Translate this page into:
Unilateral angiokeratoma of the scrotum (Fordyce's type) associated with a contralateral varicocele
2 Department of Pathology, Marques de Valdecilla Universitary Hospital, University of Cantabria, IDIVAL, C/Avda. de Valdecilla s/n E-39008, Santander, Spain
Correspondence Address:
Marcos A Gonz�lez-L�pez
Department of Dermatology, Marques de Valdecilla Universitary Hospital, University of Cantabria, IDIVAL, C/Avda. de Valdecilla s/n E-39008. Santander
Spain
| How to cite this article: Gonz�lez-L�pez MA, Consuegra G, Lacalle M, González-Vela M C. Unilateral angiokeratoma of the scrotum (Fordyce's type) associated with a contralateral varicocele. Indian J Dermatol Venereol Leprol 2017;83:470-472 |
Sir
Angiokeratoma of Fordyce is a localized form of angiokeratoma, which typically manifests as multiple vascular, warty papules usually found on the scrotum bilaterally.[1],[2] It was first described in 1896 by J A Fordyce in a 60-year-old male with bilateral varicocele. Histopathologically, it is characterised by vascular dilatation and lacunae formation in papillary dermis with or without thrombosis.[1] We report an unusual case of unilateral scrotal angiokeratoma associated with a contralateral varicocele.
A 68-year-old male presented with multiple asymptomatic cutaneous lesions on his scrotum, which had first appeared 3 years earlier and had progressively increased in number. His medical history was remarkable for hypertension and hypercholesterolemia. Examination revealed multiple, red-purple, 2–3 mm in diameter papules that only affected the right side of the scrotum and did not cross the midline [Figure - 1]. Clinical differential diagnosis included angiokeratoma of Fordyce and angiokeratoma circumscriptum neviforme (ACN). Biopsy specimens of the lesions showed dilated blood vessels in the papillary dermis [Figure 2a]. These ectatic vessels were in intimate contact with the epidermis. Focal thrombosis was present [Figure 2b]. Inmunohistochemical study revealed that the endothelial cells that lined the dilated vascular structures stained positive for CD31 [Figure 2c]. On the basis of age of presentation, and the clinical and histopathological features, a diagnosis of angiokeratoma of Fordyce was made. Ultrasonography of the abdomen and pelvis showed no significant abnormality. However, a grade II left-side varicocele was detected by physical examination and confirmed by Doppler sonography.
 |
| Figure 1: Multiple angiokeratomas on the right side of the scrotum |
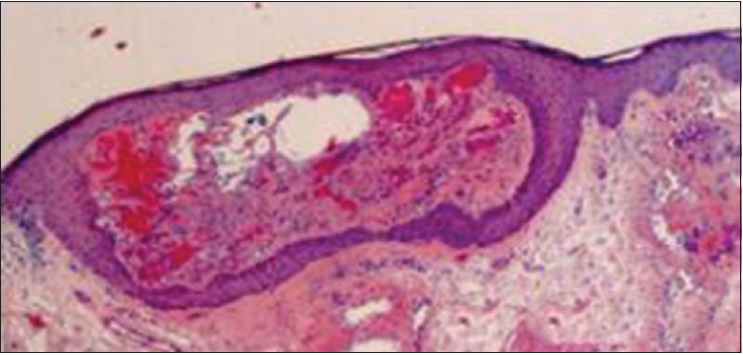 |
| Figure 2a: Histopathological examination showed dilated blood vessels in the papillary dermis (H and E, original magnification ×25) |
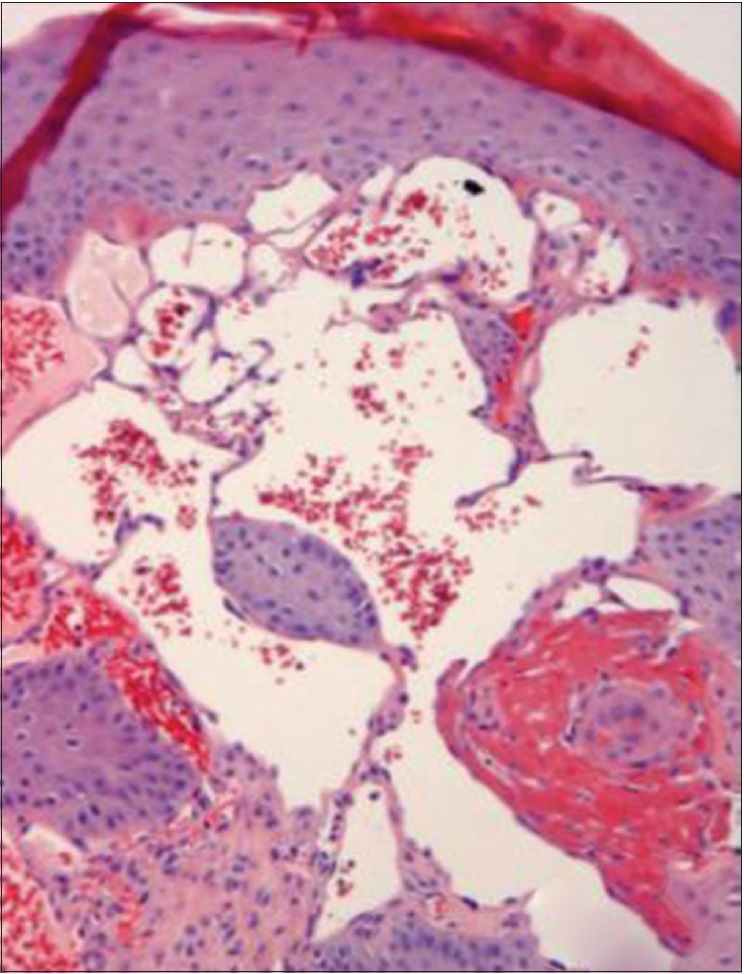 |
