Translate this page into:
Traction alopecia: A neglected entity in 2017
Correspondence Address:
Christiana Oyinlola Akingbola
Department of Dermatology, School of Medicine, Cardiff University, Cardiff, CF
UK
| How to cite this article: Akingbola CO, Vyas J. Traction alopecia: A neglected entity in 2017. Indian J Dermatol Venereol Leprol 2017;83:644-649 |
Abstract
Traction alopecia was first described in 1904 but is still a cause of scarring hair loss in young women worldwide. It is unique in being initially a reversible then an irreversible (scarring) form of alopecia. Linked to tightly-pulled hairstyles, it is seen across all races. The pattern of hair loss depends on the style creating it but most commonly affects the frontotemporal hairline. There are some new examination findings associated with traction alopecia, which are traction folliculitis, the fringe sign and hair casts (pseudonits) on dermatoscopy. These may prove key in prompting early specialist referral. The mainstay of current treatment is cessation of the contributing hairstyles. Camouflage, anti-inflammatory or growth-stimulating topical preparations are second line treatments. In later stages of severe traction alopecia hair transplantation may be the only effective treatment. The evidence basis for medical intervention with topical agents is anecdotal at best. Furthermore, additional research is required to clarify the pathogenesis of this biphasic alopecia. Until then, prompt diagnosis and identification of causative hairstyles are focus of current dermatological practice.Introduction
Traction alopecia is caused by persistent, pulling forces on the hair follicles from traction-inducing hairstyles. It has been reported across all races.[1],[2],[3] Traction alopecia uniquely exists in both the scarring (cicatricial) and non-scarring alopecia categories depending on whether it is early and reversible or late and permanent. The greatest risk from a delay in diagnosis is the progression to scarring traction alopecia.
This review will underline the current understanding of traction alopecia's pathogenesis, its management and their evidence bases.
Epidemiology
At present, traction alopecia has been described across most races. Examples include young Sikh men with tight knots beneath their turbans,[1] a Caucasian ballerina wearing tight buns for 13 years [2] and Hispanic women with tight ponytails [4]. The prevalence of traction alopecia in different populations is still uncertain.
Two South African studies by Khumalo et al. found that 31.7%[5] of women and 9.4%[6] of children had traction alopecia. They also showed a higher prevalence with increasing age in 8.6% of younger girls (ages 6–7) and 21.7% of older girls (ages 17–21).[6] In contrast, a Nigerian study found traction alopecia in only 7.7% (3/39) of women.[7] Wright et al. (an American study) quoted traction alopecia in 18.4% (37/201) in a questionnaire-based study in young girls (ages 1–15).[8] Unfortunately, the Nigerian and American studies had small sample sizes and very little detail of their clinical and histological criteria. Furthermore, there were potential confounders of pregnancy, malnourishment and recall bias about which specific hairstyles were worn regularly. Interestingly, the American study relied solely on carer- or parent-based diagnoses of traction alopecia. In contrast, with their larger sample sizes and dermatologist or experienced clinician diagnoses, the South African studies had more robust findings.
Nonetheless, these studies all agree that traction alopecia is frequently seen in women and children of African descent with a greater prevalence noted with increasing age. They also underline the scarcity of prevalence data from other populations.
Diagnosis
The three key steps for diagnosing traction alopecia are history-taking, scalp examination and specialist tests.
Pertinent questions in the history
These include the duration of the hair loss, which styling practices were previously employed and traction symptoms while creating such hairstyles. In 2008, Khumalo et al. found that traction alopecia was almost twice as likely to be present in South African women or children who had previously experienced tight, painful braids (odds ratio [OR] =1.94 [P = 0.004]) or noted “pimples” at the base of their braids (OR = 1.81 [P = 0.046]) at the time of styling, both of which were statistically significant.[3] This suggests a link between signs of traction during hairstyling and diagnosable traction alopecia.
Clinical examination
This begins at the scalp by looking at the area of hair loss and the hair strands. The hairstyle of the patient is also important. Below are signs that help strengthen a diagnosis of traction alopecia.
