Translate this page into:
Topical betamethasone for prevention of radiation dermatitis
2 Department of Medical physics, Nemazee Hospital, Shiraz University of Medical Sciences, Shiraz, Iran
3 Department of Dermatology, Nemazee Hospital, Shiraz University of Medical Sciences, Shiraz, Iran
4 Department of Pharmacology, Nemazee Hospital, Shiraz University of Medical Sciences, Shiraz, Iran
Correspondence Address:
Shapour Omidvari
Department of Radiation Oncology, Nemazee Hospital, Shiraz University of Medical Sciences, Shiraz
Iran
| How to cite this article: Omidvari S, Saboori H, Mohammadianpanah M, Mosalaei A, Ahmadloo N, Mosleh-Shirazi MA, Jowkar F, Namaz S. Topical betamethasone for prevention of radiation dermatitis. Indian J Dermatol Venereol Leprol 2007;73:209 |
Abstract
Background: Although acute radiation dermatitis (ARD) is a common side-effect of radiotherapy (RT), currently there is no general consensus about its prevention or treatment of choice. Aims: The purpose of this study was to investigate whether prophylactic use of topical betamethasone 0.1% can prevent ARD caused by chest wall irradiation. Methods: Fifty-one patients who underwent modified radical mastectomy for breast cancer and were going to receive RT, were randomly assigned to receive topical betamethasone 0.1%, petrolatum or none during RT. The frequency and severity of ARD (measured using Radiation Therapy Oncology Group acute radiation morbidity scoring criteria) were recorded at the end of each week during RT and two weeks after its completion. Clinical outcomes were analyzed by relevant statistical methods. Results: All patients developed some degree of ARD, the frequency and severity of which increased with time and reached the maximum at the end of the seventh week for all groups. Patients receiving betamethasone had less severe ARD than the other two groups throughout the course of the study, but this difference was significant only at the end of the third week (p =0.027). No significant difference was observed between the petrolatum and control arms. Conclusion: Prophylactic and ongoing use of topical betamethasone 0.1% during chest wall RT for breast cancer delays occurrence of ARD but does not prevent it. Petrolatum has no effect on the prevention of ARD in these patients.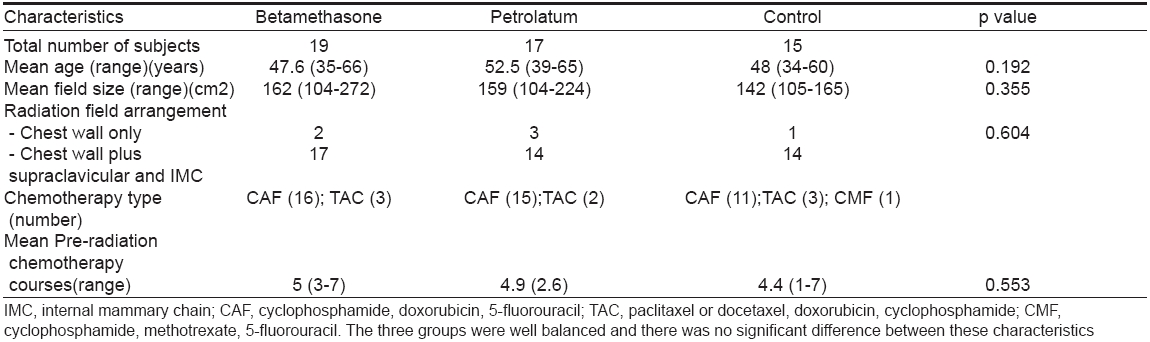

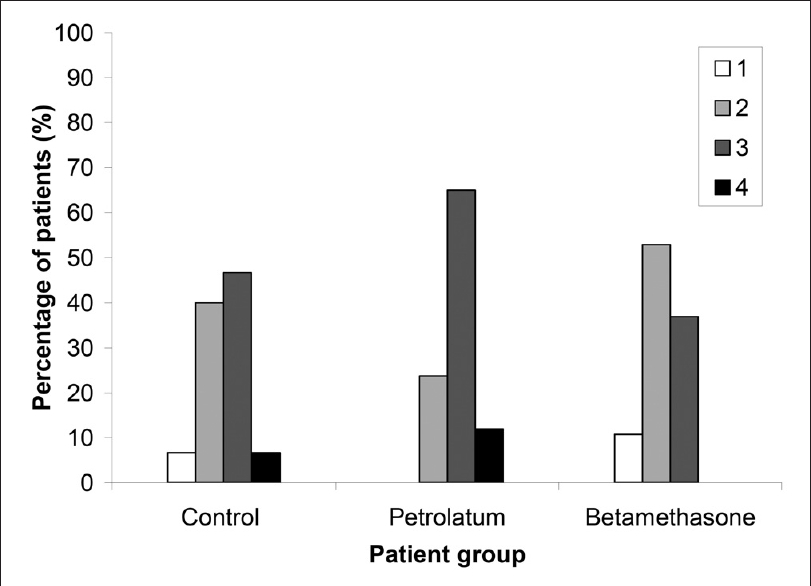 |
| Figure 3: Frequencies of the maximum observed ARD grade for each arm of the study |
|
| Figure 3: Frequencies of the maximum observed ARD grade for each arm of the study |
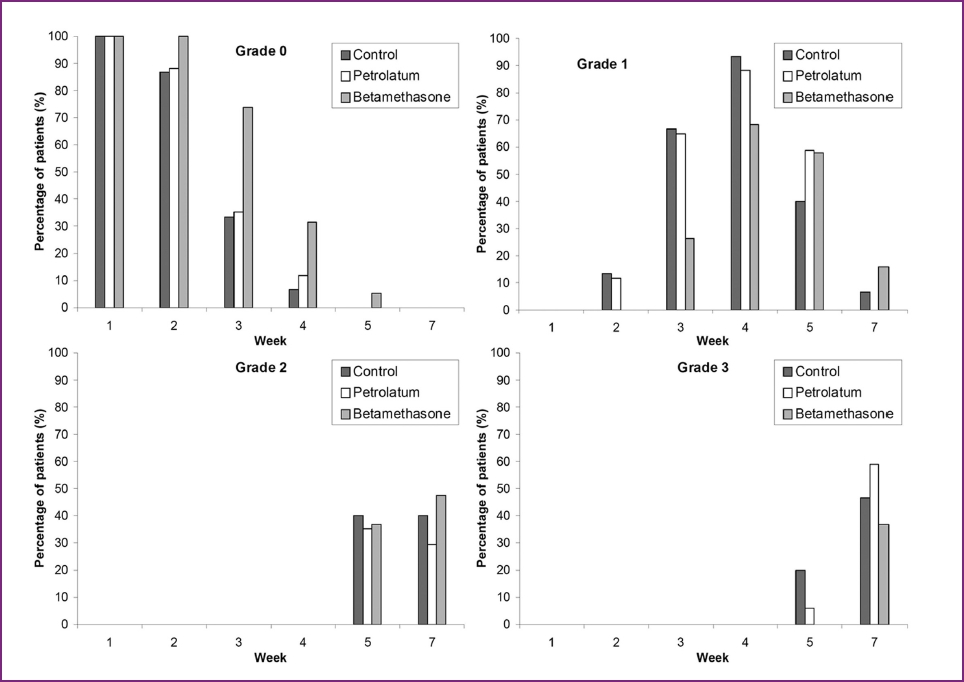 |
| Figure 2: Observed frequencies of radiation dermatitis grades 0 to 3 at each recorded time point. Additionally, Grade 4 ARD occurred only at seventh week (6.4%, 11.8% and 0% for the control, petrolatum and betamethasone arms respectively) |
