Translate this page into:
The effectiveness of adding low-level light therapy to minoxidil 5% solution in the treatment of patients with androgenetic alopecia
2 Skin and Stem Cell Research Center, Tehran University of Medical Sciences, Tehran, Iran
3 Department of Biostatistics and Epidemiology, Skin Diseases and Leishmaniasis Research Center, Health Faculty, Isfahan University of Medical Sciences, Isfahan, Iran
Correspondence Address:
Samaneh Mozafarpoor
Skin Diseases and Leishmaniasis Research Center, Department of Dermatology, Isfahan University of Medical Sciences, Isfahan
Iran
| How to cite this article: Faghihi G, Mozafarpoor S, Asilian A, Mokhtari F, Esfahani AA, Bafandeh B, Nouraei S, Nilforoushzadeh MA, Hosseini SM. The effectiveness of adding low-level light therapy to minoxidil 5% solution in the treatment of patients with androgenetic alopecia. Indian J Dermatol Venereol Leprol 2018;84:547-553 |
Abstract
Background: Androgenetic alopecia is the commonest type of alopecia affecting over half of men and women. Low-level light therapy is a new technique for stimulating hair growth in both genders.
Aims: To overcome the shortcomings of previous epidemiological studies and a lack of controlled clinical trials on the subject, this study compared the effectiveness of adding low-level light therapy to minoxidil topical solution in the treatment of androgenetic alopecia in patients presenting to two skin clinics in Isfahan, Iran during 2014–2015.
Materials and Methods: This clinical trial included 50 patients aged 17–45 presenting to Khorshid and Alzahra educational centers and skin diseases research center for androgenetic alopecia during 2014–2015. The patients were randomly divided into a control and a case group. The case group received topical minoxidil 5% solution plus low-level light therapy twice per day. The control group was given the same topical solution and a laser comb system that was turned off to act as a placebo. Changes in patients' hair density and diameter and its overall regrowth as well as their satisfaction with the treatment were assessed at months 0 (baseline), 3, 6, 9 and 12.
Results: The percentage of recovery from androgenetic alopecia and the patients' satisfaction with their treatment were significantly higher in the case group compared to the control group. The patients' mean hair density and diameter were found to be higher in the case group after the intervention compared to the control group.
Limitations: The study limitations included patient compliance, small sample size, patient insight due to novelty of the method and clinical judgement.
Conclusion: As a new method of treatment, low-level light therapy can help improve the percentage of recovery from androgenetic alopecia and increase patients' satisfaction with their treatment.
Introduction
Alopecia is a skin disorder affecting more than half of the world's population.[1] Androgenetic alopecia is the most common type of alopecia that affects over 50% of men aged over 40 and 75% of women aged over 65.[1],[2],[3],[4],[5] In genetically-predisposed individuals, androgenetic alopecia is often caused by androgens such as testosterone and its derivatives.[1] The most common techniques for the treatment of androgenetic alopecia include the use of topical minoxidil, the administration of Finasteride tablets and hair transplantation.[1],[2],[4],[6] Studies suggest that traditional therapies are only slightly effective in the treatment of this condition.[6] Patients who respond poorly to these common therapies and those who experience side-effects are always seeking more modern and suitable techniques to treat their condition.
Low-level light therapy is a new technique for stimulating hair growth in men and women that has recently been approved by the US food and drug administration. It is assumed to stimulate anagen phase re-entry in telogen hair follicles, prolong the duration of anagen phase, increase rates of proliferation in active anagen hair follicles and prevent premature catagen development. Most studies conducted on the effectiveness of low-level light therapy in the treatment of alopecia have had epidemiological problems such as lacking scientific rigor, the presence of confounding factors and inappropriate statistical analysis, which render their results unreliable. Given the lack of a randomized controlled clinical trial with an appropriate design on the subject, the present study was conducted to carry out a comparative assessment of the effectiveness of adding low-level light therapy to minoxidil topical solution for the treatment of alopecia in patients presenting to skin clinics in Isfahan, Iran during 2014–2015.
Materials and Methods
The present randomized double-blind controlled clinical trial was conducted in 2014–2015 on 17–45-year-old patients presenting to Khorshid and Alzahra educational centers and skin diseases research center for the treatment of androgenetic alopecia. The study protocol was approved by the Ethics Committee of Isfahan University of Medical Sciences, and all the participants signed written consent form for participation in the study.
