
| 27. |
Gerber W, Arheilger B, Ha TA, Hermann J, Ockenfels HM. Ultraviolet B 308-nm excimer laser treatment of psoriasis: A new phototherapeutic approach. Br J Dermatol 2003;149:1250-8.
[Google Scholar]
|
| 28. |
Asawanonda P, Anderson RR, Chang Y, Taylor CR. 308-nm excimer laser for the treatment of psoriasis: A dose-response study. Arch Dermatol 2000;136:619-24.
[Google Scholar]
|
| 29. |
Morison WL, Atkinson DF, Werthman L. Effective treatment of scalp psoriasis using the excimer (308 nm) laser. Photodermatol Photoimmunol Photomed 2006;22:181-3.
[Google Scholar]
|
| 30. |
Rodewald EJ, Housman TS, Mellen BG, Feldman SR. Follow-up survey of 308-nm laser treatment of psoriasis. Lasers Surg Med 2002;31:202-6.
[Google Scholar]
|
| 31. |
Köllner K, Wimmershoff MB, Hintz C, Landthaler M, Hohenleutner U. Comparison of the 308-nm excimer laser and a 308-nm excimer lamp with 311-nm narrowband ultraviolet B in the treatment of psoriasis. Br J Dermatol 2005;152:750-4.
[Google Scholar]
|
| 32. |
Rivort J. Experience with excimer laser. J Drugs Dermatol 2006;5:550-4.
[Google Scholar]
|
| 33. |
He YL, Zhang XY, Dong J, Xu JZ, Wang J. Clinical efficacy of a 308 nm excimer laser for treatment of psoriasis vulgaris. Photodermatol Photoimmunol Photomed 2007;23:238-41.
[Google Scholar]
|
| 34. |
Mudigonda T, Dabade TS, Feldman SR. A review of protocols for 308 nm excimer laser phototherapy in psoriasis. J Drugs Dermatol 2012;11:92-7.
[Google Scholar]
|
| 35. |
Kaur M, Oliver B, Hu J, Feldman SR. Nonlaser UVB-targeted phototherapy treatment of psoriasis. Cutis 2006;78:200-3.
[Google Scholar]
|
| 36. |
Toll A, Vélez-González M, Gallardo F, Gilaberte M, Pujol RM. Treatment of localized persistent plaque psoriasis with incoherent narrowband ultraviolet B phototherapy. J Dermatolog Treat 2005;16:165-8.
[Google Scholar]
|
| 37. |
Amornpinyokeit N, Asawanonda P. 8-Methoxypsoralen cream plus targeted narrowband ultraviolet B for psoriasis. Photodermatol Photoimmunol Photomed 2006;22:285-9.
[Google Scholar]
|
| 38. |
Lapidoth M, Adatto M, David M. Targeted UVB phototherapy for psoriasis: A preliminary study. Clin Exp Dermatol 2007;32:642-5.
[Google Scholar]
|
| 39. |
Ozkan I, Köse O, Ozmen I, Arca E. Efficacy and safety of non-laser, targeted UVB phototherapy alone and in combination with psoralen gel or calcipotriol ointment in the treatment of localized, chronic, plaque-type psoriasis. Int J Dermatol 2012;51:609-13.
[Google Scholar]
|
| 40. |
Wollina U, Koch A, Scheibe A, Seme B, Streit I, Schmidt WD. Targeted 307 nm UVB-phototherapy in psoriasis. A pilot study comparing a 307 nm excimer light with topical dithranol. Skin Res Technol 2012;18:212-8.
[Google Scholar]
|
| 41. |
Nishida E, Furuhashi T, Kato H, Kaneko N, Shintani Y, Morita A. Successful treatment of psoriasis vulgaris with targeted narrow-band ultraviolet B therapy using a new flat-type fluorescent lamp. Photodermatol Photoimmunol Photomed 2011;27:248-50.
[Google Scholar]
|
| 42. |
Kemény L, Csoma Z, Bagdi E, Banham AH, Krenács L, Koreck A. Targeted phototherapy of plaque-type psoriasis using ultraviolet B-light-emitting diodes. Br J Dermatol 2010;163:167-73.
[Google Scholar]
|
| 43. |
Köllner K, Wimmershoff M, Landthaler M, Hohenleutner U. Treatment of oral lichen planus with the 308-nm UVB excimer laser – Early preliminary results in eight patients. Lasers Surg Med 2003;33:158-60.
[Google Scholar]
|
| 44. |
Gundogan C, Greve B, Raulin C. Treatment of alopecia areata with the 308-nm xenon chloride excimer laser: Case report of two successful treatments with the excimer laser. Lasers Surg Med 2003;33:158-60.
[Google Scholar]
|
| 45. |
Baltás E, Csoma Z, Bodai L, Ignácz F, Dobozy A, Kemény L. Treatment of atopic dermatitis with the xenon chloride excimer laser. J Eur Acad Dermatol Venereol 2006;20:657-60.
[Google Scholar]
|
| 46. |
Kontos AP, Kerr HA, Malick F, Fivenson DP, Lim HW, Wong HK. 308-nm excimer laser for the treatment of lymphomatoid papulosis and stage IA mycosis fungoides. Photodermatol Photoimmunol Photomed 2006;22:168-71.
[Google Scholar]
|
| 47. |
Goldberg DJ, Sarradet D, Hussain M. 308-nm excimer laser treatment of mature hypopigmented striae. Dermatol Surg 2003;29:596-8.
[Google Scholar]
|
| 48. |
Goldberg DJ, Marmur ES, Schmults C, Hussain M, Phelps R. Histologic and ultrastructural analysis of ultraviolet B laser and light source treatment of leukoderma in striae distensae. Dermatol Surg 2005;31:385-7.
[Google Scholar]
|
| 49. |
Alexiades-Armenakas MR, Bernstein LJ, Friedman PM, Geronemus RG. The safety and efficacy of the 308-nm excimer laser for pigment correction of hypopigmented scars and striae alba. Arch Dermatol 2004;140:955-60.
[Google Scholar]
|
| 50. |
Aubin F, Vigan M, Puzenat E, Blanc D, Drobacheff C, Deprez P, et al. Evaluation of a novel 308-nm monochromatic excimer light delivery system in dermatology: A pilot study in different chronic localized dermatoses. Br J Dermatol 2005;152:99-103.
[Google Scholar]
|
| 51. |
Noborio R, Nishida E, Kurokawa M, Morita A. A new targeted blue light phototherapy for the treatment of acne. Photodermatol Photoimmunol Photomed 2007;23:32-4.
[Google Scholar]
|
| 52. |
Sadick NS, Magro C, Hoenig A. Prospective clinical and histological study to evaluate the efficacy and safety of a targeted high-intensity narrow band UVB/UVA1 therapy for striae alba. J Cosmet Laser Ther 2007;9:79-83.
[Google Scholar]
|
Fulltext Views
11,242
PDF downloads
2,817





![[Table - 1]](#tbl_ijdvl_2016_82_1_1_172902_t1.jpg){kind=link}