Translate this page into:
Verruciform xanthoma of the penis: A rare case with an unusual clinical morphology
2 Department of Pathology, Istanbul Medical Faculty, Istanbul University, Istanbul, Turkey
Correspondence Address:
Goncagul Babuna Kobaner
Millet Street (Caddesi), Capa, 34093, Istanbul
Turkey
| How to cite this article: Babuna Kobaner G, Demir O, Ozturk Sari S, Baykal C, Buyukbabani N. Verruciform xanthoma of the penis: A rare case with an unusual clinical morphology. Indian J Dermatol Venereol Leprol 2018;84:600-602 |
Sir,
Verruciform xanthoma is a rare benign lesion of unknown etiology. Although it primarily affects the oral mucosa, the genital area including vulva, scrotum and penis may also be involved. Only 33 cases of penile form have been reported in the literature till date.[1],[2],[3],[4],[5]
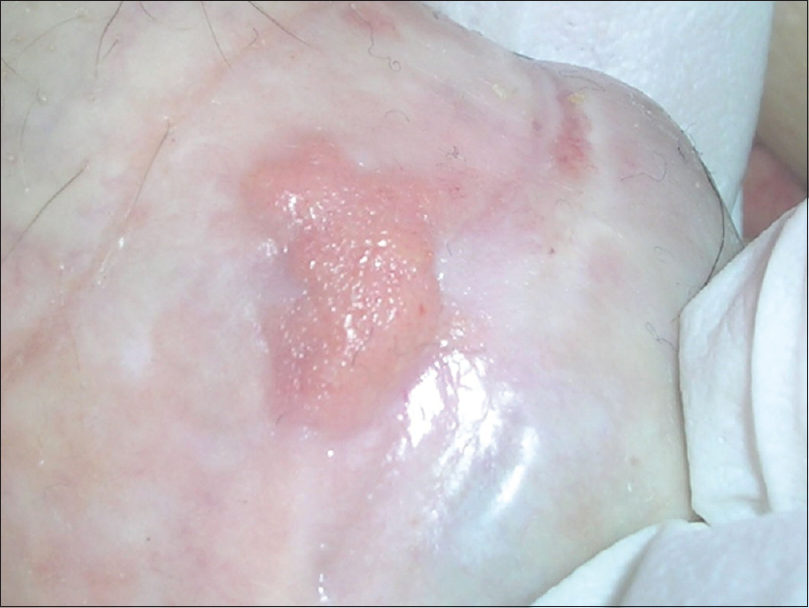
We herewith present a 78-year-old Turkish man with a 2-month history of a rapidly growing asymptomatic exophytic tumoral lesion on the ventral part of the penis. The lesion measured 1 × 1 cm and showed a combined morphology with a yellowish, erythematous, verrucous base and a bright yellowish-pink, pedunculated component with a papillomatous, “mulberry-like” surface [Figure - 1]. There was neither a coexisting extragenital lesion nor inguinal lymphadenopathy. His current and past medical history was unremarkable, except for a traditional circumcision procedure in the childhood. Blood tests including lipid profile were within the normal levels and serology for hepatitis and human immunodeficiency virus was negative.
 |
| Figure 1: Penile tumoral lesion showing a combined morphology with a yellowish, erythematous verrucous base, and a bright yellowish-pink, pedunculated component with a papillomatous, “mulberry-like” surface |
An incisional biopsy involving the papillomatous part of the tumor showed verruciform acanthosis in the epidermis and numerous lipid-laden, foamy histiocytes in the papillary dermis [Figure - 2] and [Figure - 3], revealing a diagnosis of verruciform xanthoma. Additionally, p16 immunohistochemistry revealed only a weak patchy staining of epidermal cells, which excludes a possible human papilloma virus infection in the pathogenesis. Complete surgical excision was planned, but the patient refused treatment. In a 20-month follow-up, no change was observed in the remaining basal portion of the tumor [Figure - 4].