The inclusion criteria consisted of at least 6 months history of hair loss or thinning without response to other commonly used treatments, having no other hair loss disorders, a Fitzpatrick skin type of 1–4, a Norwood–Hamilton grade of 3–6 for men and a Ludwig grade of 2–3 for women and having no history of finasteride and anti-androgen drugs' administration, such as cyproterone, spironolactone, ketoconazole and flutamide, topical estrogen, progesterone, tamoxifen, anabolic steroids, drugs potentially causing hypertrichosis, such as cyclosporine, diazoxide, phenytoin, oral glucocorticoids, and phenothiazines.
The study exclusion criteria consisted of having a history of hair transplantation or any condition affecting hair growth such as a connective tissue disease, inflammatory intestinal disease or certain endocrinopathies such as polycystic ovary syndrome, ovarian and adrenal tumors and hypothyroidism.
In this study, androgenetic alopecia was diagnosed clinically and based on the Ludwig and the Hamilton–Norwood scales and by rejecting other causes of hair loss. The study sample size was calculated as 50 according to the sample size equation (with a confidence interval of 95% and a statistical power of 80%) and taking into account a withdrawal of 10%. The participants were randomly divided into a control and a case group using a table of random numbers. To place patients in the treatment and control groups, randomization was performed by simple randomized sampling.
The case group received 20 drops of topical minoxidil 5% solution twice per day to use on their bald areas at home for six months plus 2–3 20-minute sessions of low-level light therapy (using LDU 8024PN/8024BN, made in Germany, with a 10-50 mw power and a 785-nm wavelength) per week for 24 weeks at Arman skin and hair center. The controls received only topical minoxidil 5% solution in the same manner as in the case group and were given a laser comb system that was switched off to act as a placebo. The number of low-level light therapy/laser comb treatment sessions was determined as 2–3 according to the study protocol, but the majority of patients took part two times per week in the course of study.
All the participants underwent three monthly hair counts at months 0 (i.e., at the beginning of the study), 3, 6, 9 and 12 of the study using a trichogram (hd-pro, bomtech electronics, made in South Korea). In addition to the demographic questionnaire, another questionnaire was designed to assess the side-effects of the medications used. The changes in hair density and diameter, overall hair regrowth and patient satisfaction were assessed. To assess the overall response to the treatment, the patients were divided into four subgroups based on their percentage of recovery and increased hair density, forming mild (less than 25% progress) to complete (at least 75% recovery) recovery groups. The participants were also visually monitored on a 5-point scale from “worse” to “perfect,” and their satisfaction was assessed from “low” to “high.” The treatment-giving physician who should be aware of the laser comb process was not blinded, but the investigator physician, who was a dermatologist and inspected the data, photos and improvement scales, was blinded.
Statistical analysis
The data were analyzed using SPSS. The quantitative data were expressed as mean ± standard deviation, and the qualitative data as frequency and percentage. The data obtained were compared using the paired t-test, the repeated measures analysis of variance (ANOVA) and the independent sample t-test. Given the significance level of 95%, all results with P values lower than 0.05 were considered statistically significant.
Results
No significant differences were observed between the control and case groups in terms of age (30.1 ± 5.7 vs. 30.4 ± 6.5 years; P = 0.9) and gender distribution or the male to female ratio (6.17 vs. 9.13; P = 0.29). Two patients in the case group and three in the control group did not complete the study due to moving out of the city or reluctance to continue in the study.
The percentage of recovery from androgenetic alopecia was similar in both groups 3 months after the intervention; however, compared to the controls, the case group revealed a significant increase in this percentage at 6, 9 and 12 months after the intervention (P < 0.001) [Table - 1].