Traction folliculitis
Fox et al. first described this perifollicular erythema (redness) and/or pustules following long-standing traction on the hair strands.[9] They noted that these changes were found in the areas that were under maximal tension from the hairstyle.[9] Later, Puttgen reported signs of a dry, itchy and flaky scalp and proposed that the pustules were usually sterile.[10] Urbina et al. also presented a case report of six Chilean ladies (aged 12–26) with traction folliculitis after wearing tight braids, glued-on hair extensions and ponytails.[11] These resolved with traction-avoidance advice and oral antibiotics (though only two cases were confirmed to have Staphylococcus aureus). Interestingly, such findings were described by Hjorth in 1957 as “groups of inflamed follicles,” “perifollicular erythema” and “firmly adherent crusts or scales suggestive of seborrheic eczema” in his marginal traction alopecia case report.[12] Lastly, Khumalo et al. also found that 24.3% (150/604) of South African women with tightly braided hairstyles reported symptoms and signs suggestive of traction folliculitis.[5] Discovering the true prevalence of traction folliculitis would require larger, multi-centered surveys with various racial backgrounds included. An example of traction folliculitis is given here [Figure - 1].
 |
| Figure 1: Traction folliculitis. Perifollicular erythema (blue arrows) |
Pattern of hair loss
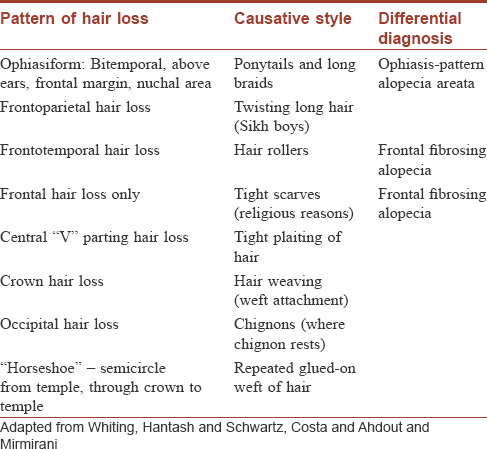
Traction alopecia typically affects the frontotemporal margins of the scalp. However, the specific causative hairstyle will determine any other pattern of hair loss seen.[12],[13],[14],[15],[16],[17],[18] Within areas of hair loss, there will be thin, vellus-like hairs centrally with surrounding mid-length thicker hairs (broken terminal hairs).[13] [Table - 1] summarizes the various patterns of hair loss (Adapted from Whiting [14] Hantash and Schwartz [15], Costa [18] and Ahdout and Mirmirani [17]). [Figure - 2] shows posterior margin traction alopecia.
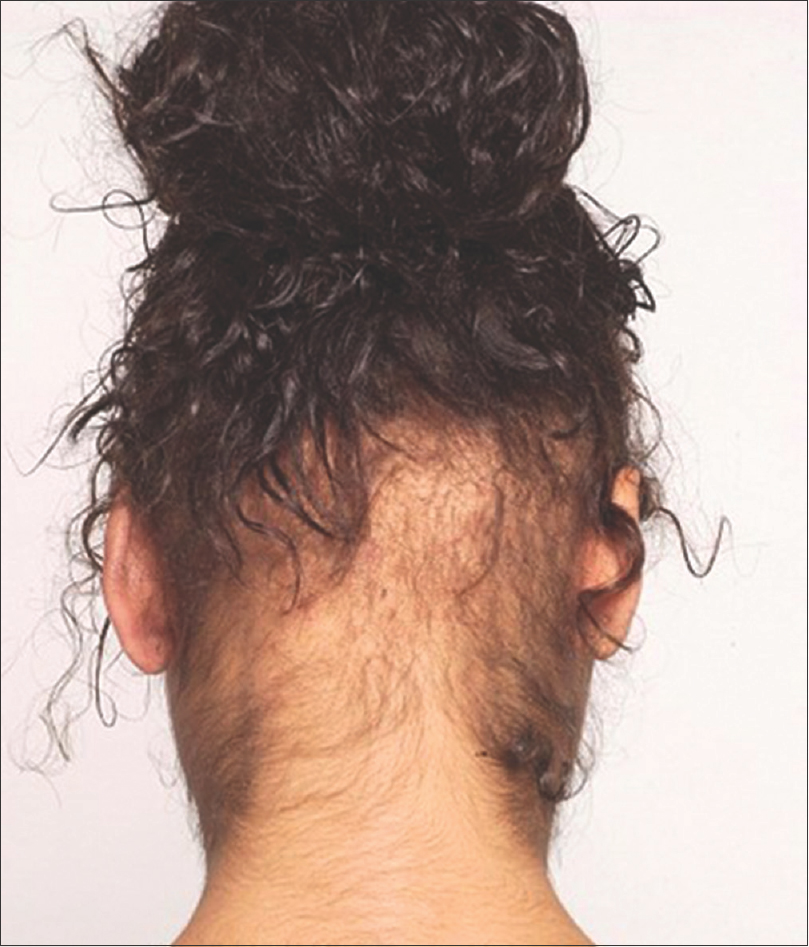 |
| Figure 2: Posterior hairline traction alopecia |
The “Fringe Sign”
This sign, first suggested in 2011 by Samrao et al. describes short terminal hairs bordering areas of marginal hair loss.[4] Interestingly, it is present before clinical hair loss and persists throughout to late traction alopecia.[4] Of note, Costa [18] and Hjorth [12] similarly described this “strip of peripheral hair” in 1946 and “a thin straggling strip of hair at the distal margin” in 1957. The historical constancy of this sign lends credibility to its use as a clinical marker of traction alopecia. In addition, it rules out the main differentials of ophiasis pattern alopecia areata and frontal fibrosing alopecia, respectively [Figure - 3].[4]
 |
| Figure 3: The fringe sign at the right frontotemporal hair margin |
Supplementary tests
Medical photography
This aims to accurately record the extent of traction alopecia and the response to treatment. Khumalo et al. developed the Marginal Traction Alopecia Severity Score in 2007, using photographs of the anterior and posterior hair margins.[19] While it showed good inter-observer agreement in the photograph-matched severity scores (interclass correlation coefficient = 0.99), it was unreliable for diagnosing posterior margin traction alopecia.[19] It still needs to be validated for use in studies and trials.