|
| Figure 2: Observed frequencies of radiation dermatitis grades 0 to 3 at each recorded time point. Additionally, Grade 4 ARD occurred only at seventh week (6.4%, 11.8% and 0% for the control, petrolatum and betamethasone arms respectively) |
 |
| Figure 1: Mean weekly clinical dermatitis scores |
|
| Figure 1: Mean weekly clinical dermatitis scores |
Radiotherapy (RT) is a common modality in cancer treatment and more than 50% of affected patients will eventually receive some form of RT as definite, preoperative, postoperative or palliative treatment. [1],[2],[3] A common side-effect of external RT is acute radiation-induced skin toxicity, [1],[2],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14] which occurs in at least 87% of irradiated patients [1],[7],[15],[16] with unfavorable effects on the patients′ quality of life and may cause cessation of RT or prolongation of its course, [2],[4],[5],[7],[12],[15],[17] with possible negative effects on treatment outcome. [4],[18] General preventive measures for acute radiation dermatitis (ARD) include washing with mild soap and keeping the area clean and dry, wearing loose-fitting clothes made of natural fibers and protecting the RT field from further physical or chemical irritants such as ultraviolet light. [1],[2],[7],[15],[19],[20] Many different topical agents have also been evaluated for treatment or prophylaxis of ARD. These include plant-based treatments (such as Aloe Vera and Calendula), petrolatum-based emollients, trolamine-containing formulation (Biafine), dexpanthenol-containing formulation (Bepanthen), corticosteroids, sucralfate cream and many others. All these medications had variable degrees of success in randomized and non-randomized clinical trials. [1],[2],[4],[5],[6],[7],[8],[9],[10],[19],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30],[31],[32],[33],[34],[35],[36],[37],[38],[39],[40] Antioxidants (such as ascorbic acid) did not show any significant effect. [41],[42]
Because of the lack of general consensus for prevention and treatment of these complications [4],[5],[7],[33] and variable results from clinical trials and because these acute toxicities may have profound effects on the patients′ quality of life and also may compromise treatment outcome, this area of investigation is an open one and further studies are clearly needed. [1],[4],[5],[7],[9],[14],[15],[18],[24],[32]
This study was designed essentially to evaluate the prophylactic effect of topical betamethasone 0.1% on ARD. Breast cancer is one of the most common cancers in women [5] and post-mastectomy chest wall provides an excellent model to evaluate skin toxicities; [6] so we planned a study to assess prophylactic use of topical betamethasone 0.1% in this group of female patients. We also used petrolatum as an emollient to simulate emollient effects of the betamethasone base. In addition, we had a control group who received neither type of the two topical therapies.