| Figure 2b: The ectatic vessels were in intimate contact with the epidermis. Focal thrombosis was present (H and E, original magnification ×100) |
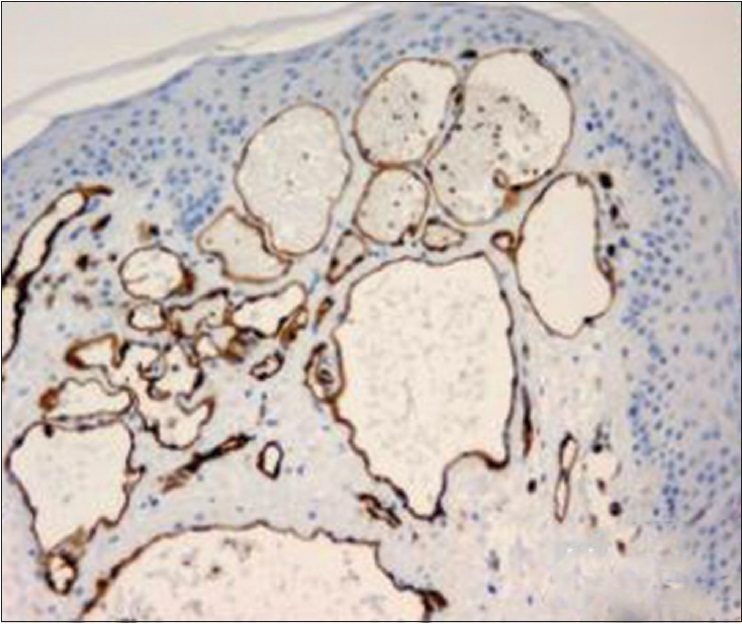 |
| Figure 2c: The endothelial cells that lined the dilated vascular structures showed positivity for CD31 with immunhistochemical staining (CD31, original magnification ×250) |
Angiokeratoma of Fordyce usually develops in late adulthood or in elderly patients, although it may sometimes manifest in childhood or adolescence. The lesions are commonly multiple and they typically arise on the scrotum bilaterally, but are ocassionally found on the shaft or glans of the penis, the thighs, the abdomen, and the buttocks.[1]
The cause of scrotal angiokeratoma is still unknown, although several factors have been postulated regarding its pathophysiology. These include: (i) a reduction of venous supportive elastic tissues, (ii) a direct injury of the dermal capillaries and (iii) a chronic local scrotal venous hypertension.[3],[4] With regard to this last point, some conditions that may increase the blood pressure in the scrotal veins, such as hernias, epididymal or urinary tract tumours and particularly, varicoceles may contribute to the development of scrotal angiokeratoma.[4]
Varicocele is a venous dilatation caused by valvular insufficiency in the internal spermatic vein. It can affect up to 15% of all adult males.[4] Approximately 90% of varicoceles appear on the left side owing to the anatomical difference between the two sides contributing to a higher venous pressure on the left side of the scrotum. Thus, while the right internal spermatic vein empties directly into the inferior caval vein, the vein of the left testicle ascends vertically to the left renal vein.[4],[5]
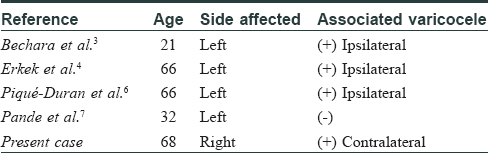
Unilateral angiokeratoma of the scrotum has been very rarely reported. To our knowledge, only five cases have been described in the literature, including our patient.[3],[4],[6],[7] Comparing our case with those reported previously [Table - 1], we wish to highlight the following: (a) in all cases except one,[7] the angiomatous lesions were associated with a varicocele; (b) in three of these four patients,[3],[4],[6] excluding ours, the angiokeratomas were limited to the left side of the scrotum, and they were in association with a left-sided varicocele. In our patient, however, the angiokeratomas were restricted to the right scrotum and, curiously, they were associated with a varicocele of the contralateral testicle. In the present case and in those previously mentioned, the association of angiokeratomas with varicoceles may be simply coincidental, considering that varicoceles are fairly common. However, it is also possible that in those patients with unilateral left-sided angiokeratomas and ipsilateral left-side varicocele, the unilateral development of the angiomatous lesions could have been caused by increased venous pressure due to ipsilateral varicocele.
