
Translate this page into:
Targetoid bullous tinea corporis: Unusual presentation of a dermatophyte infection
Corresponding author: Dr. Shi Yu Derek Lim, Department of Dermatology, National Skin Centre, 1 Mandalay Road, Singapore 308205. derek.lim@mohh.com.sg
-
Received: ,
Accepted: ,
How to cite this article: Derek Lim SY, Lee JS, Chong WS. Targetoid bullous tinea corporis: Unusual presentation of a dermatophyte infection. Indian J Dermatol Venereol Leprol 2021;87:101-103.
Sir,
Bullous lesions in tinea are uncommon and are usually seen in the setting of tinea pedis. Commonly reported causative fungal pathogens are Trichophyton rubrum and Trichophyton mentagrophytes.1 We report a case of Microsporum canis causing targetoid bullous tinea corporis.
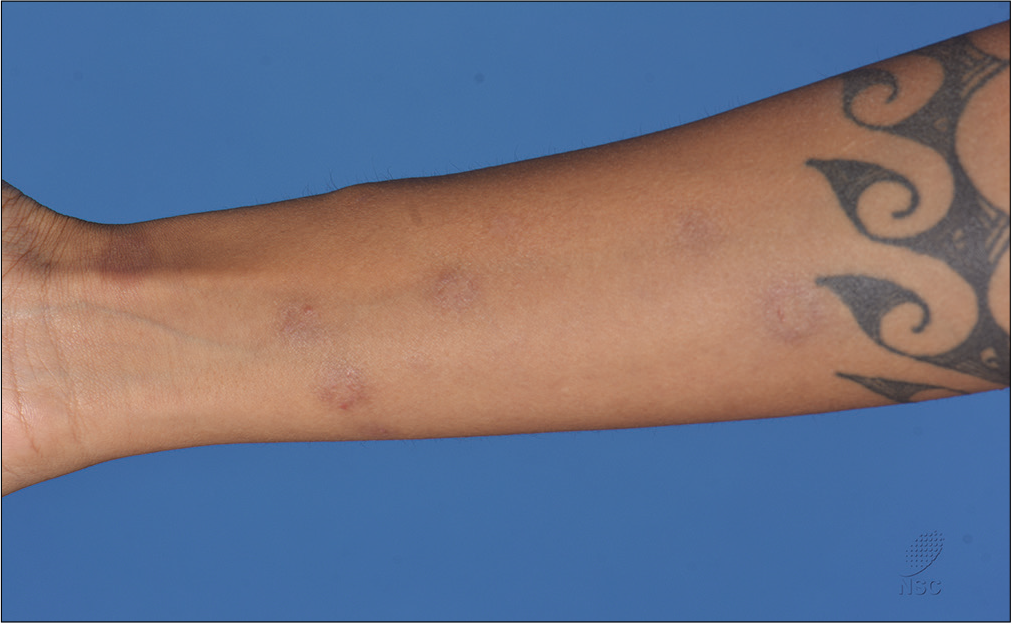
A 35-year-old woman gave a 6-day history of a generalised pruritic eruption involving the trunk and limbs. She had travelled to Kuantan, Malaysia and Bintan Island, Indonesia, in the past few weeks. One week prior to the onset of the rash, whilst in Kuantan, she had carried a stray kitten which scratched her on the neck. She reported no other contactants or medications prior to the eruption. She had no fever or mucosal involvement and was otherwise systemically well. Her past medical history was significant only for female pattern hair loss and alopecia areata, which was quiescent. On examination, multiple umbilicated targetoid papulovesicular lesions were seen over the neck, trunk, upper and lower limbs [Figure 1a-c]. The palms, soles, oral and conjunctival mucosae were not involved. She did not have any lymphadenopathy.

- Multiple umbilicated targetoid papulovesicular lesions over the neck and trunk

- Multiple umbilicated targetoid papulovesicular lesions over the neck, trunk, and upper limbs