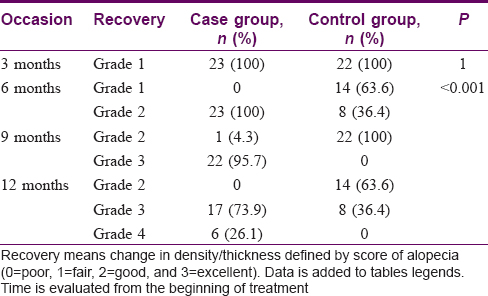
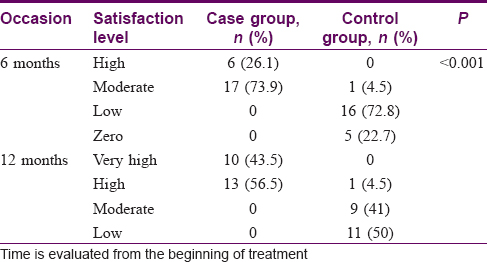
Nevertheless, a significant difference was observed between the two groups in terms of their satisfaction with the treatment (P < 0.001) [Table - 2].
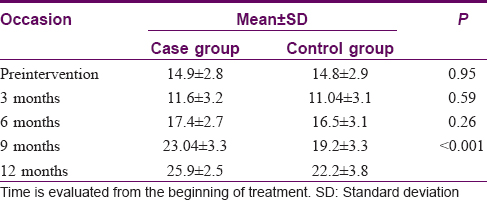
There were no significant differences between the groups in terms of their mean hair count before and 3 and 6 months after the intervention; however, the mean hair count was found to be significantly higher in the case group compared to in the controls 9 and 12 months after the intervention (P < 0.001). [Table - 3] and [Table - 4] present the mean hair density (i.e., hair count) on the vertical and frontoparietal areas of the head.
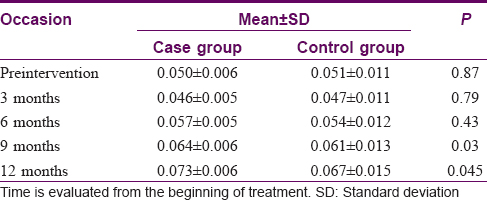
Similarly, there were no significant differences between the groups in their mean hair diameter before and 3, 6 and 9 months after the intervention; however, this variable increased significantly in the case group 12 months after the intervention (P = 0.045).
The mean increase in hair count was significantly higher in the case group compared to the control group (78.3% vs. 51.3%; P < 0.001). The mean increase in hair diameter was also significantly higher in the case group compared to the controls (45.4% vs. 32.3%; P = 0.002). Nevertheless, no significant differences were observed between the two groups in terms of side-effects such as headache (P = 0.35), itching (P = 0.44) and burning (P = 0.81), although the likelihood of developing erythema was significantly higher in the control group compared to the case group (5 vs. 1 cases; P = 0.04).
Discussion
The results obtained showed a significantly higher percentage of recovery from androgenetic alopecia in the case group compared to the control group, and the cases were generally more satisfied with their treatment compared to the controls. The mean hair count was significantly higher 9 and 12 months after the intervention in the case group compared to the control group [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4]. The mean hair diameter was significantly higher in the cases compared to the controls only 12 months after the intervention and not before [Figure - 5] and [Figure - 6]a-e]. The percentage of increase in hair count and hair diameter was significantly higher in the case group compared to the control group. The results obtained show that, as a relatively new technique, low-level light therapy can stimulate hair growth significantly in both men and women with androgenetic alopecia. This technique has recently been approved by the food and drug administration.[4] Offering this treatment to the public requires only the safety approval of the government and no further studies are required on its effectiveness,[5] especially because scientists have known for a long time that red or near infrared light stimulate tissue repair and the discovery of laser in the 1960s generated a greater interest in its use as a therapeutic method.