The reason why the angiomatous lesions developed unilaterally in our case was unknown. A possible explanation would be the presence of mosaicism, which would cause angiokeratomas to develop only in genetically susceptible areas.[6] In this respect, it has been supposed that, at least in some patients, scrotal angiokeratomas may be due to a congenital defect affecting the walls of the venules, but the lesions only become clinically apparent in adulthood.[8]
In this regard, the main differential diagnosis in our case was ACN; however, ACN is typically present at birth and usually involves the lower extremities.[9] Finally, another possibility could be that a previous injurious factor (e.g., chronic irritation) only affecting the right scrotum may have triggered the development of the vascular lesions restricted to this area.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Masuria BL, Gupta LK, Batra A, Kothiwala RK. Angiokeratoma of Fordyce on unusual site. Indian J Dermatol Venereol Leprol 1999;65:240-1.
[Google Scholar]
|
| 2. |
Imperial R, Helwig EB. Angiokeratoma of the scrotum (Fordyce type). J Urol 1967;98:379-87.
[Google Scholar]
|
| 3. |
Bechara FG, Altmeyer P, Jansen T. Unilateral angiokeratoma scroti: A rare manifestation of a vascular tumor. J Dermatol 2004;31:39-41.
[Google Scholar]
|
| 4. |
Erkek E, Basar MM, Bagci Y, Karaduman A, Bilen CY, Gokoz A. Fordyce angiokeratomas as clues to local venous hypertension. Arch Dermatol 2005;141:1325-6.
[Google Scholar]
|
| 5. |
Raheem OA. Surgical management of adolescent varicocele. Surgical management of adolescent varicocele: Systematic review of the world literature. Urol Ann 2013;5:133-9.
[Google Scholar]
|
| 6. |
Piqué-Duran E, Pérez-Cejudo JA, Cameselle-Martínez D, García-Vázquez O. Angiokeratoma de Fordyce unilateral. Actas Dermosifiliogr 2013;104:163-4.
[Google Scholar]
|
| 7. |
Pande SY, Kharkar D, Mahajan S. Unilateral angiokeratoma of Fordyce. Indian J Dermatol Venereol Leprol 2004;70:377-9.
[Google Scholar]
|
| 8. |
Patrizi A, Neri I, Trevisi P, Landi C, Bardazzi F. Congenital angiokeratoma of Fordyce. J Eur Acad Dermatol 1998;10:195-6.
[Google Scholar]
|
| 9. |
Das A, Mondal AK, Saha A, Chowdhury SN, Gharami RC. Angiokeratoma circumscriptum neviforme: An entity, few and far between. Indian Dermatology Online Journal. 2014;5(4):472-4.
[Google Scholar]
|
Fulltext Views
15,384
PDF downloads
2,322





![[Figure - 1]](#fig_ijdvl_2017_83_4_470_206724_f1.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_4_470_206724_t3.jpg){kind=link}