
Translate this page into:
Unusual presentation of digital papillary adenocarcinoma in a sporotrichoid pattern
Corresponding author: Dr. Shruti Sharma, Department of Pathology, ICMR National Institute of Pathology, Safdarjung Hospital Campus, New Delhi, India. shrutigautam@rediffmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gupta A, Khullar G, Divyashree R, Sharma S. Unusual presentation of digital papillary adenocarcinoma in a sporotrichoid pattern. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_932_2023
Dear Editor,
Digital papillary adenocarcinoma (DPAC) is a rare, slow-growing, malignant tumour of eccrine glands with a predilection for acral sites.1 It is known for its high recurrence rate and metastatic potential. Here, we report a unique presentation of DPAC as multiple cutaneous nodules and a verrucous plaque in a sporotrichoid distribution on the left upper limb, masquerading as an infectious condition.
A 62-year-old woman presented with a 6-year history of a gradually progressive asymptomatic plaque on the left forefinger and nodules on the left forearm. The lesions had increased in size in the last 6 months. Cutaneous examination revealed an ill-defined verrucous plaque, focally ulcerated, measuring 4 × 3 cm on the distal aspect of the left forefinger, causing nail dystrophy and flexion deformity, and two well-defined, firm, skin-coloured nodules measuring 1 × 1 cm, proximally on the extensor surface of the left forearm and elbow in a linear distribution [Figures 1a and 1b]. Lymph nodes were not palpable and systemic examination was unremarkable. Clinically, differential diagnoses of lymphocutaneous sporotrichosis, cutaneous leishmaniasis, atypical mycobacterial infection and tuberculosis verrucosa cutis were considered. Two punch biopsies were performed, one from the verrucous plaque and the other from the nodule on the forearm. Histopathological examination from both the lesions showed unremarkable epidermis with an underlying grenz zone separating it from a poorly circumscribed tumour filling the dermis. The tumour was composed of multiple, variably dilated and interconnected duct-like structures lined by two cell layers: inner lined by cuboidal to columnar cells and outer lined by myoepithelial cells. Focal areas of multi-layering and papillary infoldings, mild to moderate atypia and frequent mitotic figures were seen [Figures 2a and 2b]. Solid areas with back-to-back glands were also noted. Presence of solid areas ruled out the possibility of tubular papillary adenoma. Immunohistochemistry (IHC) revealed diffuse positivity for pan cytokeratin, CD15 and S-100 in the tumour cells and smooth muscle actin in myoepithelial cells. There was a high proliferative index of approximately 40% with Ki-67 [Figures 2c, 2d, 2e and 2f]. Histopathology images from the verrucous plaque also show similar morphology [Figure 3]. Tissue cultures for fungus, leishmaniasis and atypical and typical mycobacterial infection were all negative. Based on the clinical and histological findings, a final diagnosis of sporotrichoid DPAC was made. Routine haematological and biochemical investigations were unremarkable. Positron emission tomography scan did not reveal any metastasis. The patient was referred to the Department of Surgical Oncology, where her forefinger was amputated along with excision of both the nodules followed by radiotherapy. There was no evidence of local recurrence or distant metastasis after 1 year of follow-up and the patient is doing well.

- Verrucous plaque on the forefinger showing focal ulceration and causing nail dystrophy distally.

- Verrucous plaque on the forefinger and skin-coloured nodule on the forearm in a linear arrangement.
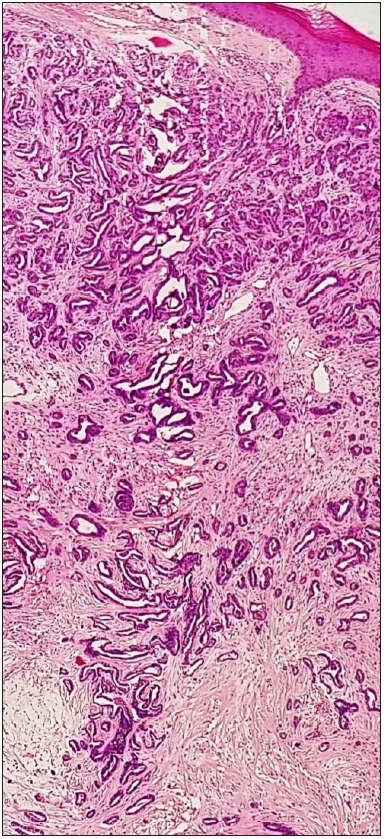
- Tumour is composed of multiple variably dialated and anastomosing duct like structures in the dermis (Haematoxylin and eosin, x40).
