Translate this page into:
The rationale of ideal pulse duration and pulse interval in the treatment of steatocystoma multiplex using the carbon dioxide laser in a super-pulse mode as opposed to the ultra-pulse mode
2 Department of Pathology, PGIMER and Dr. RML Hospital, Delhi, India
Correspondence Address:
Kabir Sardana
Department of Dermatology, PGIMER and Dr. RML Hospital, Delhi
India
| How to cite this article: Dixit N, Sardana K, Paliwal P. The rationale of ideal pulse duration and pulse interval in the treatment of steatocystoma multiplex using the carbon dioxide laser in a super-pulse mode as opposed to the ultra-pulse mode. Indian J Dermatol Venereol Leprol 2020;86:454-456 |
Sir,
Steatocystoma multiplex is a clinical condition characterized by numerous dermal cysts that have their origin in the pilosebaceous duct. Various treatment modalities have been used including surgery, carbon dioxide laser, radiofrequency, oral isotretinoin and cryotherapy.[1] The ultimate goal is to remove the lesion without adverse effects. Aggressive ablation with a continuous wave carbon dioxide laser can cause thermal damage and we elucidate the use of the super-pulsed mode of carbon dioxide laser, tweaking the settings to effect a successful ablation with minimal sequelae and lack of recurrence even after 24 months of follow-up.
A 60-year-old man presented to the dermatology outpatient department at Dr. Ram Manohar Lohia hospital, Delhi, with multiple, asymptomatic, skin-colored papules and nodules on the upper chest, which started in his adolescence and gradually increased in number. Examination revealed translucent, skin-colored to yellow dermal cysts with a smooth surface, size varying from 0.05–0.1 cm, present bilaterally symmetrically on the upper chest [Figure - 1]a. Histopathological examination was consistent with steatocystoma multiplex and revealed a cyst in the dermis with sebaceous glands embedded in its wall [Figure - 1]b and [Figure - 1]c. A decision was taken to treat some of the lesions to assess treatment response, sequelae and relapse before treating all the lesions. The carbon dioxide laser (ultra-dream pulse surgical carbon dioxide laser system, DS-40U, Daeshin Enterprise Co., Ltd., Korea) was set to super-pulse mode “C” with a pulse width of 1400 μs at laser power 2 watts and repeat time of 50 ms. The first pass was directed at the center of a lesion, using a 1 mm spot size in the super-pulsed mode and after that once the cyst was visualized, gentle pressure in horizontal direction (inward) was used to extrude the contents [Figure - 2]a and [Figure - 2]b. Later a defocused laser pass was made on the cyst lining. For smaller lesions, the whole lesion was vaporized in total. The patient was advised to apply topical antibiotic cream for 7 days and lesions were allowed to heal by secondary intention. The patient was followed up for 24 months and no recurrence was seen [Figure - 3].