Dermatoscopy
With its magnified images, dermatoscopy (dermoscopy) allows finer details to be appreciated than naked eye examination.[20] As a non-invasive technique, it should be integral to clinical examination of the scalp. Yin and Tosti suggest using it as a guide for choosing the biopsy site.[21] Dermatoscopy in traction alopecia shows broken hairs, miniaturized hairs, pin-point white dots (loss of follicular openings or ostia), reduced hair density and hair casts.[21],[22]
Hair casts
Hair casts (pseudonits) are 2–7 mm long, freely moveable, gray-white cylinders wrapped around the proximal hair shaft of hairs surrounding areas under tension.[21],[23] They were first associated with traction-inducing hairstyles in 1990 by Zhu et al.[24] Zhang confirmed this in 1995 with a prospective survey of 3548 school-aged women and girls where 81% (1073/1332) of women and girls with tightly braided hair exhibited this sign in the areas under maximal tension.[25] Recent case reports by Tosti et al.[26] and Ozuguz et al.[27] have reinforced this finding [Figure - 4].
 |
| Figure 4: Dermatosopic Image x 20 magnifcation. Hair casts (yellow arrows), vellus like hair (blue arrows), pinpoint white dots (red arrows). Image courtesy of Dr Antonella Tosti |
Histopathology of traction alopecia
Traction alopecia staging is based on its histological appearance as seen in [Table - 2] (adapted from the Literature [2],[26],[27],[28],[29],[30],[31],[32],[33])and the histology slides in [Figure - 5] and [Figure - 6]. Unlike other causes of scarring alopecia that show perifollicular fibrosis and inflammatory infiltrates with loss of sebaceous glands, traction alopecia has preserved sebaceous glands, increased vellus-like hairs and paucity of inflammation.[2],[28]
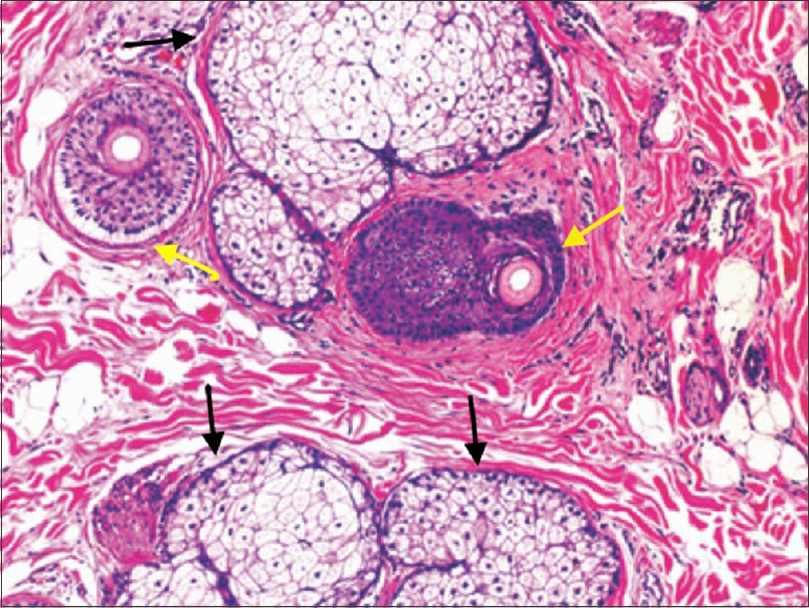 |
| Figure 5: Horizontal section of early traction alopecia with vellus-like follicles (yellow arrows) and retained sebaceous glands (black arrows) (H and E, x10). Image from Miteva and Tosti 201229. Copyright 2012 by John Wiley and Sons |