Methods
Eligible patients were female patients who underwent modified radical mastectomy for Stage II or III pathologically proved breast cancer and in addition to surgery and chemotherapy, needed RT. Patients had to be in the 20-70 years range, without history of previous RT, confirmed diabetes mellitus or systemic connective tissue disease. Patients who were receiving concurrent chemotherapy and radiation or were on systemic corticosteroids were excluded. Total radiation dose (50Gy to chest wall with or without irradiation of supraclavicular-axillary region and internal mammary chain) and fractionation (2Gy per day in a single fraction, five days a week) were the same for all patients. All patients were treated with the same machine, energy and setup (ipsilateral arm up and face towards contralateral breast).
In our planning, RT field arrangement for these patients included post-mastectomy chest wall for all patients and supraclavicular-axillary and internal mammary chain for most of them; a few patients received RT to chest wall only. Chest wall field arrangement for the patients included the area between the internal mammary chain field (or midsternal line) medially, midaxillary line laterally, two centimeters below the contralateral inframammary fold inferiorly and supraclavicular-axillary field (or a line horizontally drawn from angle of Louis to axilla) superiorly.
Our routine planning for chest wall irradiation uses superficial X-rays (Siemens Stabilipan, 120kV, 10mA, 2mm Al filtration, 4mm Al half-value layer). The supraclavicular-axillary and internal mammary chain fields were delivered on the same days using a cobalt 60 unit. Although the use of superficial X-rays may cause more severe acute and late skin toxicities on chest wall than other techniques such as electron therapy or tangential fields with high energy photons and bolus, we use this technique because of limited electron facilities. In addition, our local control rates in the chest wall with this technique are quite good, although these patients develop both acute (ARD) and late (pigmentation changes and telangiectasias) toxicities more frequently (unpublished data). More than 90% of the patients treated with this approach develop Grade II or higher ARD by the end of the radiation course or thereafter. Preliminary statistical analysis showed that for a 50% reduction in severe dermatitis at the end of RT with 80% power and 95% confidence interval, we needed at least 15 patients in each arm. Then we planned the study for a total number of 56-60, with an estimated 25-30% of patients being excluded from the evaluation or quitting.