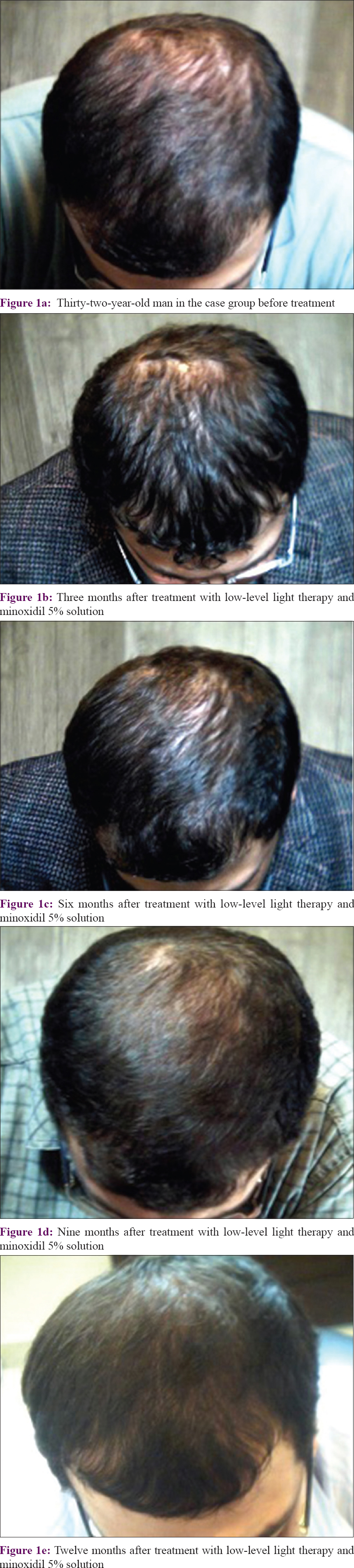 |
| Figure 1: |
 |
| Figure 2: The patients trichogram at the same intervals |
 |
| Figure 3: |
 |
| Figure 4: The trichogram at the same intervals |
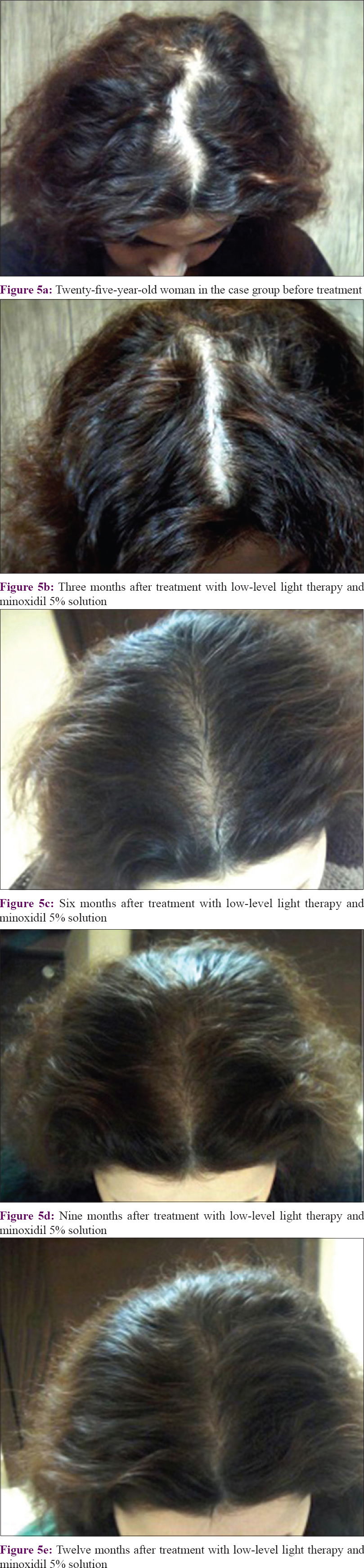 |
| Figure 5: |
 |
| Figure 6: The trichogram at the same intervals |
Many studies have been conducted to date for understanding the different theories proposed for the biological mechanisms by which light therapy affects hair growth. Some studies have focused on the hypertrichosis resulting from the changes in the follicles from the telogen (rest) phase to the anagen (active) phase or the terminal changes in the vellus follicles.[4],[6] Moreover, stimulating proliferation can at least be considered an initiative mechanism in light therapy. Given that both the reconstructive regeneration occurring in the process of wound healing and the physiological regeneration occurring in the hair growth cycle require cell proliferation, it is possible that the stimulating effect of low-level light on hair growth can be achieved through a direct or indirect increase in the proliferative intra matrix activity of the epithelial hair follicles.[3] The hair growth capacity of laser therapy was discovered by accident in 1967. Ever since Kim et al. used laser on the shaved back of a rat to treat cancer,[7] different studies have been conducted to assess the effect of laser therapy on the treatment of alopecia, especially the androgenetic and areata subtypes.[1],[4],[5],[7],[8],[9] A study conducted in 2013 on men with androgenetic alopecia showed a significantly higher hair count after laser therapy.[8] Another study conducted in 2013 on men and women with androgenetic alopecia showed a greater hair density and diameter in cases and reported no side-effects of this treatment.[2] Another study conducted among men with androgenetic alopecia reported an increase in hair density after laser therapy and a higher patient satisfaction of 83%.[7] Christie et al. examined the effect of laser therapy on hair growth in men and women with androgenetic alopecia and reported that laser therapy can have significantly positive effects on hair growth among these patients.[10] Most studies conducted to date for assessing the effectiveness of low-level light therapy in the treatment of alopecia have failed to properly control the role of confounding factors or have had problems in their statistical analysis of the data, which render their results unreliable. The present study was, therefore, conducted to overcome the weaknesses of previous studies on the subject and can be considered a scientific clinical trial of the effectiveness of low-level light therapy in the treatment of androgenetic alopecia.