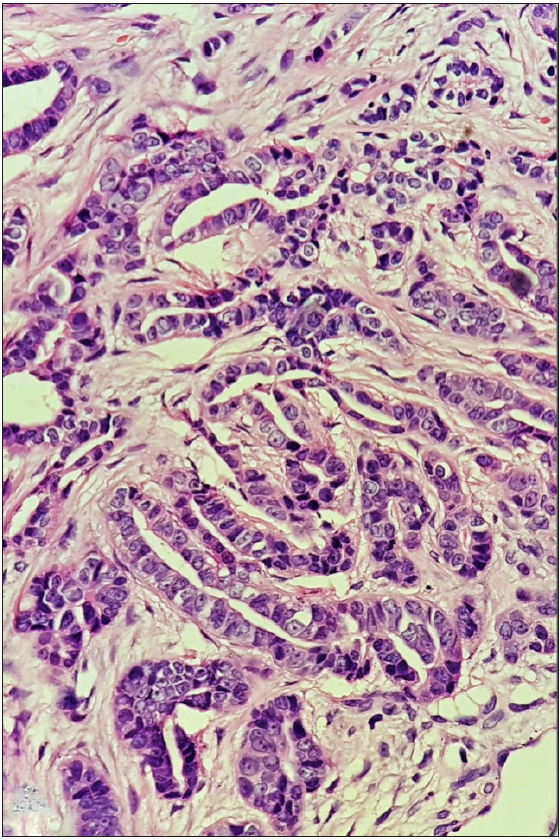
- Tumour composed of multiple variably dialated and anastomosing duct like structures in the dermis (Haematoxylin and eosin, x400).
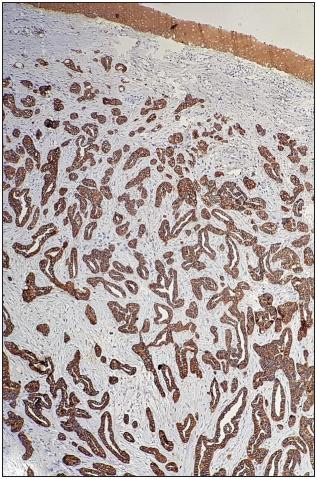
- Immunohistochemistry (IHC) reveals diffuse positivity for pancytokeratin in tumour cells IHC CK; ×100).
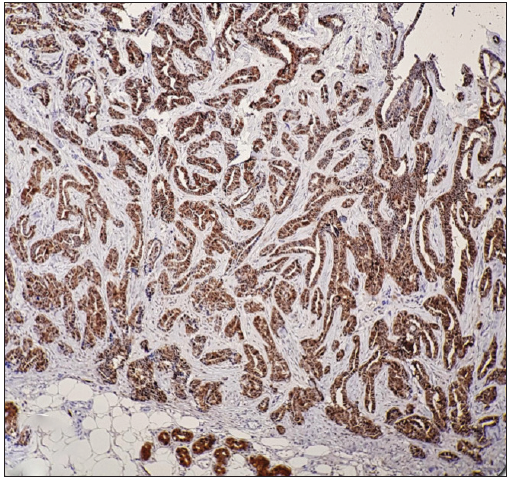
- Diffuse positivity for S-100 in tumour cells (IHCS100; ×100).
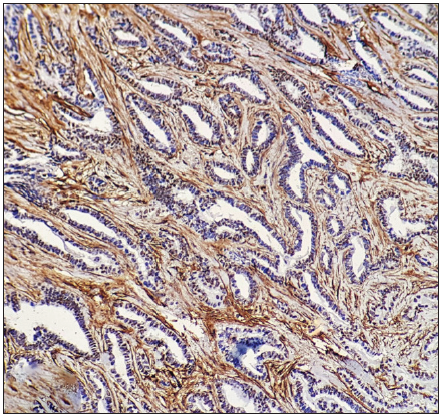
- Smooth muscle actin positivity in myoepithelial cells (IHC-SMA; ×200).