During a three-month period from August 2005 to October 2005, 58 eligible patients were randomly assigned to receive petrolatum, betamethasone 0.1% or none. Because petrolatum may have some (adverse or protective) effect on radiation-induced skin toxicity, the third group (control) was recruited. Those who used topical agents received clear verbal instructions regarding the application of the drug in the beginning of randomization and weekly during observation period and those who did not use the agents properly were excluded from the study. They had to use the agent twice daily from the first day of RT to two weeks after its completion. They were also asked to use the same volume of formulation on each application and to clean the radiation field before each fraction of radiation.
Randomization was computer-based and two blinded groups (for both the patients and the assessing physician) were those who received petrolatum and betamethasone. Written consent was obtained from all the patients before randomization. The two topical agents were placed in 50g jars of identical appearance, each with a label containing the patient name and randomization code only. Each patient received four to six jars, depending on the field size and the calculated volume of formulation. Application of the topical agents and evaluation of dermatitis were confined to the chest wall field only, because of its greater susceptibility to severe ARD than the other two fields in our technique.
At the end of the first, second, third, fourth and fifth week of RT and two weeks following its completion, all patients were assessed by the same radiation-oncologist and their dermatitis grade measured using Radiation Therapy Oncology Group (RTOG) acute radiation morbidity scoring criteria for skin [Table - 1] and recorded separately. We used this scoring system because it is fully clinical rather than pathologic or physiologic, which makes it easier to apply.
Results
Fifty-eight patients entered randomization. Seven patients failed to complete the study course or were excluded because of declining to participate, new onset of diabetes mellitus and prolonged radiation course due to other causes (such as zona), leaving 51 statistically evaluable cases at the end of the study. Of these, 19 were in the betamethasone group, 17 in the petrolatum group and 15 in the control arm.
Statistical analysis was done using non-parametrical tests (Kruskal-Wallis test and Friedman test). The analysis showed that these three groups were well balanced in regard to patient age, RT field size and field arrangement (chest wall field only versus chest wall plus supraclavicular-axillary and internal mammary chain) and type and number of chemotherapy courses prescribed before RT [Table - 2]. None of the patients had skin folds or intertrigo sites in the RT field because of the surgical technique and patient positioning.
[Figure - 1] shows the mean ARD grade at the different observation time points for each group. This measure was significantly increasing over the observation time for all groups and was lower for betamethasone receiving patients throughout the study, but significant difference was observed only at the end of the third week (p =0.027). [Figure - 2] shows the observed frequencies of different ARD grades at each recorded time point. It can be seen that ARD occurs later in the observation period for betamethasone-receiving patients and low-grade ARD (Grades 0 and 1) are more frequent in the early phases in this group, but later on both low- and high-grade ARD occur with comparable frequencies in the three arms.
At the end of the third week, only 26.3% of the betamethasone group developed Grade I dermatitis, compared with 64.7% and 66.7% in the emollient and control arms, respectively. Chi square and Kruskal-Wallis tests revealed that this difference was statistically significant (p = 0.027). At the end of the seventh week, which was also the end of the topical treatment and the last evaluation for dermatitis, 15.8% of the betamethasone group had only Grade I dermatitis but this rate was 6.7% for the control group. All petrolatum-receiving patients developed Grade II or higher ARD. At the same time, all patients had some degree of ARD; although betamethasone-receiving patients had lower mean dermatitis grade than the other two arms, this difference did not reach significance but approached it (p=0.055).
Throughout the study, the frequency and mean severity of ARD in the petrolatum and control arms were comparable and we did not find any significant difference between them at any time in the evaluation period.
[Figure - 3] shows the frequency of the maximum observed ARD grade for each arm of the study. Betamethasone-receiving patients had lower maximum ARD grades than the other two groups but this difference did not reach significance. In general, we found that the severity of ARD in the betamethasone group was less than the other two arms at any time during the study, but this was significant only at the end of the third week. We also found that the frequency of RD early in the course of RT (up to the third week) was lower for the betamethasone group than the other arms; but, later in the observation period, both the severity and frequency of RD were comparable for all three arms. There was no statistically significant difference between the petrolatum and control arms throughout the study.
