Translate this page into:
Verrucous eccrine angiomatous hamartoma
2 Department of Pathology, Indian Council of Medical Research, New Delhi, India
Corresponding Author:
Prashant Verma
9 State Bank Colony, G.T. Karnal Road, New Delhi - 110 009
India
drprashant_derma@yahoo.co.in
| How to cite this article: Verma P, Kaur M, Narula V, Ramesh V, Singh A, Saxena A K. Verrucous eccrine angiomatous hamartoma. Indian J Dermatol Venereol Leprol 2017;83:367-369 |
Sir,
A 15-year-old girl presented with a lesion on her left thigh for the last 1 year. The lesion was associated with pain and hyperhidrosis which was often provoked by physical activity and emotional stress. Systemic examination was normal.
Cutaneous examination revealed a 9 cm × 6 cm, bluish-black, verrucous, firm plaque on the medial aspect of left thigh [Figure 1a]. The margins of the plaque were irregular. The lesion was warm and tender. On stroking, the surface of the plaque showed oozing beads of a shiny, transparent and colorless fluid [Figure 1b]. The starch-iodide test was positive.
 |
| Figure 1a: Bluish-black, verrucous plaque on the medial aspect of left thigh |
 |
| Figure 1b: Beads of sweat on the surface of the plaque after stroking the lesion |
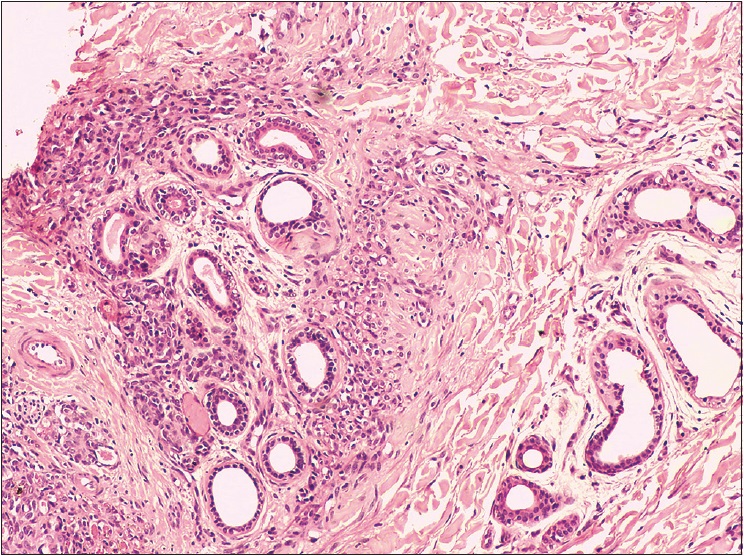
Biopsy from the plaque revealed hyperkeratosis and marked acanthosis with elongated rete ridges and increased epidermal basal layer melanin. The underlying dermis showed dilated eccrine glands and admixed capillaries within and around these glands [Figure 2a]. In addition, tufts and lobules of vascular proliferation with prominent endothelial cells and slit-like capillaries were present in the dermis [Figure 2b]. Accordingly, a diagnosis of eccrine angiomatous hamartoma was rendered. Surgical excision was planned for the patient; however, she was lost to follow-up.