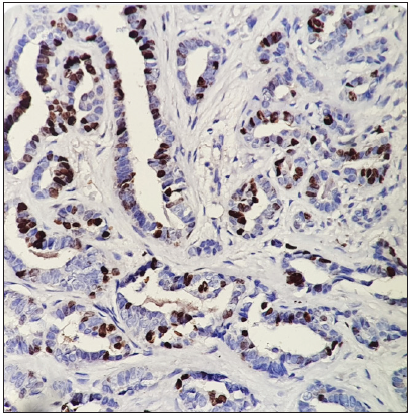
- Tumour cells showing positivity for Ki 67 (IHC-Ki67; ×100).
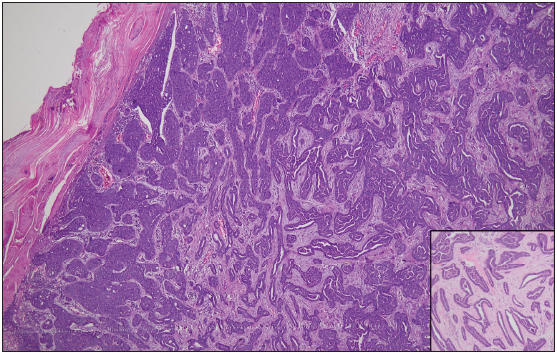
- Histopathology image from verrucous plaque showing marked hyperkeratosis and parakeratosis. Entire dermis is infiltrated by a tumour composed of ducts and solid areas. (H&E x40). Inset show tumour in high magnification (x400).
In the past, digital papillary adenoma and adenocarcinoma were considered as separate entities, but neither the clinical features nor the histomorphology predicted the incidence of recurrences or metastasis. Hence, in 2006, WHO classified both the terminologies under a single entity of DPAC, in the absence of any benign counterpart.2 DPAC presents as a solitary mass that frequently involves the distal aspect of the finger/thumb or palm and sole. Our case is unique in terms of multiple lesions of the upper limb. The clinical differential diagnoses include digital mucous cyst, foreign body granuloma, paronychia, benign adnexal tumour and vascular tumour-like pyogenic granuloma and glomus tumour. Histologically, it may resemble sweat gland tumours like spiradenocarcinoma or metastatic adenocarcinoma from colon, thyroid or breast.3
Surgical management options for DPAC include wide excision, digital amputation, partial digital amputation or Mohs micrographic surgery.4 Long-term follow-up is important for the early detection of local recurrence and metastasis to lymph nodes and lungs.
The present case was unique since sporotrichoid pattern of involvement in DPAC mimicking an infectious aetiology has not been described in literature. Besides infections, rarely cutaneous tumours such as metastatic cutaneous squamous cell carcinoma, lymphomas, melanoma, epithelioid sarcoma, peripheral nerve sheath tumour and keratoacanthomas have been reported to present in a sporotrichoid fashion.5 Digital papillary adenocarcinoma is known for local recurrence and distant metastasis, mostly to the lungs, owing to the haematogenous spread. However, lymph node involvement is also described in literature explaining the lymphatic spread. Hence, it appears to be spread via both haematogenous and lymphatic routes. Lymphatic spread appears to be the most probable explanation in our case.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Aggressive digital papillary adenocarcinoma (aggressive digital papillary adenoma and adenocarcinoma revisited) Am J Surg Pathol. 2000;24:775-84.
- [CrossRef] [PubMed] [Google Scholar]
- World Health Organization classification of tumours: Pathology and genetics of skin tumours. Lyon: IARC Press; 2006. p. :133-4.
- Aggressive digital papillary adenocarcinoma: A report of two diseases and review of the literature. J Am Acad Dermatol. 2009;60:331-9.
- [CrossRef] [PubMed] [Google Scholar]
- Aggressive digital papillary adenocarcinoma with multiple organ metastases: A case report and review of the literature. Am J Dermatopathol. 2016;38:910-14.
- [CrossRef] [PubMed] [Google Scholar]
- Sporotrichoid keratoacanthomas: Case report and review of neoplasms presenting in a sporotrichoid pattern. Cureus. 2018;10:3196.
- [Google Scholar]