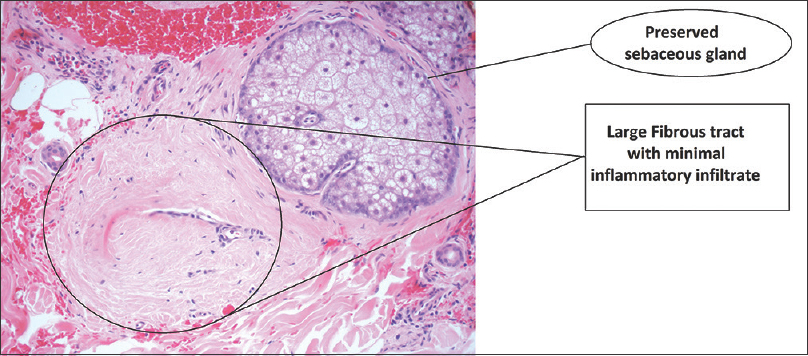 |
| Figure 6: Horizontal section of late-stage traction alopecia with preserved sebaceous glands and fibrous tracts (H and E, ×20) (Image courtesy of Dr. Kenneth May) |
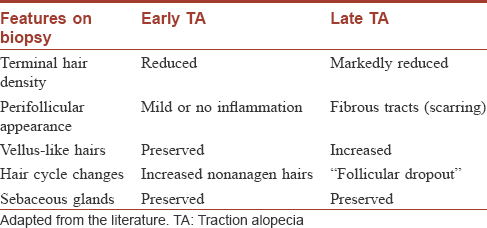
Follicular miniaturization
In 2008, Khumalo et al. hypothesized that the presence of short vellus-like hairs in early traction alopecia may lend credence to a follicular miniaturization theory.[3] This was supported in 2012 by Miteva and Tosti's findings of miniaturized follicles (diameter <0.03 mm) in scalp biopsies [Figure - 5] of African-American women with traction alopecia [29] and its persistence to late-stage traction alopecia. Not surprisingly, they highlighted the possible misdiagnosis of such findings as androgenetic alopecia in the absence of scarring changes in early traction alopecia. Goldberg suggested a means of circumventing this obstacle by noting the overall reduced follicular density of the specimen.[13] He found only 7–8 follicles (on average) per 4 mm punch graft specimen in traction alopecia compared to normal ranges of 21–38 follicles in his 15 biopsy specimens.[13] Nonetheless, this step in the pathogenesis of traction alopecia requires more research to determine if the miniaturization process is a viable target for future therapeutic options.
Follicular drop-out late-stage (scarring) traction alopecia
In this stage of traction alopecia, there are reduced follicular numbers with minimal or no surrounding inflammation.[29] The presence of fibrous tracts indicates a loss of the hair follicles (follicular dropout). In further contrast to other forms of scarring alopecia, the sebaceous glands are preserved [Figure - 6].[28],[31],[32],[33] The point at which the above changes occur is yet to be clarified.
Current Management
The treatment of traction alopecia begins with conservative measures and progresses through medical and surgical interventions.
