Translate this page into:
Unilateral striate-punctate keratoderma: An extremely rare presentation of punctate keratoderma
2 Department of Pathology, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
Correspondence Address:
Tasleem Arif
Al-Rahman Apartment, Ground Floor, Behind Zakaria Market, New Sir Syed Nagar, Civil Lines Aligarh, Uttar Pradesh
India
| How to cite this article: Arif T, Adil M, Amin SS, Saeed N. Unilateral striate-punctate keratoderma: An extremely rare presentation of punctate keratoderma. Indian J Dermatol Venereol Leprol 2017;83:589-592 |
Sir,
Inherited punctate palmoplantar keratoderma is a rare disease characterized by multiple, small, asymptomatic, keratotic papules on the palms and soles.[1] Punctate keratoderma has rarely been reported in a linear fashion.[2] We found only three reports of unilateral linear type of punctate palmoplantar keratoderma described till now.[3],[4],[5] We present a unique case of unilateral linear punctate plantar keratoderma, a presentation never reported before in literature.
A 26-year-old female presented with linear thickening of the right sole noticed since the age of 8 years [Figure - 1] and [Figure - 2]. The patient initially developed some thickened lesions on the right sole that progressed gradually over several years to form a linear thickening. The patient was born of nonconsanguineous marriage, and there was no history of similar lesions in other family members. There was no history of chronic weight loss, prolonged drug intake, itching, dry skin or other systemic involvement. On examination, a 1 cm × 6 cm sized linear plaque was seen extending from the base of the second interdigital space to the middle of the forefoot on the right sole. This plaque was studded with pinhead-sized punctae, had a rough surface and was non-tender. The examination of the underlying joints showed no signs of inflammation, tenderness or obvious bony abnormality. Paring of the lesions did not show any pin point bleeding. Rest of the cutaneous examination including hair, nails and mucosa was normal. Systemic examination showed no abnormality. Our differential diagnosis included unilateral punctate-striate plantar keratoderma, striate keratoderma, porokeratosis, porokeratotic eccrine ostial and dermal duct nevus, clavus, plantar verruca and callosity. Blood counts, renal and liver function tests and chest radiograph were normal. Stool for occult blood was negative. Histopathology showed orthohyperkeratosis, hypergranulosis and acanthosis [Figure - 3] and [Figure - 4]. There was no cornoid lamella. Genetic analysis was not done due to nonavailability and financial constraints. Based on clinical and histopathological findings, a diagnosis of linear inherited punctate plantar keratoderma of the right sole was made. The patient was started on topical tretinoin 0.025% ointment but was subsequently lost to follow-up.
 |
| Figure 1: Unilateral striate-punctate keratoderma of the right sole with sparing of the left sole |
 |
| Figure 2:Punctate keratoderma in a striate pattern |
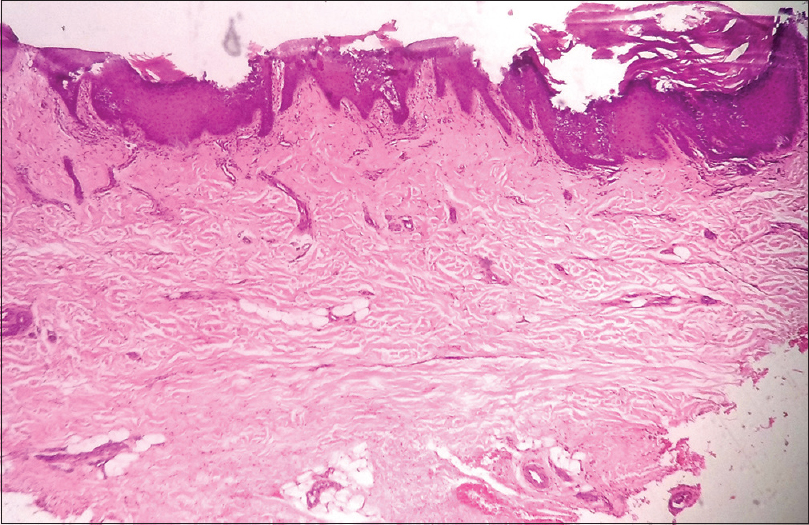 |
| Figure 3: Punctate keratoderma showing orthohyperkeratosis, hypergranulosis and acanthosis (H and E, ×10) |
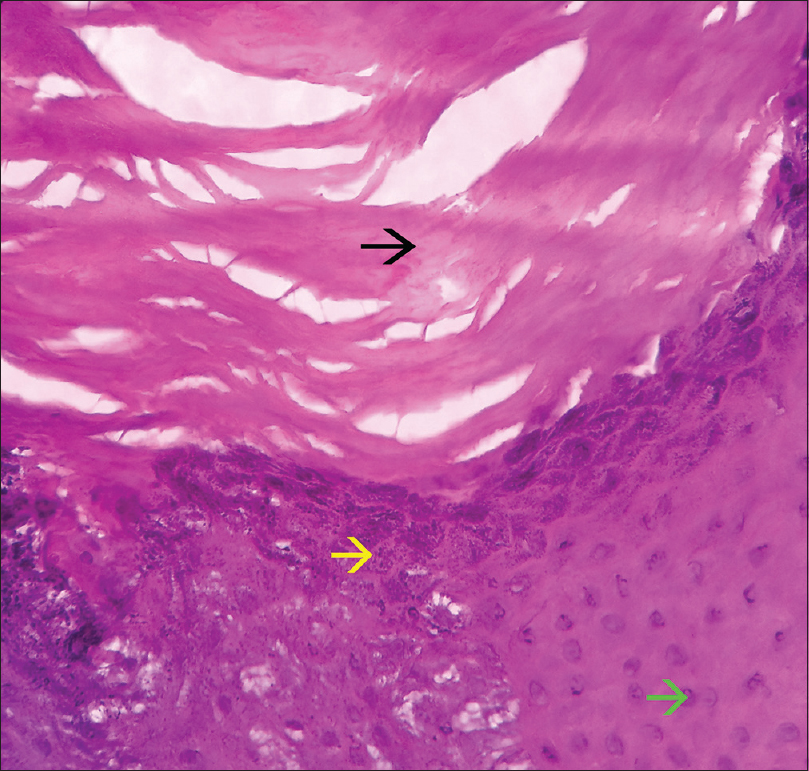 |
| Figure 4: Punctate keratoderma showing hyperkeratosis without any parakeratosis (no nuclei present in corneocytes, black arrow), hypergranulosis (yellow arrow) and acanthosis (green arrow) (H and E, ×40) |