 |
| Figure 2a: Hyperkeratosis, marked acanthosis and increased epidermal basal layer melanin with dilated eccrine glands and admixed capillaries within and around these glands (H and E, ×100) |
 |
| Figure 2b: Tufts and lobules of vascular proliferation with prominent endothelial cells and slit-like capillaries in the dermis (H and E, ×200) |
The term eccrine angiomatous hamartoma was coined by Hyman et al. in the year 1968;[1] however, the clinical description was first put forward by Lotzbeck, in 1895 and the earlier name was sudoriparous angioma.[2] Eccrine angiomatous hamartoma is a rare, benign cutaneous proliferation of eccrine glands and thin-walled vascular channels. The lesions arise at birth or during childhood in 77% of cases.[3] Extremities, palms and soles in particular, are the usual sites affected.[4] Feet, face, neck and trunk may seldom be involved. Solitary, flesh-colored, blue-brown or reddish papules, plaques and nodules are characteristic. Occasionally, eccrine angiomatous hamartoma may manifest multiple lesions.[4] Pain and hyperhidrosis are reported in approximately 42% and 32%, respectively.[5] Interestingly, verrucous changes in the epidermis were noted in the present case which is a rare finding in eccrine angiomatous hamartoma.[6] Unencapsulated, dermal proliferation of mature-appearing eccrine secretory and ductal structures that are intimately associated with thin-walled angiomatous channels usually of a capillary nature but of variable size are the characteristic histopathological features of eccrine angiomatous hamartoma.[7] The exact etiology of this entity is not known. Some authors have proposed a pathophysiological model which considers it a biochemical fault in the interactions between differentiating epithelium and subjacent mesenchyme that gives rise to an abnormal proliferation of adnexal and vascular structures. It might be caused by abnormal induction of heterotypic dependency during organogenesis. Late-onset lesions are related to recurrent trauma.[8]
The differential diagnosis of eccrine angiomatous hamartoma includes tufted angioma, vascular malformations, macular telangiectatic mastocytosis, nevus flammeus, glomus tumor, smooth muscle hamartoma, congenital hamartoma of the eccrine sweat gland, eccrine nevus and single lesion of blue rubber bleb syndrome. These entities can be differentiated by histopathology. Of these, tufted angioma is a close differential as it may also manifest hyperhidrosis as seen in eccrine angiomatous hamartoma; however, histopathologically, tufted angioma shows a pandermal capillary proliferation with characteristic “cannon ball” appearance. Hypertrichosis, hyperhidrosis, pain or itching are valuable diagnostic clues. The natural history of eccrine angiomatous hamartoma is benign and typically slow-growing and hence, aggressive treatment is generally unwarranted. Simple excision is usually curative and is reserved for painful or cosmetically disfiguring lesions.[9] Deep excision with full-thickness grafting or amputation of a finger or toe may be required for symptom control in those with larger lesions on acral parts.[10] Botulinum toxin might be useful in hyperhidrotic cases.[11]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. | Hyman AB, Harris H, Brownstein MH. Eccrine angiomatous hamartoma. N Y State J Med 1968;68:2803-6. [Google Scholar] |
| 2. | Tanaka M, Shimizu S, Miyakawa S. Hypertrophic eccrine glands in eccrine angiomatous hamartoma produce gross cystic disease fluid protein 15. Dermatology 2000;200:336-7. [Google Scholar] |
| 3. | Cebreiro C, Sánchez-Aguilar D, Gómez Centeno P, Fernández-Redondo V, Toribio J. Eccrine angiomatous hamartoma: Report of seven cases. Clin Exp Dermatol 1998;23:267-70. [Google Scholar] |
| 4. | Morrell DS, Ghali FE, Stahr BJ, McCauliffe DP. Eccrine angiomatous hamartoma: A report of symmetric and painful lesions of the wrists. Pediatr Dermatol 2001;18:117-9. [Google Scholar] |
| 5. | Martinelli PT, Tschen JA. Eccrine angiomatous hamartoma: A case report and review of the literature. Cutis 2003;71:449-55. [Google Scholar] |
| 6. | Galan A, McNiff JM. Eccrine angiomatous hamartoma with features resembling verrucous hemangioma. J Cutan Pathol 2007;34 Suppl 1:68-70. [Google Scholar] |
| 7. | Fathaddin AA, Alhumidi AA. Eccrine angiomatous hamartoma, with verrocous hemangioma-like features: A case report. Int J Health Sci (Qassim) 2013;7:103-6. [Google Scholar] |
| 8. | Zeller DJ, Goldman RL. Eccrine-pilar angiomatous hamartoma. Report of a unique case. Dermatologica 1971;143:100-4. [Google Scholar] |
| 9. | Lin YT, Chen CM, Yang CH, Chuang YH. Eccrine angiomatous hamartoma: A retrospective study of 15 cases. Chang Gung Med J 2012;35:167-77. [Google Scholar] |
| 10. | Gabrielsen TO, Elgjo K, Sommerschild H. Eccrine angiomatous hamartoma of the finger leading to amputation. Clin Exp Dermatol 1991;16:44-5. [Google Scholar] |
| 11. | Barco D, Baselga E, Alegre M, Curell R, Alomar A. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol 2009;145:241-3. [Google Scholar] |
Fulltext Views
4,515
PDF downloads
2,174