Conservative management
The mainstay of management is the cessation of the traction-inducing hair practices. This is through patient education with clear guidance on looser hairstyles and the avoidance of chemical damage. In 2014, Mirmirani and Khumalo noted that caregivers (parents) and hairdressers should be primary targets for any educational effort as children and adolescents seemed most at risk.[34]
Although wigs and scalp camouflage (sprays and lotions) help hide areas of hair loss, hair pieces or extensions are discouraged. This advice followed case reports of worsening traction alopecia in a 17-year-old ballerina [2] and a “horseshoe” pattern of hair loss in two women with glued-in hair pieces.[17]
Medical management
Anti-inflammatory preparations
Oral and topical antibiotics are recommended for treating traction folliculitis for their anti-inflammatory effects.[9],[11],[34] Although some articles have mentioned the anecdotal use of corticosteroids (either topically or intralesionally) in traction alopecia, there were no clear cases demonstrating the benefit of this treatment in the literature.[34],[35]
Topical minoxidil 2% preparations
Although mainly used in androgenetic alopecia where it stimulates follicles to differentiate, minoxidil has been discretely used in traction alopecia. In a case report by Khumalo and Ngwanya, traction alopecia refractory to cessation of traction-inducing practices for up to 2 years regrew after 3 months of treatment with 2% minoxidil in two women with long-standing disease.[36] It is also routinely used in the peri- and post-operative period of hair transplantation to reduce graft loss and encourage regrowth.[35]
Surgical management
In refractory cases of late traction alopecia, surgical options include punch grafting, micro- or mini-grafting and follicular unit transplants.[37] The choice of technique is tailored to the patient and the pattern of hair loss. Punch graft hair transplants, first described in 1959, involve transferring 2–4 mm round grafts to the area of alopecia.[35] Follicular unit transplantation has superseded this technique. A microscopically dissected follicular unit - one to four follicles growing in a bundle – is implanted at the recipient site.[37] Advantages of the latter include the seamless appearance of the transplanted hairline, the ability to move more follicular units and the smaller wound size.[38]
Callender et al. found that follicular unit transplants seemed more suited to straighter Caucasoid hair strands while mini- and punch-grafting were better in those of African descent.[35] They postulated that the latter's curved follicles were more likely to be transected (sliced) during follicular unit extraction. Bernstein et al. reported that this occurred in 1.7%–15% of such patients.[38] However, the curly strands are purported to give a fuller-looking result using the traditional methods.[35] The lack of statistical figures or analyses to support this assertion does limit its credence. Careful patient selection is needed to minimize the risk of hypertrophic and keloid scarring when considering hair transplantation.
Discussion
After reviewing the literature, it is clear that traction alopecia is not a new condition. It progresses from a pre-alopecic, inflammatory stage that includes traction folliculitis, through a reversible alopecia (early traction alopecia) to a scarring stage (late traction alopecia) – as seen in [Figure - 8]. Such a timeline may allow earlier intervention with medical therapies. Should these be successful, they would be clues to the pathogenesis from traction to inflammation and eventual scarring [Figure - 8].
The high prevalence rates of traction alopecia noted in those of African descent infers either a genetic susceptibility or persistent environmental factors not addressed by current clinical practice.
Genetic susceptibility to traction alopecia