Discussion
Acute radiation dermatitis is a frequent side-effect of fractionated external RT which has unfavorable effects on patients′ quality of life and may cause cessation or prolongation of radiation period with subsequent possible effects on antitumoral activity. Radiation-induced skin toxicities can be classified as acute and delayed complications. [1],[2],[11] Acute radiation-induced skin toxicities include erythema, edema, dry and wet desquamation, ulceration, necrosis and hemorrhage. [1],[2],[4],[7] These may be accompanied by itching and/or pain [2],[4],[7],[21] and are related to a variety of patient- and treatment-related factors including site of irradiation, RT dose and schedule, RT modality and energy and RT field size. Patient′s skin color is not a proved risk factor but several other factors are believed to be associated with more severe and more frequent radiation-induced skin toxicities; these include extreme age, existence of skin folds and intertrigos in the radiation field, diabetes mellitus, poor nutritional status of the patient, systemic connective tissue diseases (especially scleroderma), concurrent chemoradiation and further physical or chemical irritants to the irradiated area. [1],[2],[4],[7],[11],[15],[22] Therefore, many different agents have been evaluated as prophylactic measures to reduce these skin toxicities, but most studies resulted in inconsistent and non-reproducible results.
Early trials using topical corticosteroids for prevention of ARD were generally unsuccessful. Potera ME and coworkers found no statistically significant difference between 0.2% hydrocortisone and placebo in a cohort of 19 patients who received RT to chest wall, abdomen, head and neck. Their patients used hydrocortisone to one half of the field and placebo to the other half, beginning two weeks after the initiation of RT to three weeks after its completion. There was no control group. Acute skin response, symptoms of the ARD and late effects of RT were comparable in the two arms. [29]
Lack of preventive effect of local corticosteroids in the early trials is attributed to the use of less potent corticosteroids, occurrence of "break through phenomenon", variations in the local corticosteroid administration, heterogeneity of patients and radiation schemes, subjective evaluation methods and self-control approach. [4],[7]
More recent trials show more consistent results in favor of reduced ARD with the use of topical corticosteroids. In a double-blind, randomized study of 49 breast cancer patients, Asa Bostrom and colleagues found that topical mometasone furoate (MMF), a potent corticosteroid cream, can significantly reduce ARD over emollient. They used MMF or emollient from the start of radiation to three weeks after its termination. Their patients underwent breast-conserving surgery and were treated by tangential 5MV photon beam RT to breast parenchyma. Quality of life scores were similar it the two groups. [4] In another randomized trial, M. Schmuth and associates found similar results in favor of prophylactic and ongoing use of topical 0.1% methylprednisolone during RT. [5]
This protective effect of corticosteroids seems to be related to their anti-inflammatory properties. [4],[5] Although there are some concerns about long-term use of topical corticosteroids, short-term observations did not show any increase in the rate of telangiectasias or skin atrophy. Also, the risk of suppression of the pituitary-adrenal axis is reported not to be considerable. [4]
Our study showed that topical betamethasone 0.1% delays occurrence of ARD in breast cancer patients who are receiving radiation to chest wall but does not prevent it. So, this study provides some support to the prophylactic use of local betamethasone 0.1% for preventing or ameliorating ARD. We also found that petrolatum has no effect on the prevention of radiation-induced acute dermatitis.
We acknowledge the possible drawbacks of this study. Chest wall irradiation for breast cancer with low-energy photons is not a widely used approach, but because it can induce more severe and more frequent skin toxicities than electron therapy or tangential photon fields, it can serve as an excellent model to evaluate preventive or therapeutic options for ARD. It must be emphasized that the main objective of this study is to evaluate possible preventive effect of the drug and not to assess therapeutic efficacy of the radiation technique.
The lack of statistically significant differences between the three arms in much of the observation period may be due to the relatively small number of patients, although the observed frequencies of higher-grade ARD were lower for the betamethasone group throughout the study. Also, we had a short post-radiation observation period and each patient was assessed just once after completion of RT. We had to design such a relatively short time evaluation scheme because it was not possible for most of our patients to undergo more frequent observations or over a longer period for practical reasons (such as long distance travel). On the other hand, we were primarily interested in the effects of the drug just during the radiation course which may affect probability of treatment interruptions due to severe skin reactions. So we have no data about the time-to-healing period of ARD (duration of ARD).
