
Translate this page into:
Transient pseudophlebitis: Benzyl alcohol-induced transient reactive vasodilation

Corresponding author: Dr. Vishal Gaurav, Department of Dermatology and Venereology, Maulana Azad Medical College, New Delhi, India. mevishalgaurav@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Garg S, Rao A, Yadav D, Gaurav V. Transient pseudophlebitis: Benzyl alcohol-induced transient reactive vasodilation. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_1533_2024
Dear Editor,
We present two female patients, aged 18 and 32 years, diagnosed with chronic plaque psoriasis and psoriatic arthritis without other comorbidities. They were scheduled to receive infliximab infusions, for which they were premedicated with intravenous pheniramine maleate (22.75 mg/mL) and hydrocortisone (50 mg/mL), 2 mL each. Immediately following the administration of these medications, both patients experienced a burning sensation accompanied by erythema along the volar and dorsal tributaries of the cannulated forearm veins. Notably, proximal to the cannulation site, serpiginous networks of venous tributaries became visibly prominent but resolved spontaneously within 10 minutes [Figures 1a, Figure 1b, and Figure 2]. Throughout this time, both patients remained haemodynamically stable and reported no systemic symptoms. The infliximab infusions were subsequently administered without any issues. Neither patient had a history of drug allergies or similar previous reactions, and there were no signs of pain, induration, or other indicators of venous inflammation during or after their hospitalisation period. Since neither pheniramine maleate nor hydrocortisone is typically associated with vasodilation, attention shifted to the preservatives used in the formulations. It was discovered that the pheniramine injection contained 1.5% v/v benzyl alcohol, a known vasodilator, suggesting that it could have been responsible for the observed reactions. No similar preservative was noted in the hydrocortisone injection. During their subsequent infliximab infusions two weeks later, with consent, a challenge test was performed using a pheniramine maleate formulation that did not contain benzyl alcohol. No adverse reactions were observed. However, upon rechallenge with the original pheniramine injection containing benzyl alcohol, both patients redeveloped erythema and a burning sensation, confirming benzyl alcohol as the causative agent. The probability score was 11 (out of 13) on the Naranjo algorithm – adverse drug reaction probability indicating a definite adverse drug reaction.

- The volar tributaries of the vein in the right upper limb before drug challenge in patient 1.

- Erythema along the volar tributaries of the cannulated vein in the right upper limb after drug challenge in patient 1.
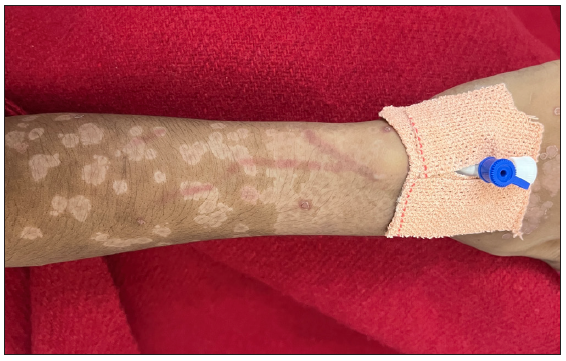
- Erythema along the tributaries of the cannulated vein in patient 2.
Phlebitis, defined as inflammation of the tunica intima, is typically associated with symptoms such as swelling, pain, and erythema around the cannulation site or along the vein.1 In more severe cases, it can result in vein thrombosis. Phlebitis can arise from various aetiologies, including mechanical (intravenous cannula size, location, and composition), chemical (drugs and infusates), and biological (infections) ones.2 Chemical phlebitis occurs when irritative substances, such as drugs with extreme pH values or excessive particulate matter, lead to vascular irritation.2
However, a transient form of phlebitis, termed ‘transient phlebitis” or transient reactive phlebitis (TRP), has also been described. TRP is a benign localised reaction to certain medications, including propofol, diphenhydramine, eptifibatide, ciprofloxacin, and vancomycin.3 It is often characterised by a vermiform rash, mild pain, or erythema and is typically self-limiting, resolving shortly after cessation of the drug. The precise mechanism underlying TRP remains unclear, but several hypotheses have been proposed. TRP may result from direct irritation of the venous endothelium by the infused drug, triggering the release of inflammatory mediators such as histamine or activating the kallikrein-kinin system, which leads to bradykinin release. Additionally, direct stimulation of C-nociceptors in the vein wall could contribute to localised inflammation and pain. The acidic pH of the infusion may further damage endothelial cells, leading to transient inflammation.3,4 In our case, the transient nature of TRP may be attributed to the delayed action of pheniramine, an antihistamine that mitigates histamine-mediated effects by receptor antagonism.
Our case highlights a reaction induced by benzyl alcohol, a common preservative in many injectable medications. It is typically used in concentrations of 0.5-2.0%. Benzyl alcohol is known to cause vasodilation, contact sensitisation, and maculopapular drug reactions. Benzyl alcohol is rapidly metabolised in the body to benzoic acid, which causes prostaglandin-D2 (PGD2) mediated vasodilation.5 We propose that this reaction be named ‘transient pseudophlebitis”, which is more accurate than commonly used terms ‘transient phlebitis” or ‘transient reactive phlebitis”.2-4 Unlike phlebitis, which involves inflammation of the vein, this phenomenon is primarily due to the vasodilatory effects of the offending agent, in this case, benzyl alcohol, rather than any inflammatory process. This distinction is critical, as mislabelling the reaction as phlebitis may lead to unnecessary treatment with anti-inflammatory agents, which is not warranted in cases of transient pseudophlebitis. Another related entity is serpentine supravenous hyperpigmentation, which presents as a darkening of the skin along superficial veins. It can develop after intravenous drug use or the administration of certain intravenous medications, particularly anticancer agents.6
To our knowledge, these are the first reported cases of benzyl alcohol-induced transient pseudophlebitis. Dermatologists and clinicians should be aware of this phenomenon, especially when administering medications containing benzyl alcohol.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- The epidemiology of peripheral vein infusion thrombophlebitis: A critical review. Am J Med. 2002;113:146-51.
- [CrossRef] [PubMed] [Google Scholar]
- Transient phlebitis: An unusual effect of intravenous diphenhydramine. BMJ Case Rep. 2020;13:e237273.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Transient reactive phlebitis induced during anesthesia induction. Anesthesiology. 2024;140:803-4.
- [CrossRef] [PubMed] [Google Scholar]
- “Getting under your skin”: First reported case of transient reactive phlebitis involving vancomycin infusion therapy. Cureus. 2021;13:e18471.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Topical benzoic acid induces the increased biosynthesis of prostaglandin D2 in human skin in vivo. Clin Pharmacol Ther. 1995;57:441-5.
- [CrossRef] [PubMed] [Google Scholar]
- Irinotecan-Induced serpentine supravenous hyper-Pigmentation. Indian J Dermatol. 2022;67:779-81.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