This genetic susceptibility may be due to the asymmetrical shape of the African hair follicle. It has a retrocurvature at the hair bulb and an S-shaped hair shaft. Thibaut et al. argued that this shape creates geometric points of weakness along the hair shaft.[39] Coupled with fewer anchoring fibers within the dermis, it may predispose them to greater traction forces as shown in [Figure - 7].[40]
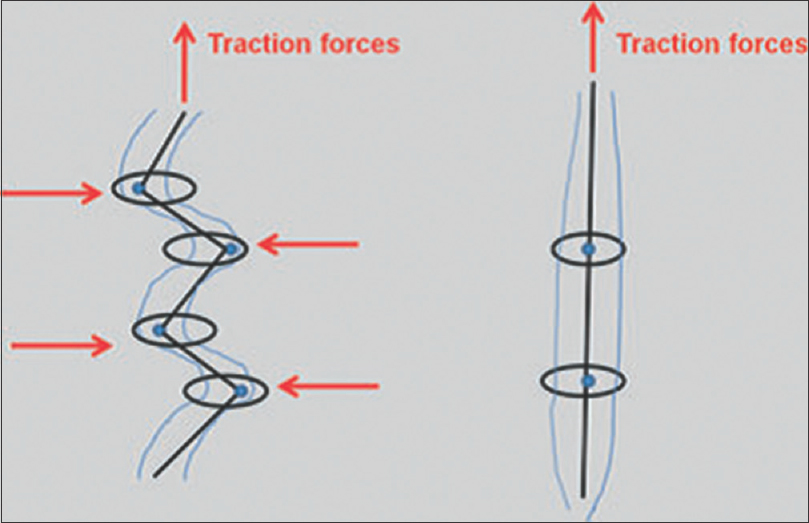 |
| Figure 7: Diagram showing predisposition of curly African hair (left) to traction damage along its length versus straight Caucasian hair (right). (Points of weakness in red). Image from Miteva and Tosti, 201229 Copyright 2012 by John Wiley and Sons |
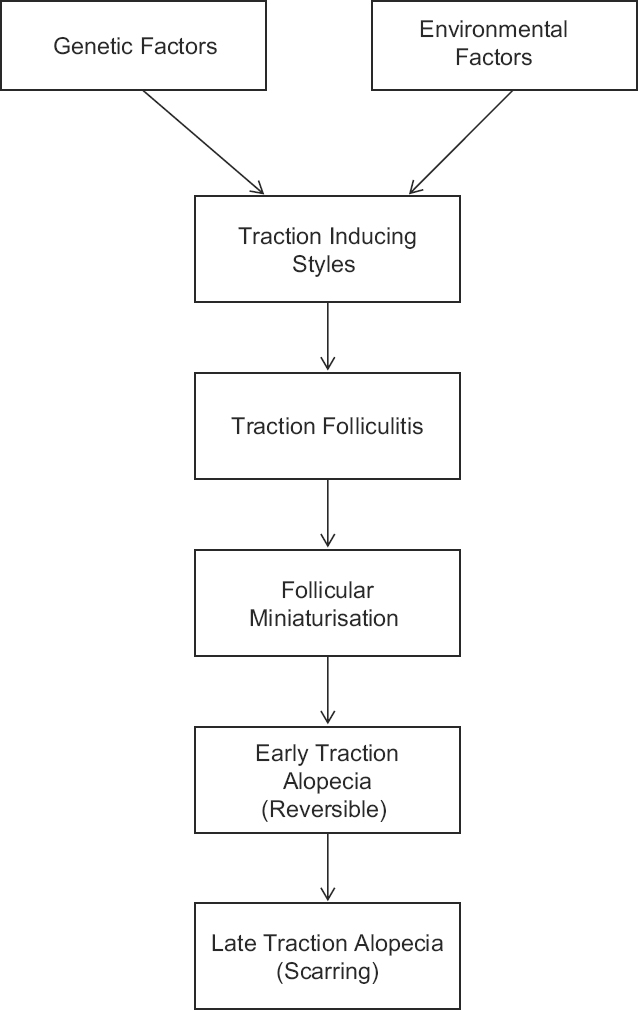 |
| Figure 8: A revised probable pathogenesis of traction alopecia with genetic and environmental factors |
Environmental contributors to traction alopecia
There are two main environmental factors for people of African descent: the chemical processing or “relaxing” of hair strands to achieve a straight appearance and braiding or twisting practices.[34]
“Relaxers” have been in use since the early 1900s to straighten African hair by breaking disulfide and hydrogen bonds within the strands. Research has shown that relaxed hair is more fragile and probably more prone to tension forces.[5],[6] With 59% of South African girls [6] and 80% of African-American women [41] chemically straightening their hair, this may be a key factor in the development of traction alopecia.
In 2014, Mirmirani and Khumalo have proposed a sign to alert women to high tension levels in their braided or twisted hairstyles: “tenting.”[34] This denotes a raised scalp or bumps from the excessive pull on the hair in a braided or twisted style.[34] Hairstyles eliciting this sign should be undone to prevent hair loss.
Finally, the psychosocial impact of traction alopecia has not been explored in the literature. Too often, the physician's focus in making treatment decisions is on the clinical severity of hair loss as evidenced by tools like the marginal traction alopecia severity score. However, it has been shown that physician-perceived hair loss severity does not correlate with the patient's hair loss severity or its effect on their quality of life.[42] Accordingly, patients who felt their disease was more severe or they had no control over it had poorer quality of life outcomes.[42] Furthermore, Cash found that patients seeking professional consult have usually tried several coping mechanisms (like camouflage) before presenting.[43] Various quality of life indices have been trialed including the Dermatology Life Quality Index, Skindex and Scalpdex.[42] These tools can be filled by patients on their first and subsequent consultations.
By exploring the patient's concerns regarding traction alopecia and its regrowth potential, physicians could improve the compliance with medical advice and therapies.
Conclusion
Although traction alopecia has long been agreed to be the end point of long-standing tension hairstyles, steps in its pathogenesis are still perplexing. The presence of vellus-like hairs throughout its development points to follicular miniaturization as a yet under-explored aspect of its pathogenesis. Furthermore, the progression from a reversible hair loss to scarring alopecia is still poorly understood. Nonetheless, traction folliculitis may represent the earliest point for medical intervention. Moreover, newer therapies targeting miniaturized follicles as in androgenetic alopecia may in turn revolutionize traction alopecia management.
Finally, a more robust evidence base for the current medical therapies will hopefully produce a comprehensive treatment algorithm for the optimal management of traction alopecia.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
James J, Saladi RN, Fox JL. Traction alopecia in Sikh male patients. J Am Board Fam Med 2007;20:497-8.