- Close-up view of targetoid papulovesicular lesions over the right forearm
The differential diagnoses considered were erythema multiforme, syphilis, ecthyma, orf and cat scratch disease. A full blood count was unremarkable and rapid plasma reagin was negative.
Histology from the edge of a left forearm blister showed subcorneal neutrophils, spongiosis of the epidermis with neutrophilic exocytosis and prominent upper dermal oedema resulting in subepidermal pseudovesiculation, as well as septate fungal hyphae within the stratum corneum, which were seen on periodic acid–Schiff and Gomori methenamine silver stain [Figures 2a and b].
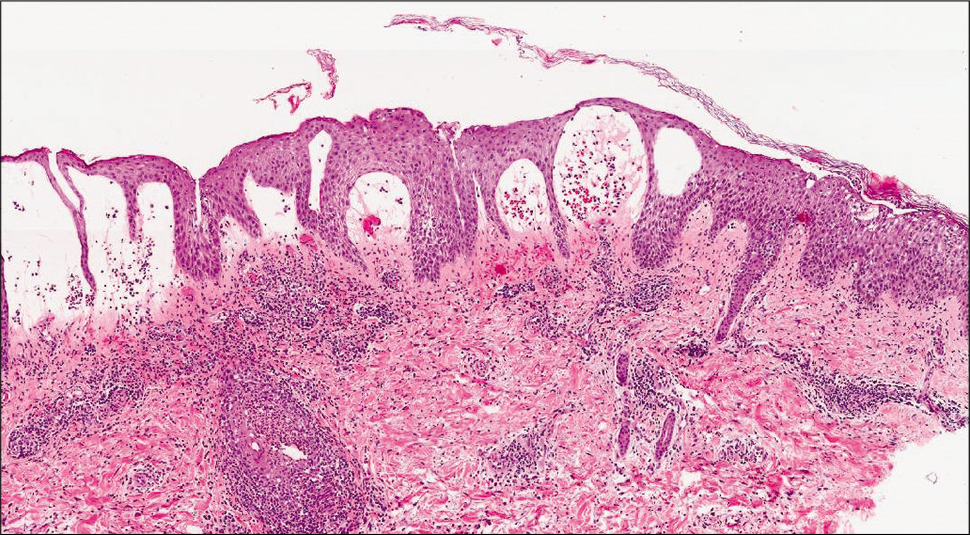
- Epidermal spongiosis with subcorneal neutrophils, and prominent upper dermal edema resulting in subepidermal pseudovesiculation (H and E, ×40)
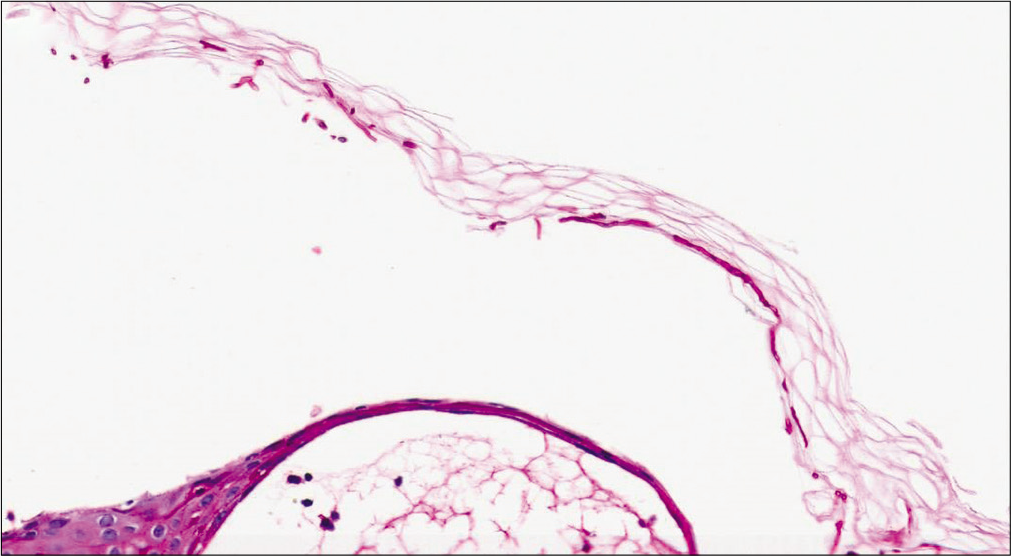
- Septate fungal hyphae within the stratum corneum (Periodic acid-Schiff stain, ×200)
She was diagnosed with bullous tinea corporis and commenced on oral terbinafine 250mg daily. Her lesions completely cleared in 3 weeks [Figures 3a and b]. Cultures from the biopsy later returned positive for M. canis.M. canis is a zoophilic fungus, which usually causes infection in dogs, cats, and other animals.2 The first case of M. canis causing bullous tinea was reported in 1993 and we found only 3 reports in the published literature.3 Our patient had a clear history of contact with a likely infected animal.

- Complete resolution of the patient’s lesions after 3 weeks of oral terbinafine
- Complete resolution of the patient’s lesions after 3 weeks of oral terbinafine
Bullous tinea corporis, owing to the rarity of its presentation, can be mistaken for a variety of dermatoses such as erythema multiforme, bullous allergic contact dermatitis and linear IgA bullous dermatosis. In
fact, in one reported case, the authors empirically started treatment with dapsone for linear IgA bullous dermatosis before a change in the morphology of the lesions prompted them to send samples for direct microscopy, which returned positive for hyphae.4
We hope that this report of targetoid bullous tinea corporis will encourage clinicians to consider a fungal aetiology in the differential diagnoses of generalised targetoid bullous lesions in contrast to the annular scaly plaques usually expected in tinea.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A case of bullous tinea pedis with dermatophytid reaction caused by Trichophyton violaceum. Mycoses. 2006;49:249-50.
- [CrossRef] [PubMed] [Google Scholar]
- In vitro activities of 15 antifungal drugs against a large collection of clinical isolates of Microsporum canis. Mycoses. 2019;62:1069-78.
- [CrossRef] [PubMed] [Google Scholar]
- Tinea corporis bullosa due to Microsporum canis mimicking linear IgA bullous dermatosis. Eur J Dermatol. 2012;22:805-6.
- [CrossRef] [PubMed] [Google Scholar]