We had no data about the patients′ quality of life and possible effects of the drugs on it and we used pure objective data of ARD grade determined by the examining physician only.
We used a clinical scale only. Neither pathologic nor physiologic evaluations are included in the study because of limited financial resources and available laboratory facilities. However, these three measures are related to each other. [2] In addition, clinical outcome is more important to both clinicians and patients than absolute pathologic or physiologic findings. Overall, we provide some evidence to support prophylactic use of topical betamethasone 0.1% during RT in patients whose skin receive high doses of radiation. We did not find any beneficial effect in favor of petrolatum in these situations.
To date, there is no globally accepted standard of care for radiation-induced skin toxicities and further randomized clinical trials are obviously needed. Future studies should focus not only on the preventive or therapeutic effects of the agents, but also on the patients′ quality of life. In addition, the effect of such treatments on the healing rate of ARD, late toxicities and local control can be subjects of future trials.
Acknowledgment
This study was approved and supported by the Shiraz University of Medical Sciences as research project number 2361.
| 1. |
Maddocks-Jennings W, Wilkinson JM, Shillington D. Novel approaches to radiotherapy-induced skin reactions: A literature review. Complement Ther Clin Pract 2005;11:224-31.
[Google Scholar]
|
| 2. |
Hymes SR, Strom EA, Fife C. Radiation dermatitis: Clinical presentation, pathophysiology and treatment 2006. J Am Acad Dermatol 2006;54:28-46.
[Google Scholar]
|
| 3. |
Mendelsohn FA, Divino CM, Reis ED, Kerstein MD. Wound care after radiation therapy. Adv Skin Wound Care 2002;15:216-24.
[Google Scholar]
|
| 4. |
Bostrom A, Lindman H, Swartling C, Berne B, Bergh J. Potent corticosteroid cream (mometasone furoate) significantly reduces acute radiation dermatitis: Results from a double-blind, randomized study. Radiother Oncol 2001;59:257-65.
[Google Scholar]
|
| 5. |
Schmuth M, Wimmer MA, Hofer S, Sztankay A, Weinlich G, Linder DM, et al . Topical corticosteroid therapy for acute radiation dermatitis: A prospective, randomized, double-blind study. Br J Dermatol 2002;146:983-91.
[Google Scholar]
|
| 6. |
Graham P, Browne L, Capp A, Fox C, Graham J, Hollis J, et al . Randomized, paired comparison of No-Sting Barrier Film versus sorbolene cream (10% glycerine) skin care during postmastectomy irradiation. Int J Radiat Oncol Biol Phys 2004;58:241-6.
[Google Scholar]
|
| 7. |
D'haese S, Bate T, Claes S, Boone A, Vanvoorden V, Efficace F. Management of skin reactions during radiotherapy: A study of nursing practice. Eur J Cancer Care (Engl) 2005;14:28-42.
[Google Scholar]
|
| 8. |
Porock D, Kristjanson L. Skin reactions during radiotherapy for breast cancer: The use and impact of topical agents and dressings. Eur J Cancer Care (Engl) 1999;8:143-53.
[Google Scholar]
|
| 9. |
McDougall CJ, Franklin LE, Gresle SO, Long MA. Management of radiation dermatitis in a patient after mastectomy. J Wound Ostomy Continence Nurs 2005;32:337-9.
[Google Scholar]
|
| 10. |
Roper B, Kaisig D, Auer F, Mergen E, Molls M. Theta-Cream versus Bepanthol lotion in breast cancer patients under radiotherapy. A new prophylactic agent in skin care? Strahlenther Onkol 2004;180:315-22.
[Google Scholar]
|
| 11. |
Lorette G, Machet L. Radiation-induced skin toxicities: Prevention, treatment. Cancer Radiother 2001;5:116s-20s.
[Google Scholar]
|
| 12. |
Hill A, Hanson M, Bogle MA, Duvic Mth . Severe radiation dermatitis is related to Staphylococcus aureus. Am J Clin Oncol 2004;27:361-3.
[Google Scholar]
|
| 13. |
Nystrom J, Geladi P, Lindholm-Sethson B, Rattfelt J, Svensk AC, Franzen L. Objective measurements of radiotherapy-induced erythema. Skin Res Technol 2004;10:242-50.
