Translate this page into:
Which therapy works for melasma in pigmented skin: Lasers, peels, or triple combination creams?
Correspondence Address:
Kabir Sardana
466 Sector 28, Noida, Uttar Pradesh 201 303
India
| How to cite this article: Sardana K, Chugh S, Garg VK. Which therapy works for melasma in pigmented skin: Lasers, peels, or triple combination creams?. Indian J Dermatol Venereol Leprol 2013;79:420-422 |
Sir,
We read with interest the study of Kar, et al. [1] and considering the studies using lasers and triple combination creams (TC) [2],[3],[4],[5] and the continued, invariably futile attempt to tackle this recalcitrant disorder, we feel it is time to focus on the relative merits of various modalities in melasma. The fundamental assessment criterion of the largely subjective (melasma area severity index, MASI) and the objective (Mexameter) assessment is crucial for logical interpretation of results, but probably more important is the pigment in the skin which makes a huge difference in the results of any laser in pigmented skin [6] including melasma. In pigmented skin, the results are not as good as in western skin types as the pigment in the epidermis alters the laser physics dynamics. [7] In the study, the difference in the improvement of the peel group (40.44%) and the low fluence laser group (47.93%) was not markedly different though it apparently achieved statistical significance. [1] It would have been informative to know at which sitting did this difference emerge and the statistical comparison between the two groups is not mentioned in the plethora of tables in the text, which probably is an oversight. These results contrast with a similar study in Korean patients who have a markedly lighter skin tone than Indian skin. [2] Here, a split face design was used to compare the effects of glycolic acid (GA) peel with Qsw Nd: YAG lasers versus the GA peel group. This study in a Korean population (a lighter skin type) [2] should have logically delivered superior results but only a 32.6-37.4% improvement using the Mexameter readings and modified MASI was seen, compared with 22% and 16.7%, respectively, with the laser only. This study was a split face study and used an objective tool and the paradoxically superior results in Indian skin using just the pigment laser (40.44% [1] vs. 22% [2] ) and the even more remarkable results in the peel group [1] (40.44%) could be partly due to the subjective assessment tool, MASI. Inexplicably, the results achieved in the peel group [1] (40.44%) by Kar et al. are comparable to most of the laser interventions in melasma [2],[3],[4],[5] which have been used largely in the fairer skin types.
Though peels have been touted as a useful intervention, it is a universal "practical" experience that without TC creams, the results are not profound, especially in pigmented skin. This is probably as deep peels (papillary dermis level), which are useful in the common mixed dermal melasma cases, are difficult to use in Indian skin as they can cause profound PIH (post inflammatory hyperpigmentation). The Erbium YAG (Er: YAG) laser which has a calibrated dose depth (1 μj/cm 2 = 5 μm) was used in three cases to target the pigment in melasma cases with disappointing results though laser peel is believed to be better than chemical peels. Though a study from India found that GA peels with TC cream was inferior to GA peels, [6] this study was hampered by a poor study design and evaluation as it was done in an era where "evidence-based" dermatology was not in vogue. Moreover, it relied entirely on the "subjective" MASI scores. Hurley, et al.[8] conducted the first randomized, investigator-blinded, controlled, split-faced study and compared the use of hydroquinone alone with hydroquinone plus GA peels in a homogeneous (Hispanic) population using objective (photography, Mexameter readings, and MASI) and subjective measures. The authors found that though the combination of GA and hydroquinone (HQ) improved melasma, there were no significant differences in skin lightening between regimens. This highly accessed article (2266 times!) has brought forth the evident fact that probably the results of 4% HQ are better than the chemical peels used. It probably does not require a study to prove that a TC cream would have superior results to the chemical peel! This is highlighted by the studies where TC have been combined and compared with lasers and have been found to have superior results, [3],[4],[5] which probably puts a question mark on the unnecessary use of lasers in melasma. In fact when TC were used with lasers, the results were better which is probably because of the effect of the TC preparation [3],[4],[5] ! The study by Wind, et al. [4] showed that the effects of TC cream are probably as effective or superior to the laser used!