Punctate palmoplantar keratoderma is divided into hereditary and acquired forms. Hereditary punctate palmoplantar keratoderma is seen to occur in the first decade in half of the cases and in second decade in another third.[6] Our patient had the onset of her lesions in the first decade of life. It affects people without discrimination of region or sex.[7] Both genetic and environmental factors including trauma are believed to play a role in the disease pathogenesis.[2] An autosomal dominant mode of transmission with variable penetration is suggested by many case reports.[8] Unilateral involvement has been hypothesized to occur due to genetic mosaicism.[9]
Clinical presentation is that of asymptomatic, thickened, pinpoint papules on the palms and soles. Nails may show longitudinal ridges, onychoschizia, trachyonychia and onychorrhexis.[3] The disease is associated with systemic manifestations such as sebaceous hyperplasia, atopic dermatitis, spastic paralysis and ankylosing spondylitis. However, there were neither nail changes nor systemic involvement in our case. Owing to reports of pulmonary and gastrointestinal malignancies, a regular follow-up of such patients is required.[8] Histopathology of all palmoplantar keratodermas is essentially the same and shows hyperkeratosis, acanthosis without parakeratosis and elastorrhexis.[3] Electron microscopy reveals prominent nucleoli, increased tonofilaments in the stratum basale and keratohyaline granules in the upper spinous layer.[10] Electron microscopy was not done in our patient due to nonavailability.
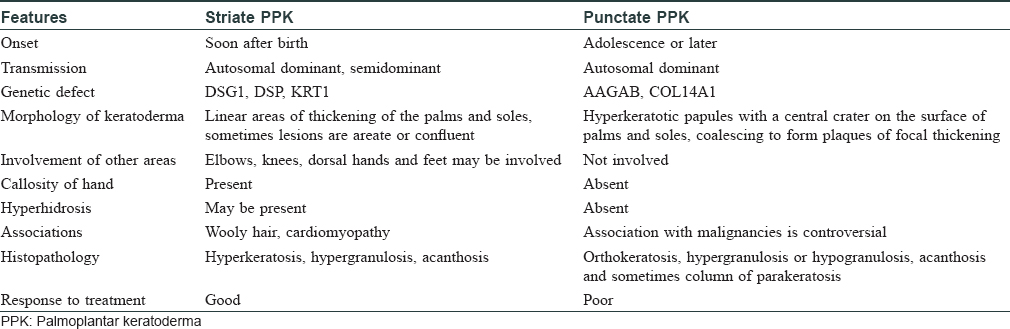
Differential diagnosis includes striate keratoderma, callosities, clavi, plantar warts, linear punctate porokeratosis, porokeratotic eccrine ostial and dermal duct nevus and arsenical keratosis. Striate keratoderma presents soon after birth with linear bands, areate or confluent areas of keratoderma raised well above the skin surface without the punctate lesions and occurs due to genetic mutation in one of the three genes encoding for desmoglein 1, desmoplakin or V1 domain of keratin 1.[11] Punctate palmoplantar keratoderma, on the other hand, has its onset after the first decade, and presents as keratotic papules or crateriform lesions or both.[10] As in our case, the lesions comprised of keratotic papules and crateriform (depressions) lesions arranged in a linear or striate pattern in line with the skin surface or hardly raised above the surface on the sole rather than a thickened plaque which is well elevated above the skin surface as is seen in striate keratoderma of Brunauer–Fuhs–Siemens. [Table - 1] differentiates between these two types of palmoplantar keratodermas. The nonavailability of genetic analysis in our case was a limitation in definite diagnosis and made us rely on clinical parameters for a diagnosis. Corns and callosities are plaques produced due to repeated friction rubbing and occur usually over the pressure sites such as metatarsal heads. Corn is tender on vertical pressure. Plantar warts are sharply defined rough keratotic papules or plaques which on paring show small bleeding points which was not seen in our patient. Punctate porokeratosis presents with characteristic cornoid lamella on histology. Porokeratotic eccrine ostial and dermal duct nevus presents at birth with small keratotic papules with central plugs. Epidermal invaginations filled with parakeratotic plugs and cytoplasmic vacuolization of keratinocytes are seen on histopathology. Arsenical keratosis presents as lesions like that of corn present on the fingers and back of hands. Older lesions show inflammation, ulceration or dysplastic changes on histopathology.[3] Treatment involves keratolytic agents, retinoids, psoralen and ultraviolet A therapy. Retinoids and 5-fluorouracil have shown good therapeutic response.[5],[7]