[Google Scholar]
|
| 14. |
Barkham AM. Radiotherapy skin reactions and treatments. Prof Nurse 1993;8:732-6.
[Google Scholar]
|
| 15. |
Fisher J, Scott C, Stevens R, Marconi B, Champion L, Freedman GM, et al . Randomized phase III study comparing Best Supportive Care to Biafine as a prophylactic agent for radiation-induced skin toxicity for women undergoing breast irradiation: Radiation Therapy Oncology Group (RTOG) 97-13. Int J Radiat Oncol Biol Phys 2000;48:1307-10.
[Google Scholar]
|
| 16. |
Harper JL, Franklin LE, Jenrette JM, Aguero EG. Skin toxicity during breast irradiation: Pathophysiology and management. South Med J 2004;97:989-93.
[Google Scholar]
|
| 17. |
Miko Enomoto T, Johnson T, Peterson N, Homer L, Walts D, Johnson N. Combination glutathione and anthocyanins as an alternative for skin care during external-beam radiation. Am J Surg 2005;189:627-31.
[Google Scholar]
|
| 18. |
Zimmermann JS, Wilhelm R, Niehoff P, Schneider R, Kovacs G, Kimmig B. Prevention and therapy of acute radiation injuries of the skin and mucosa. I. Results of a German multicenter questionnaire. Strahlenther Onkol 1998;174:142-8.
[Google Scholar]
|
| 19. |
Zimmermann JS, Budach W, Dorr W. Individual skin care during radiation therapy. Strahlenther Onkol 1998;174:74-7.
[Google Scholar]
|
| 20. |
Schratter-Sehn AU, Brinda K, Kahrer M, Novak M. Improvement of skin care during radiotherapy. Onkologie 2001;24:44-6.
[Google Scholar]
|
| 21. |
Schlappack O. Homeopathic treatment of radiation-induced itching in breast cancer patients. A prospective observational study. Homeopathy 2004;93:210-5.
[Google Scholar]
|
| 22. |
Gorodetsky R, Andriessen A, Polyansky I, Vexler A. Measurement of breast skin viscoelasticity and a pilot study on the potential radioprotective effect of a zinc-based cream. J Wound Care 1999;8:514-8.
[Google Scholar]
|
| 23. |
Hu YR, Wu CQ, Liu YJ, Wang Y, Li X, Zhong H, et al . Clinical observation on effect of shenqi fanghou recipe in preventing and treating radiation injury in patients with head and neck tumor. Zhongguo Zhong Xi Yi Jie He Za Zhi 2005;25:623-5.
[Google Scholar]
|
| 24. |
Ertekin MV, Tekin SB, Erdogan F, Karslioglu I, Gepdiremen A, Sezen O, et al . The effect of zinc sulphate in the prevention of radiation-induced dermatitis. J Radiat Res (Tokyo) 2004;45:543-8.
[Google Scholar]
|
| 25. |
Cuadrillero Martin F, Sandoval Cuadrado P, Rodriguez Hernandez F. Collagen powder: Hydrocolloidal dressings. Their effectiveness in radiodermatitis. Rev Enferm 2004;27:17-22.
[Google Scholar]
|
| 26. |
Cuadrillero Martin F, Sandoval Cuadrado P, Rodriguez Hernandez F. Radiodermatitis. Effectiveness of a collagen dust healing product. Rev Enferm 2001;24:66-9.
[Google Scholar]
|
| 27. |
Kouvaris JR, Kouloulias VE, Plataniotis GA, Balafouta EJ, Vlahos LJ. Dermatitis during radiation for vulvar carcinoma: Prevention and treatment with granulocyte-macrophage colony-stimulating factor impregnated gauze. Wound Repair Regen 2001;9:187-93.
[Google Scholar]
|
| 28. |
Glees JP, Mameghan-Zadeh H, Sparkes CG. Effectiveness of topical steroids in the control of radiation dermatitis: A randomized trial using 1% hydrocortisone cream and 0.05% clobetasone butyrate (Eumovate). Clin Radiol 1979;30:397-403.
[Google Scholar]
|
| 29. |
Potera ME, Lookingbill DP, Stryker JA. Prophylaxis of radiation dermatitis with a topical cortisone cream. Radiology 1982;143:775-7.