[Google Scholar]
|
| 2. |
Samrao A, Chen C, Zedek D, Price VH. Traction Alopecia in a ballerina: Clinicopathologic Features. Arch Dermatol 2010;146:930-1.
[Google Scholar]
|
| 3. |
Khumalo NP, Jessop S, Gumedze F, Ehrlich R. Determinants of marginal traction alopecia in African girls and women. J Am Acad Dermatol 2008;59:432-8.
[Google Scholar]
|
| 4. |
Samrao A, Price VH, Zedek D, Mirmirani P. The “fringe sign” A useful clinical finding in traction alopecia of the marginal hair line. Dermatol Online J 2011;17.
[Google Scholar]
|
| 5. |
Khumalo NP, Jessop S, Gumedze F, Ehrlich R. Hairdressing and the prevalence of scalp disease in African adults. Br J Dermatol 2007;157:981-8.
[Google Scholar]
|
| 6. |
Khumalo NP, Jessop S, Gumedze F, Ehrlich R. Hairdressing is associated with scalp disease in African schoolchildren. Br J Dermatol 2007;157:106-10.
[Google Scholar]
|
| 7. |
Nnoruka NE. Hair loss: Is there a relationship with hair care practices in Nigeria? Int J Dermatol 2005;44:13-7.
[Google Scholar]
|
| 8. |
Wright DR, Gathers R, Kapke A, Johnson D, Joseph CL. Hair care practices and their association with scalp and hair disorders in African American girls. J Am Acad Dermatol 2011;64:253-62.
[Google Scholar]
|
| 9. |
Fox GN, Stausmire JM, Mehregan DR. Traction folliculitis: An underreported entity. Cutis 2007;79:26-30.
[Google Scholar]
|
| 10. |
Puttgen KB. Traction Folliculitis and Traction Alopecia. Contemp Pediatr 2008;25:2.
[Google Scholar]
|
| 11. |
Urbina F, Sudy E, Barrios M. Traction folliculitis: 6 cases caused by different types of hairstyle that pull on the hair. Actas Dermo-Sifiliograficas 2009;100:503-6.
[Google Scholar]
|
| 12. |
Hjorth N. Traumatic marginal alopecia. A special type: Alopecia Groenlandica. Br J Dermatol 1957;69:319-22.
[Google Scholar]
|
| 13. |
Goldberg LJ. Cicatricial marginal alopecia: Is it all traction? Br J Dermatol 2009;160:62-8.
[Google Scholar]
|
| 14. |
Whiting DA. Traumatic alopecia. Int J Dermatol 1999;38:34-44.
[Google Scholar]
|
| 15. |
Hantash BM, Schwartz RA. Traction alopecia in children. Cutis 2003;71:18-20.
[Google Scholar]
|
| 16. |
Castelo-Soccio L. Diagnosis and Management of Alopecia in Children. Pediatr Clin North Am 2014;61:427-42.
[Google Scholar]
|
| 17. |
Ahdout J, Mirmirani P. Weft hair extensions causing a distinctive horseshoe pattern of traction alopecia. J Am Acad Dermatol 2012;67:e294-e5.
[Google Scholar]
|
| 18. |
Costa OG. Traumatic marginal alopecia due to traction on the hair. Br J Dermatol Syph 1946;58:280-6.
[Google Scholar]
|
| 19. |
Khumalo NP, Ngwanya RM, Jessop S, Gumedze F, Ehrlich R. Marginal traction alopecia severity score: Development and test of reliability. J Cosmet Dermatol 2007;6:262-9.
[Google Scholar]
|
| 20. |
Tosti A, Torres F, Misciali C, Vincenzi C, Duque-Estrada B. The role of dermoscopy in the diagnosis of cicatricial marginal alopecia. Br J Dermatol 2009;161:213-5.
[Google Scholar]
|
| 21. |
Yin NC, Tosti A. A Systematic Approach to Afro Textured Hair Disorders: Dermatoscopy and When to Biopsy. Dermatol Clin 2014;32:145-51.
[Google Scholar]
|
| 22. |
Miteva M, Tosti A. Hair and scalp dermatoscopy. J Am Acad Dermatol 2012;67:1040-8.
[Google Scholar]
|
| 23. |
França K, Villa RT, Silva IR, de Carvalho CA, Bedin V. Hair casts or pseudonits. Int J Trichology 2011;3:121-2.
[Google Scholar]
|
| 24. |
Zhu WY, Xia MY, Wu JH, Do DA. Hair casts: A clinical and electron microscopic study. Pediatr Dermatol 1990;7:270-4.