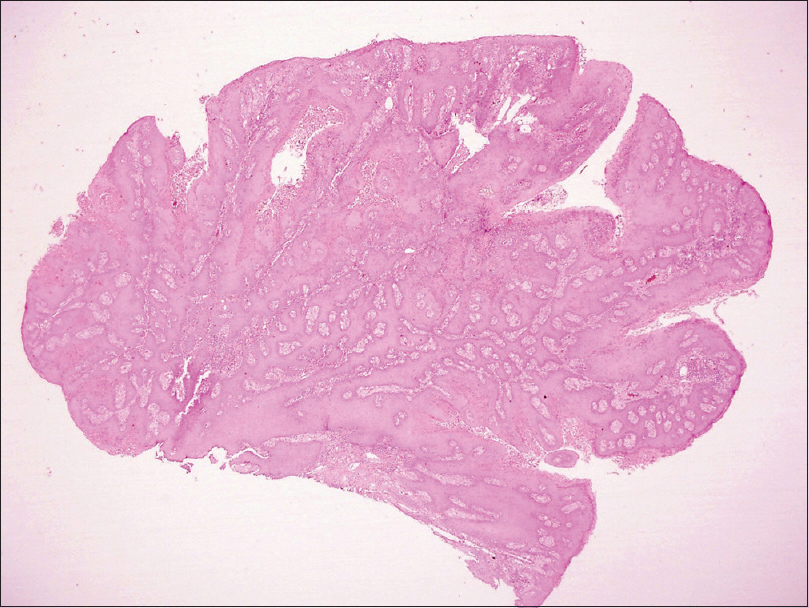 |
| Figure 2: The papillomatous part of the tumor seen under low magnification [hematoxylin and eosin (H and E), ×20] |
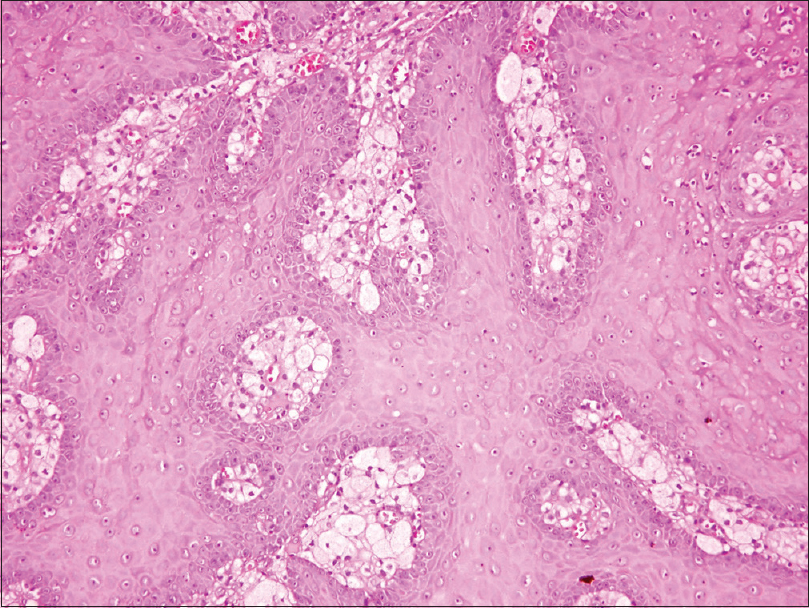 |
| Figure 3: In higher magnifications, proliferative squamous epithelium and foamy histiocytes under the epithelium are remarkable (H and E, ×200) |
 |
| Figure 4: The yellowish, erythematous verrucous base of the tumor after incisional biopsy involving the pedunculated portion |
The etiopathology of verruciform xanthoma remains elusive till date. An association with human papillomavirus infection or lipid disorders has been suggested, but not confirmed, in most of the patients.[1] Owing to its association with lichen planus, an autoimmune etiopathology including apoptosis of epithelial cells has also been proposed.[2] The latest concept however is based on a traumatic or inflammatory injury leading to keratinocyte degeneration and an inflammatory reaction, which induces macrophages to engulf lipid material released from the epithelial cells and become lipid-laden, foamy histiocytes.[3] The xanthomatous appearance in verruciform xanthoma is related to the presence of these subepithelial foamy histiocytes and epithelial hyperplasia is a secondary change.
Verruciform xanthoma may occur in the setting of various cutaneous disorders such as congenital hemidysplasia with ichthyosiform erythroderma and limb defects (CHILD syndrome), inflammatory linear verrucous epidermal nevus and dystrophic epidermolysis bullosa, suggesting that it may be an unusual reactive phenomenon.[1] It has also been reported in patients following bone marrow transplantation, with or without graft versus host disease.[4] Nevertheless, our patient had no associated dermatoses or systemic diseases.