[Google Scholar]
|
| 30. |
Fenig E, Brenner B, Katz A, Sulkes J, Lapidot M, Schachter J, et al . Topical Biafine and Lipiderm for the prevention of radiation dermatitis: A randomized prospective trial. Oncol Rep 2001;8:305-9.
[Google Scholar]
|
| 31. |
Szumacher E, Wighton A, Franssen E, Chow E, Tsao M, Ackerman I, et al . Phase II study assessing the effectiveness of Biafine cream as a prophylactic agent for radiation-induced acute skin toxicity to the breast in women undergoing radiotherapy with concomitant CMF chemotherapy. Int J Radiat Oncol Biol Phys 2001;51:81-6.
[Google Scholar]
|
| 32. |
Lokkevik E, Skovlund E, Reitan JB, Hannisdal E, Tanum G. Skin treatment with bepanthen cream versus no cream during radiotherapy--a randomized controlled trial. Acta Oncol 1996;35:1021-6.
[Google Scholar]
|
| 33. |
Wells M, Macmillan M, Raab G, MacBride S, Bell N, MacKinnon K, et al . Does aqueous or sucralfate cream affect the severity of erythematous radiation skin reactions? A randomized controlled trial. Radiother Oncol 2004;73:153-62.
[Google Scholar]
|
| 34. |
Pommier P, Gomez F, Sunyach MP, D'Hombres A, Carrie C, Montbarbon X. Phase III randomized trial of Calendula officinalis compared with trolamine for the prevention of acute dermatitis during irradiation for breast cancer. J Clin Oncol 2004;22:1447-53.
[Google Scholar]
|
| 35. |
Wickline MM. Prevention and treatment of acute radiation dermatitis: A literature review. Oncol Nurs Forum 2004;31:237-47.
[Google Scholar]
|
| 36. |
Olsen DL, Raub W Jr, Bradley C, Johnson M, Macias JL, Love V, et al . The effect of aloe vera gel/mild soap versus mild soap alone in preventing skin reactions in patients undergoing radiation therapy. Oncol Nurs Forum 2001;28:543-7.
[Google Scholar]
|
| 37. |
Richardson J, Smith JE, McIntyre M, Thomas R, Pilkington K. Aloe vera for preventing radiation-induced skin reactions: A systematic literature review. Clin Oncol (R Coll Radiol) 2005;17:478-84.
[Google Scholar]
|
| 38. |
Heggie S, Bryant GP, Tripcony L, Keller J, Rose P, Glendenning M, et al . A Phase III study on the efficacy of topical aloe vera gel on irradiated breast tissue. Cancer Nurs 2002;25:442-51.
[Google Scholar]
|
| 39. |
Williams MS, Burk M, Loprinzi CL, Hill M, Schomberg PJ, Nearhood K, et al . Phase III double-blind evaluation of an aloe vera gel as a prophylactic agent for radiation-induced skin toxicity. Int J Radiat Oncol Biol Phys 1996;36:345-9.
[Google Scholar]
|
| 40. |
Hom DB, Manivel JC. Promoting healing with recombinant human platelet-derived growth factor--BB in a previously irradiated problem wound. Laryngoscope 2003;113:1566-71.
[Google Scholar]
|
| 41. |
Halperin EC, Gaspar L, George S, Darr D, Pinnell S. A double-blind, randomized, prospective trial to evaluate topical vitamin C solution for the prevention of radiation dermatitis. CNS Cancer Consortium. Int J Radiat Oncol Biol Phys 1993;26:413-6.
[Google Scholar]
|
| 42. |
Vasin MV, Ushakov IB, Kovtun VIu, Komarova SN, Semenova LA, Galkin AA. Comparative effectiveness of antioxidant melatonin and radioprotectors indralin and phenylephrine in local radiation injuries. Radiats Biol Radioecol 2004;44:68-71.
[Google Scholar]
|
Fulltext Views
3,981
PDF downloads
3,253





![[Table - 1]](#tbl_ijdvl_2007_73_3_209_32755_4.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2007_73_3_209_32755_5.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2007_73_3_209_32755_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_3_209_32755_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2007_73_3_209_32755_3.jpg){kind=link}