[Google Scholar]
|
| 25. |
Zhang W. Epidemiological and aetiological studies on hair casts. Clin Exp Dermatol 1995;20:202-7.
[Google Scholar]
|
| 26. |
Tosti A, Miteva M, Torres F, Vincenzi C, Romanelli P. Hair casts are a dermoscopic clue for the diagnosis of traction alopecia. Br J Dermatol 2010;163:1353-5.
[Google Scholar]
|
| 27. |
Ozuguz P, Kacar S, Takci Z, Ekiz O, Kalkan G, Bulbul Sen B. Generalized Hair Casts Due to Traction. Pediatr Dermatol 2013;30:614-5.
[Google Scholar]
|
| 28. |
Stefanato CM. Histopathology of alopecia: A clinicopathological approach to diagnosis. Histopathology 2010;56:24-38.
[Google Scholar]
|
| 29. |
Miteva M, Tosti A. 'A detective look' at hair biopsies from African-American patients. Br J Dermatol 2012;166:1289-94.
[Google Scholar]
|
| 30. |
Salam A, Aryiku S, Dadzie OE. Hair and scalp disorders in women of African descent: An overview. Br J Dermatol 2013;169:19-32.
[Google Scholar]
|
| 31. |
Templeton SF, SantaCruz DJ, Solomon AR. Alopecia: Histologic diagnosis by transverse sections. Semin Diagn Pathol 1996;13:2-18.
[Google Scholar]
|
| 32. |
Borovicka JH, Thomas L, Prince C, Mehregan DR. Scarring alopecia: Clinical and pathologic study of 54 African American women. Int J Dermatol 2009;48:8405.
[Google Scholar]
|
| 33. |
Donovan JC, Mirmirani P. Transversely sectioned biopsies in the diagnosis of end-stage traction alopecia. Dermatol Online J 2013;19:11.
[Google Scholar]
|
| 34. |
Mirmirani P, Khumalo NP. Traction Alopecia: How to Translate Study Data for Public Education Closing the KAP Gap? Dermatol Clin 2014;32:153-61.
[Google Scholar]
|
| 35. |
Callender VD, McMichael AJ, Cohen GF. Medical and surgical therapies for alopecias in black women. Dermatol Ther 2004;17:164-76.
[Google Scholar]
|
| 36. |
Khumalo NP, Ngwanya RM. Traction alopecia: 2% topical minoxidil shows promise. Report of two cases. J Eur Acad Dermatol Venereol 2007;21:433-4.
[Google Scholar]
|
| 37. |
Rogers NE, Callender VD. Advances and Challenges in Hair Restoration of Curly Afrocentric Hair. Dermatol Clin 2014;32:163-71.
[Google Scholar]
|
| 38. |
Bernstein RM, Rassman WR, Stough D. In Support of Follicular Unit Transplantation. Dermatol Surg 2000;26:160-2.
[Google Scholar]
|
| 39. |
Thibaut S, Gaillard O, Bouhanna P, Cannell DW, Bernard BA. Human hair shape is programmed from the bulb. Br J Dermatol 2005;152:632-8.
[Google Scholar]
|
| 40. |
Montagna W, Carlisle K. The architecture of black and white facial skin. J Am Acad Dermatol 1991;24:929-37.
[Google Scholar]
|
| 41. |
Gathers RC, Lim HW. Central centrifugal cicatricial alopecia: Past, present, and future. J Am Acad Dermatol 2009;60:660-8.
[Google Scholar]
|
| 42. |
Reid EE, Haley AC, Borovicka JH, Rademaker A, West DP, Colavincenzo M, et al. Clinical severity does not reliably predict quality of life in women with alopecia areata, telogen effluvium, or androgenic alopecia. J Am Acad Dermatol 2012;66:e97-e102.
[Google Scholar]
|
| 43. |
Cash TF. The psychology of hair loss and its implications for patient care. Clin Dermatol 2001;19:161-6.
[Google Scholar]
|
Fulltext Views
16,928
PDF downloads
3,249





![[Figure - 1]](#fig_ijdvl_2017_83_6_644_213888_f1.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_6_644_213888_t9.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_6_644_213888_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_6_644_213888_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2017_83_6_644_213888_f4.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2017_83_6_644_213888_t10.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2017_83_6_644_213888_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2017_83_6_644_213888_f6.jpg){kind=link}
![[Figure - 8]](#fig_ijdvl_2017_83_6_644_213888_f8.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2017_83_6_644_213888_f7.jpg){kind=link}