Translate this page into:
Verrucous carcinoma of the upper lip: An exuberant presentation in a patient with other synchronous lesions
2 Department of Maxillofacial Surgery, Garcia de Orta Hospital, Almada, Portugal
Correspondence Address:
Ana Marta Antonio
Av. Torrado da Silva, 2801-951 Almada
Portugal
| How to cite this article: Antonio AM, Barreiros H, Goulão J, Barbosa N, Bártolo E. Verrucous carcinoma of the upper lip: An exuberant presentation in a patient with other synchronous lesions. Indian J Dermatol Venereol Leprol 2020;86:230 |
Sir,
Verrucous carcinoma is an uncommon variant of squamous cell carcinoma, first described by Ackerman in 1948, characterized by proliferative outgrowth, presenting locally destructive behavior, but low tendency of dissemination when not associated with invasive squamous cell carcinoma component. The oral cavity is the most frequent location but it is also reported in the larynx, pyriform sinus, nasal cavity, external auditory meatus, esophagus, genitals, uterine cervix and skin. In the oral cavity, it is more common on the buccal and alveolar mucosae, than on the tongue, lip and palate.[1] The pathogenesis of oral cavity verrucous carcinoma is uncertain. Some studies report the association with chronic use of inhaled or chewable tobacco, alcohol and a potential role of human papillomavirus infection, particularly through downregulation of oncosuppressor genes.[2]
We report a case of an 80-year-old woman patient, presenting with an exophytic verrucous nonbleeding tumor, covered by a yellowish-to-brown crust, 4 cm in diameter, firm upon palpation, occupying almost all the upper lip [Figure - 1]. Differential diagnosis included squamous cell carcinoma, verrucous carcinoma, amelanotic melanoma and viral wart. She had been examined 6 months before due to extensive, indurated and verrucous plaques on buccal, alveolar, palate and upper lip mucosae suggestive of proliferative verrucous leukoplakia [Figure - 2]. The first biopsy of the lip lesion was inconclusive. The patient abandoned follow-up and returned when the tumor reached these proportions. She was a nonsmoker and her medical history was unremarkable. There was no history of lichen planus or other inflammatory mucosal disease. An excisional biopsy without surgical margins was performed and histopathological examination was compatible with verrucous carcinoma [Figure - 3]. No low or high-risk human papillomavirus-DNA was detected by reverse transcription polymerase chain reaction technique for 6, 11, 16, 18 and other 14 high-risk serotypes. Clinical examination and further investigation excluded peripheral lymphadenopathies and disseminated disease. A wedge excision followed by M-plasty was performed and histopathological result showed positive margins in the lip mucosa, and therefore, a wide excision and reconstruction with Karapandzic-modified flap technique was performed by a maxillofacial surgeon with complete excision of the tumor. The other lesions were histopathologically compatible with proliferative verrucous leukoplakia, except one of them localized on the buccal mucosa that was classified as another verrucous carcinoma, and they were treated with carbon dioxide laser and surgical excision depending on the type of lesion. After 2 years of follow-up, no relapse was observed. Serologic tests for HIV were negative and no other forms of immunosuppression or concomitant diseases were found.
 |
| Figure 1: |
 |
| Figure 2: Verrucous leukoplakia on buccal, alveolar and palate mucosa |
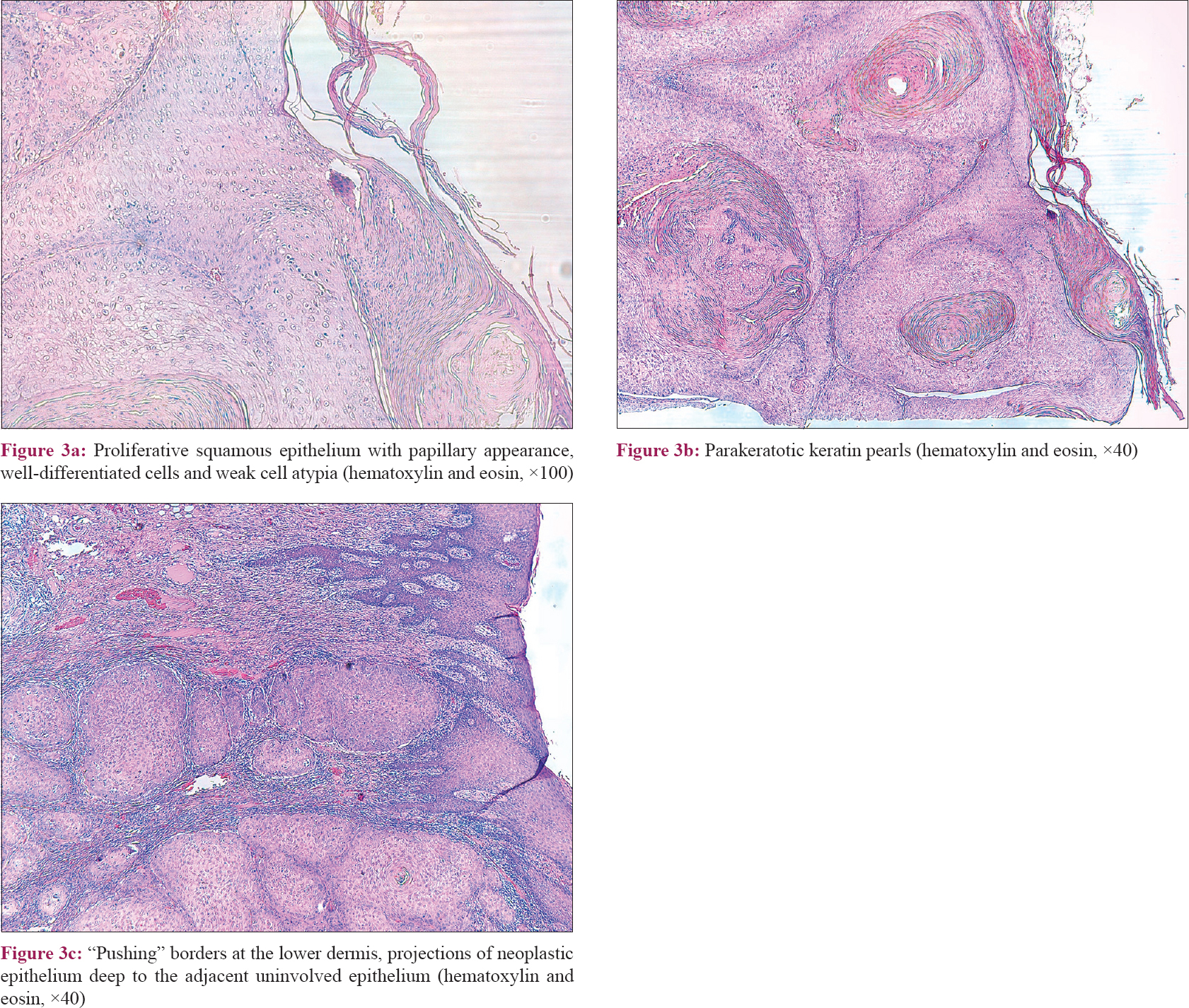 |
| Figure 3: |