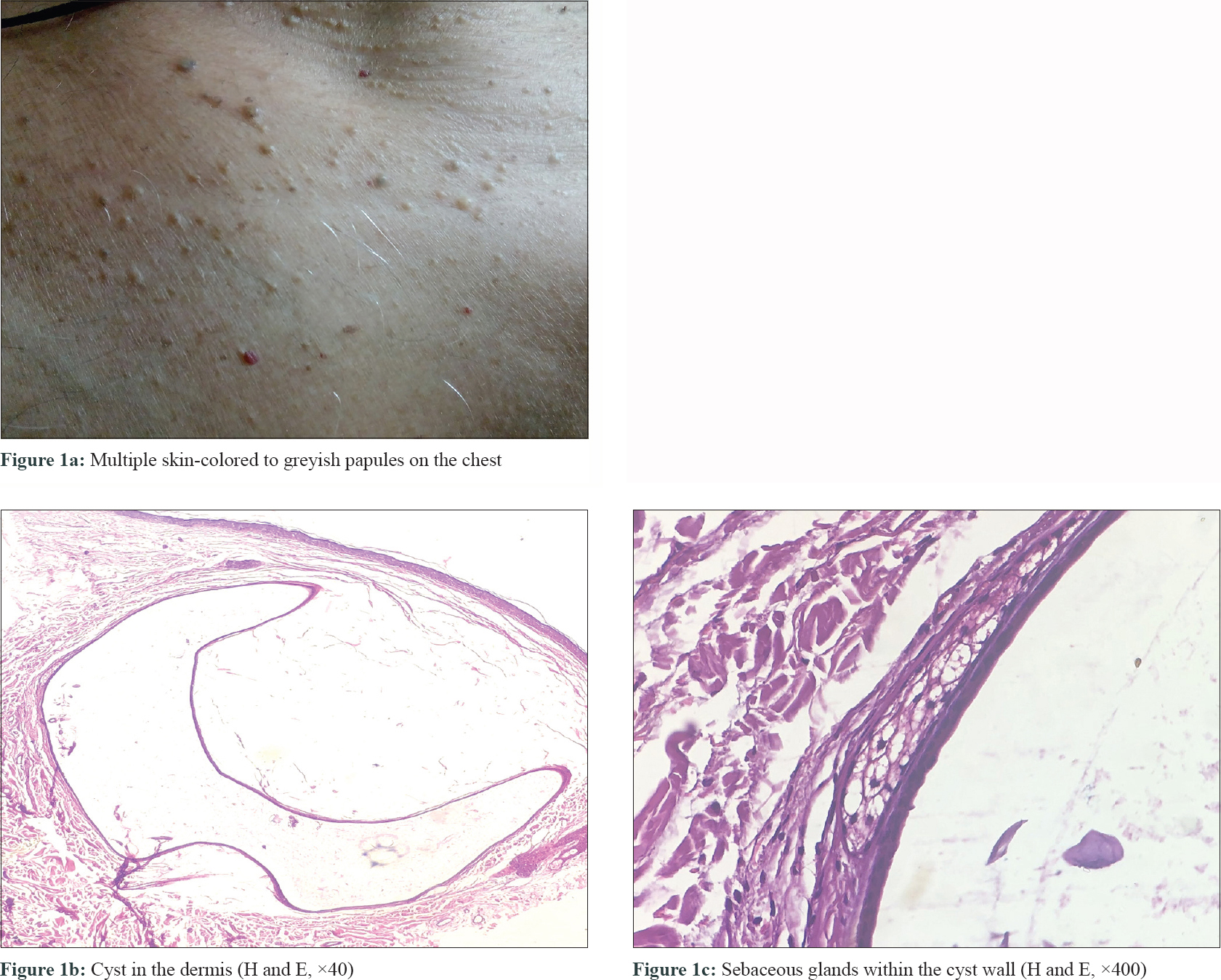 |
| Figure 1: |
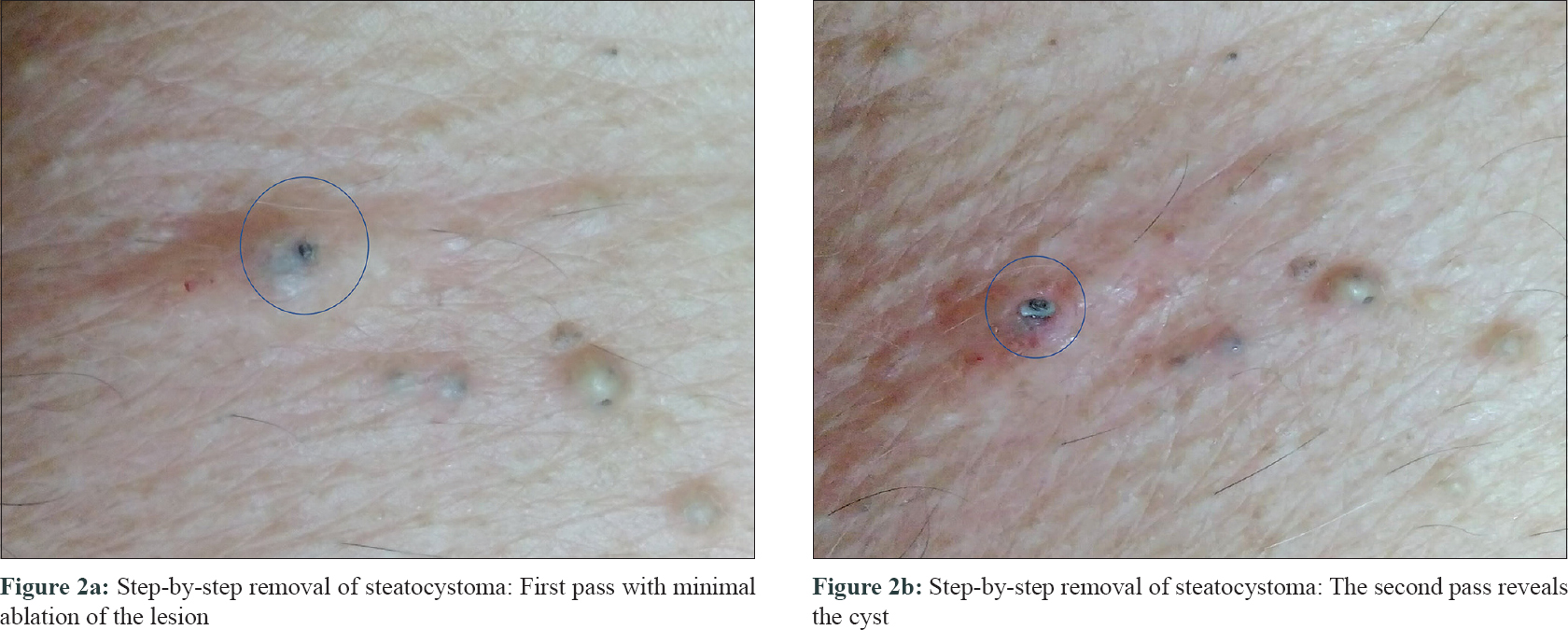 |
| Figure 2: |
 |
| Figure 3: Lack of recurrence and excellent cosmesis 24 months after the session |
Steatocystoma multiplex has been treated using various techniques: cryosurgery, aspiration, surgical excision, incisional techniques using blade or radio-frequency as well as the carbon dioxide laser but scarring and recurrence of the lesions are the major complications observed.[2] Among the ablative lasers, the erbium; yttrium aluminum garnet laser has also been used but possibly because of its minimal coagulative potential, prompt recurrence has been reported.[3] Thus, among lasers, the carbon dioxide laser remains the preferred option, with some singular advantages including the ability to treat multiple lesions during a single treatment session, a low percentage of recurrence and good cosmesis.[4]
The basic skill of using the ablative laser involves tweaking the settings, with the aim of avoiding residual thermal damage for which ideally a pulse duration of <1 ms is needed. The residual thermal damage is visually assessed by the degree of carbonization by using the ultra-pulse mode. However, in the present study, we used the super-pulse mode and it is crucial to appreciate the rationale of the settings used in our case to reduce thermal damage and maximize the results. It is believed that, in real-life scenarios, a super-pulse carbon dioxide laser can lead to comparable results as the ultra-pulse mode and most good super-pulsed lasers can be used with excellent cosmesis, if the pulse duration of 1–1.7 ms is used with a 50 ms pulse interval.[5] The logic of using the super pulse mode is based on the argument of Venugopalan et al. who surmised that for single pulses over a range of 0.25–10 ms, there were no significant increase in residual thermal damage for fluences of 1, 3, and 10 J/cm2.[6] Thus the super-pulse mode of the carbon dioxide laser can be used with minimal thermal damage, if short pulses are generated as this ensures spatial confinement of thermal injury and lowering of the ablation threshold. It has also been shown that the depth of the incision increases with increasing fluences and it decreases with increasing the pulse interval while the tissue carbonization increases with decreasing the pulse interval. At a pulse