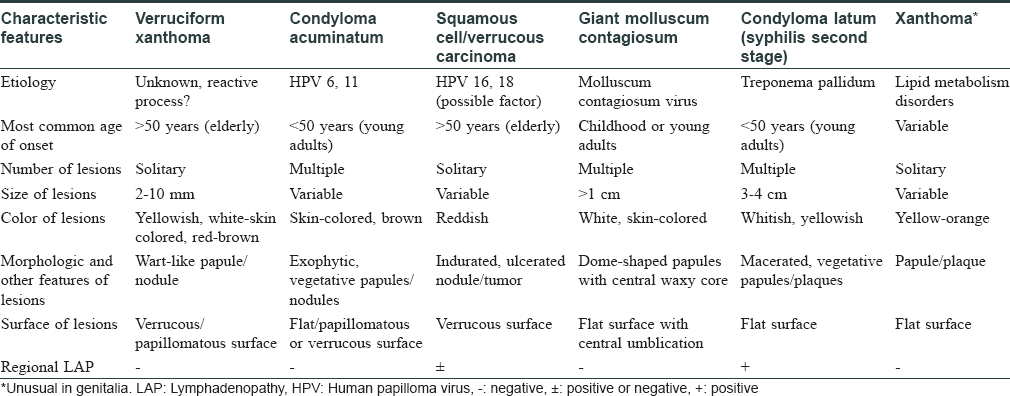
Penile verruciform xanthoma typically presents as an asymptomatic, solitary lesion of 2–10 mm in an otherwise healthy man, usually after the fifth decade of life. It may grow slowly over years or rarely, as in our case, shows rapid growth in just a few months. A review of previously reported cases revealed that although the pedunculated or sessile tumor on the penis may present in a broad range of colors, from whitish or skin-colored to pinkish-red and brown, it usually has a yellowish hue, which may be considered as an important clinical clue for differentiation from other tumoral lesions, including mainly condyloma acuminatum.[1],[2],[3],[4],[5] Moreover, in some cases, it may be indurated and focally ulcerated, mimicking malignancy. Although the clinical differential diagnosis of verruciform xanthoma includes several benign and malignant conditions, which are summarized in [Table - 1], its morphological characteristics and histopathological appearance with subepithelial foamy histiocytes are unique, and performance of a biopsy in suspicious cases is crucial to the diagnosis.[3],[4],[5] As genital occurrence is not a well-known feature of verruciform xanthoma, the diagnosis of penile verruciform xanthoma may be delayed, and patients may receive incorrect or unnecessarily aggressive treatments.
In the literature, penile lesions of verruciform xanthoma are often described as wart-like papules/nodules with a “cauliflower-like” verrucous surface, whereas scrotal verruciform xanthoma may also present with “mulberry-like” papillomatous lesions.[2] However, a combined morphology consisting of a pedunculated component on a verrucous base, as in our case, has not been reported previously in penile verruciform xanthoma.
Surgical excision remains the gold standard for the treatment of verruciform xanthoma, whereas superficial electrocauterization, carbon dioxide laser, cryotherapy, radiotherapy, topical steroids, and imiquimod have been used in select cases.[5] Given the benign nature of verruciform xanthoma, a wait-and-see approach is another option, especially in elderly patients, and it was the choice made in this case.
Although rare, verruciform xanthoma should be kept within the differential diagnosis for solitary tumoral penile nodules with a yellowish color in elderly patients. It should be noted that verruciform xanthoma lesions may have an atypical clinical appearance of the described variants, such as showing two components.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Requena L, Sarasa JL, Martin L, Pique E, Farina MC, Olivares M, et al. Verruciform xanthoma of the penis with acantholytic cells. Clin Exp Dermatol 1995;20:504-8.
[Google Scholar]
|
| 2. |
Stiff KM, Cohen PR. Vegas (Verruciform genital-associated) xanthoma: A comprehensive literature review. Dermatol Ther (Heidelb) 2017;7:65-79.
[Google Scholar]
|
| 3. |
De Rose AF, Tosi M, Mantica G, Piol N, Toncini C, Terrone C, et al. Verruciform xanthoma of the penis: A rare benign lesion that simulates carcinoma. Arch Ital Urol Androl 2016;88:284-5.
[Google Scholar]
|
| 4. |
Xue R, Su W, Pei X, Huang L, Elbendary A, Chen Z, et al. Multiple verruciform xanthomas following bone marrow transplant. Indian J Dermatol Venereol Leprol 2016;82:208-9.
[Google Scholar]
|
| 5. |
Sette CS, Wachholz PA, Brandão LS, Marques GF, Casafus FS, Soares CT, et al. Verruciform xanthoma on the penis: An unusual location. Clin Exp Dermatol 2015;40:807-8.
[Google Scholar]
|
Fulltext Views
5,073
PDF downloads
1,663





![[Figure - 1]](#fig_ijdvl_2018_84_5_600_238745_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_5_600_238745_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_5_600_238745_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_5_600_238745_f4.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2018_84_5_600_238745_t5.jpg){kind=link}