Oral verrucous carcinoma accounts for 2–12% of all oral carcinomas and typically occurs in elderly males over the age of 60. Buccal and alveolar mucosa, tongue and lips are the usually involved sites.[1],[2] The etiology of oral verrucous carcinoma is not clear and the involvement of human papillomavirus in the pathogenesis is controversial. The used methods have variable sensitivity and specificity and in most studies, the number of cases is low. On the one hand, several studies report prevalence of human papillomavirus in a variable proportion of verrucous carcinoma,[3] while some authors found no association with this infection.[4] The multicentric nature of this tumor and the coexistence with a second primary tumor or premalignant lesions as proliferative verrucous leukoplakia are emphasized in recent literature and are probably related with field cancerization and can explain the frequent recurrence of this tumor.[5] Clinicopathological correlation is essential for the diagnosis. Oral verrucous carcinoma is characterized histologically by the absence of dysplastic cytological features and well-defined “pushing” borders that push downward the basement membrane without clear invasion. When invasive tumor cells through basement membrane are observed, it is classified as verrucous squamous cell carcinoma or hybrid verrucous carcinoma. The differential diagnosis between verrucous carcinoma and proliferative verrucous leukoplakia is challenging because of their similar morphologies in clinical and histopathological aspects. From the clinical standpoint, both could have an exophytic verrucous appearance. Histologically, proliferative verrucous leukoplakia exhibits an exophytic growth pattern and verrucous carcinoma combines exophytic and endophytic growth where the projections of neoplastic epithelium are seen deep to the adjacent uninvolved epithelium.[2] Proliferative verrucous leukoplakia has a high malignant transformation rate. The precise frequency of different malignancies arising in proliferative verrucous leukoplakia is not well established. The largest series report a malignant transformation rate of 10–30% to verrucous carcinoma and 50–70% to squamous cell carcinoma after a period of about 6 years.[6] Over time and without treatment, there is an inexorable progression to verrucous carcinoma or squamous cell carcinoma.
The authors report a case of a rare tumor with an unusual and exuberant presentation. The interest of this case is to gather some of the striking features of verrucous carcinoma: the difficulty of diagnosis, the multicentric nature and the lack of pathophysiological determinants such as human papillomavirus infection. Verrucous carcinoma remains an etiopathogenic, diagnostic and therapeutic challenge for dermatologists.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her image and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Walvekar RR, Chaukar DA, Deshpande MS, Pai PS, Chaturvedi P, Kakade A, et al. Verrucous carcinoma of the oral cavity: A clinical and pathological study of 101 cases. Oral Oncol 2009;45:47-51.
[Google Scholar]
|
| 2. |
Peng Q, Wang Y, Quan H, Li Y, Tang Z. Oral verrucous carcinoma: From multifactorial etiology to diverse treatment regimens (Review). Int J Oncol 2016;49:59-73.
[Google Scholar]
|
| 3. |
Fujita S, Senba M, Kumatori A, Hayashi T, Ikeda T, Toriyama K, et al. Human papillomavirus infection in oral verrucous carcinoma: Genotyping analysis and inverse correlation with p53 expression. Pathobiology 2008;75:257-64.
[Google Scholar]
|
| 4. |
Patel KR, Chernock RD, Zhang TR, Wang X, El-Mofty SK, Lewis JS Jr., et al. Verrucous carcinomas of the head and neck, including those with associated squamous cell carcinoma, lack transcriptionally active high-risk human papillomavirus. Hum Pathol 2013;44:2385-92.
[Google Scholar]
|
| 5. |
Gokavarapu S, Parvataneni N, Charan CR, Puthamakula S, Kulkarni G, Reddy BS, et al. Multi centricity of oral verrucous carcinoma: A case series of 22 cases. Indian J Otolaryngol Head Neck Surg 2015;67:138-42.
[Google Scholar]
|
| 6. |
Capella DL, Gonçalves JM, Abrantes AA, Grando LJ, Daniel FI. Proliferative verrucous leukoplakia: Diagnosis, management and current advances. Braz J Otorhinolaryngol 2017;83:585-93.
[Google Scholar]
|
Fulltext Views
4,294
PDF downloads
3,540





![[Figure - 1]](#fig_ijdvl_2020_86_2_230_257612_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_2_230_257612_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_2_230_257612_f3.jpg){kind=link}