interval of 50 ms, the laser thus produced no visible signs of carbonization or residual thermal damage and the settings that we used corresponded to a depth and width of 1 mm which was appropriately aligned to ablate the lesions of steatocystoma. In addition, the lack of carbonization and residual thermal damage with a pulse duration of 1–1.7 ms has been validated by Walsh et al. who reported no charring after soft-tissue incision at pulse durations less than 2 ms.[7] Thus, our settings of 1.4 ms pulse duration and 50 ms of pulse interval was used, extrapolating the seminal data on the intricacies of super-pulsed ablation[6],[7] and can be used to achieve the dual purpose of effective ablation and minimal thermal damage in most ablative indications including steatocystoma.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal the identity, but anonymity cannot be guaranteed.
Acknowledgement
Dr. Pushpanjali Behera, Senior Resident, Department of Pathology, PGIMER and Dr. RML Hospital, Delhi, India.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Kamra HT, Gadgil PA, Ovhal AG, Narkhede RR. Steatocystoma multiplex-a rare genetic disorder: A case report and review of the literature. J Clin Diagn Res 2013;7:166-8.
[Google Scholar]
|
| 2. |
Düzova AN, Sentürk GB. Suggestion for the treatment of steatocystoma multiplex located exclusively on the face. Int J Dermatol 2004;43:60-2.
[Google Scholar]
|
| 3. |
Mumcuoglu CT, Gurel MS, Kiremitci U, Erdemir AV, Karakoca Y, Huten O. Er: Yag laser therapy for steatocystoma multiplex. Indian J Dermatol 2010;55:300-1.
[Google Scholar]
|
| 4. |
Rossi R, Cappugi P, Battini M, Mavilia L, Campolmi P. CO2 laser therapy in a case of steatocystoma multiplex with prominent nodules on the face and neck. Int J Dermatol 2003;42:302-4.
[Google Scholar]
|
| 5. |
Sardana K, editor. Ablative lasers. In: Lasers and Energy Devices in Aesthetic Dermatology Practice. 1st ed. New Delhi: Jaypee Brothers Medical Publishers; 2019. p. 62-3.
[Google Scholar]
|
| 6. |
Venugopalan V, Nishioka NS, Mikic BB. The effect of laser parameters on the zone of thermal injury produced by laser ablation of biological tissue. J Biomech Eng 1994;116:62-70.
[Google Scholar]
|
| 7. |
Walsh JT Jr., Flotte TJ, Anderson RR, Deutsch TF. Pulsed CO2 laser tissue ablation: Effect of tissue type and pulse duration on thermal damage. Lasers Surg Med 1988;8:108-18.
[Google Scholar]
|
Fulltext Views
6,301
PDF downloads
2,624





![[Figure - 1]](#fig_ijdvl_2020_86_4_454_283648_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_4_454_283648_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_4_454_283648_f3.jpg){kind=link}