Unilateral presentation of punctate palmoplantar keratoderma has been reported in some cases.[3],[4],[5],[9] The first report of unilateral linear punctate palmoplantar keratoderma was given by Sharma et al. in 2012.[3] They described a 12-year-old male patient with this disease on the left palm and sole with sparing of the right palm and sole. Two other reports of linear punctate palmoplantar keratoderma have since been reported by Karabacak et al.[4] and Biyik Ozkaya et al.[5] [Table - 2] compares the three reported cases to our patient.

We propose the descriptive name “keratoderma punctata striata unilateralis” for cases of punctate palmoplantar keratoderma presenting unilaterally in a striate pattern. In spite of intense search of literature, the authors were unable to find a previously reported case of inherited linear punctate palmoplantar keratoderma of the sole. We are reporting this case for its rarity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Asadi AK. Type I hereditary punctate keratoderma. Dermatol Online J 2003;9:38.
[Google Scholar]
|
| 2. |
Podder I, Das A, Bhattacharya S, Shome K, Chowdhury SN. Buschke-Fischer-Brauer keratoderma: Linear variety associated with Hodgkin's lymphoma. Indian J Dermatol 2015;60:322.
[Google Scholar]
|
| 3. |
Sharma S, Barman KD, Garg VK, Jain S. Unilateral linear punctate palmoplantar keratoderma. Indian J Dermatol Venereol Leprol 2012;78:85-8.
[Google Scholar]
|
| 4. |
Karabacak E, Kucukodaci Z, Aydin E, Goker K, Abuaf OK. A rare case report: Unilateral punctate palmoplantar keratoderma. J Clin Anal Med 2013;4 Suppl 1:46-8.
[Google Scholar]
|
| 5. |
Biyik Ozkaya D, Tas B, Su O, Unal Cakiter A, Tosuner Z, Demirkesen C, et al. Unilateral linear punctate palmar keratoderma. J Dermatol 2014;41:449-50.
[Google Scholar]
|
| 6. |
Mahajan PM, Gharpuray MB, Kulkarni V. Clinical and histopathological study of palmoplantar keratoderma. Indian J Dermatol Venereol Leprol 1994;60:258-61.
[Google Scholar]
|
| 7. |
Erkek E, Erdogan S, Tuncez F, Kurtipek GS, Bagci Y, Ozoguz P, et al. Type I hereditary punctate keratoderma associated with widespread lentigo simplex and successfully treated with low-dose oral acitretin. Arch Dermatol 2006;142:1076-7.
[Google Scholar]
|
| 8. |
Stevens HP, Kelsell DP, Leigh IM, Ostlere LS, MacDermot KD, Rustin MH. Punctate palmoplantar keratoderma and malignancy in a four-generation family. Br J Dermatol 1996;134:720-6.
[Google Scholar]
|
| 9. |
O'Toole A, O'Malley M. Unilateral keratoderma in a mother and her son. J Cutan Med Surg 2012;16:288-90.
[Google Scholar]
|
| 10. |
Oztas P, Alli N, Polat M, Dagdelen S, Ustün H, Artüz F, et al. Punctate palmoplantar keratoderma (Brauer-Buschke-Fischer syndrome). Am J Clin Dermatol 2007;8:113-6.
[Google Scholar]
|
| 11. |
Tiwary AK, Chatterjee S, Mishra DK. Brunauer-Fuhs-Siemens palmoplantar keratoderma: A rare, striate type of focal palmoplantar keratoderma. Indian J Paediatr Dermatol 2016;17:246-8.
[Google Scholar]
|
Fulltext Views
4,288
PDF downloads
1,443





![[Figure - 1]](#fig_ijdvl_2017_83_5_589_211155_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_5_589_211155_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_5_589_211155_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2017_83_5_589_211155_f4.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_5_589_211155_t5.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2017_83_5_589_211155_t6.jpg){kind=link}