The results obtained show that, as a new technique, low-level light therapy can effectively improve the percentage of recovery from androgenetic alopecia and increase patients' satisfaction with the treatments received for hair regrowth.
Limitations
The study limitations included problems of patient complaince, small sample size, patient insight due to novelty of the method and clinical judgement.
Conclusion
As a new method of treatment, low-level light therapy can help improve the percentage of recovery from androgenetic alopecia and increase patients' satisfaction with their treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Skin Diseases and Leishmaniasis Research Center, Research Deputy of Isfahan University of Medical Sciences Isfahan, Iran. (mui.ac.ir).
Conflicts of interest
There are no conflicts of interest.
| 1. |
Avci P, Gupta GK, Clark J, Wikonkal N, Hamblin MR. Low-level laser (light) therapy (LLLT) for treatment of hair loss. Lasers Surg Med 2014;46:144-51.
[Google Scholar]
|
| 2. |
Kim H, Choi JW, Kim JY, Shin JW, Lee SJ, Huh CH, et al. Low-level light therapy for androgenetic alopecia: A 24-week, randomized, double-blind, sham device-controlled multicenter trial. Dermatol Surg 2013;39:1177-83.
[Google Scholar]
|
| 3. |
Leavitt M, Charles G, Heyman E, Michaels D. HairMax laser Comb laser phototherapy device in the treatment of male androgenetic alopecia: A randomized, double-blind, sham device-controlled, multicentre trial. Clin Drug Investig 2009;29:283-92.
[Google Scholar]
|
| 4. |
Ghanaat M. Types of hair loss and treatment options, including the novel low-level light therapy and its proposed mechanism. South Med J 2010;103:917-21.
[Google Scholar]
|
| 5. |
Gupta AK, Daigle D. The use of low-level light therapy in the treatment of androgenetic alopecia and female pattern hair loss. J Dermatolog Treat 2014;25:162-3.
[Google Scholar]
|
| 6. |
Rangwala S, Rashid RM. Alopecia: A review of laser and light therapies. Dermatol Online J 2012;18:3.
[Google Scholar]
|
| 7. |
Kim S, Park M, Lee C. Phototherapy of androgenetic alopecia with low level narrow band 655-nm red light and 780-nm infrared light. J Am Acad Dermatol 2007;56:AB112.
[Google Scholar]
|
| 8. |
Lanzafame RJ, Blanche RR, Bodian AB, Chiacchierini RP, Fernandez-Obregon A, Kazmirek ER, et al. The growth of human scalp hair mediated by visible red light laser and LED sources in males. Lasers Surg Med 2013;45:487-95.
[Google Scholar]
|
| 9. |
Avram MR, Leonard RT Jr., Epstein ES, Williams JL, Bauman AJ. The current role of laser/light sources in the treatment of male and female pattern hair loss. J Cosmet Laser Ther 2007;9:27-8.
[Google Scholar]
|
| 10. |
Christie A, Jamtvedt G, Dahm KT, Moe RH, Haavardsholm EA, Hagen KB, et al. Effectiveness of nonpharmacological and nonsurgical interventions for patients with rheumatoid arthritis: An overview of systematic reviews. Phys Ther 2007;87:1697-715.
[Google Scholar]
|
Fulltext Views
15,366
PDF downloads
3,065





![[Table - 1]](#tbl_ijdvl_2018_84_5_547_236696_t7.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2018_84_5_547_236696_t8.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2018_84_5_547_236696_t9.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2018_84_5_547_236696_t10.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2018_84_5_547_236696_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_5_547_236696_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_5_547_236696_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_5_547_236696_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2018_84_5_547_236696_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2018_84_5_547_236696_f6.jpg){kind=link}