The lasers tried for melasma are usually the pigment-specific lasers (Q-switched and long-pulsed lasers and the intense pulse light [IPL] system) [Figure - 1]. [9],[10] Although more effective for the epidermal subtype, these systems have limited success in the therapy of dermal melasma and the mixed type which constitute the majority of patients in pigmented skin. [9],[10] "Laser toning" involves the use of large spot size, and a low-fluence Q-switched (QS) 1064-nm Nd: YAG laser (6-8 mm spot size, 1.6-2.3 J/cm 2 ) in the treatment of melasma. [10] There are two issues in this therapy, the first is that the success has been restricted largely to fairer skin types [10] and the Nd: YAG laser has a small spot size and its frequency makes overlapping and uniform application of the laser a cumbersome task. Moreover, prolonged treatments can lead to mottled depigmentation, [9],[10] which is difficult to manage especially in Indian skin types. Furthermore, relapse of melasma and, in some cases, rebound can occur. The treatment is further complicated by the frequent incidence of post-inflammatory hyperpigmentation and rapid recurrence upon exposure to sunlight. [1],[2],[3],[4],[5],[9],[10]
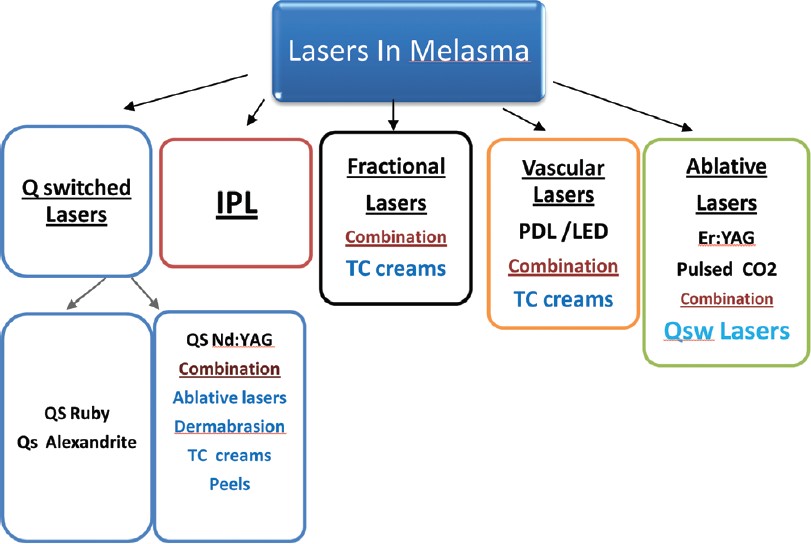 |
| Figure 1: A summary of the various lasers and adjunctive therapies used in melasma. QS: Q-switched |
Another approach is resurfacing with the pulsed CO 2 or Er: YAG laser, combined with a pigment-specific Q-switched laser, thus removing both the epidermal and dermal melanin [Figure - 1]. Our experience mirrors the views of other authors [9],[10] that the profound damage to the epidermis stimulates the melanocytes at the periphery resulting in post-inflammatory hyperpigmentation. Goldberg used a combined red/infrared light emitting diode therapy for 15-20 min following each IPL treatment to reduce recurrences. [9] We have used the IPL (three cases), QS Nd: YAG (two cases), fractional Er: Yag (seven cases), and ablative Er: YAG (two cases) but the results have been transient with rapid recurrence.
The "new kid on the block" is fractional resurfacing which in the initial studies had good results but our analysis mirrors the prevalent views [10] that fractional resurfacing has failed to achieve complete removal of the abnormal melanocytes in diseased skin, and its role is therefore adjunctive. Though fractional ruby laser has been explored for melasma in ′fair skin" Korean patients, [11] it is an addition to the plethora of laser devices in existence [Figure - 1], and the lack of long-lasting results does not augur well for the laser industry. Most of the fruitful results in melasma therapy are either augmented or as a consequence of the use of TC creams. [3],[4],[5],[8] Probably if studies in melasma are designed focusing on lasers and peels and compulsorily include a "arm" using TC creams, then this practical fact will be highlighted. The battle between the melanocytes and "man" is still to be won and probably melasma is in part a manifestation of nature′s compensation for geographical regions with a high tropical UV flux and thus attempts to treat it are rarely effective. It is to be emphasized that evidence-based literature still focuses entirely on TC creams and its rational use is the most cost-effective intervention. [8] Chemical peels and lasers are merely "cosmetic" adjuncts, [9],[10] whose cost-effectiveness is a justification for their restricted use specially in pigmented skin in tropical countries like India.
| 1. |
Kar HK, Gupta L, Chauhan A. A comparative study on efficacy of high and low fluence Q-switched Nd: YAG laser and glycolic acid peel in melasma. Indian J Dermatol Venereol Leprol 2012;78:165-71.
[Google Scholar]
|
| 2. |
Park KY, Kim DH, Kim HK, Li K, Seo SJ, Hong CK. A randomized, observer-blinded, comparison of combined 1064-nm Q-switched neodymium-doped yttrium-aluminium-garnet laser plus 30% glycolic acid peel vs. laser monotherapy to treat melasma. Clin Exp Dermatol 2011;36:864-70.
[Google Scholar]
|
| 3. |
Passeron T, Fontas E, Kang HY, Bahadoran P, Lacour JP, Ortonne JP. Melasma treatment with pulsed-dye laser and triple combination cream: A prospective, randomized, single-blind, split-face study. Arch Dermatol 2011;147:1106-8.
[Google Scholar]
|
| 4. |
Wind BS, Kroon MW, Meesters AA, Beek JF, van der Veen JP, Nieuweboer-Krobotová L, et al. Non-ablative 1,550 nm fractional laser therapy versus triple topical therapy for the treatment of melasma: A randomized controlled split-face study. Lasers Surg Med 2010;42:607-12.
[Google Scholar]
|
| 5. |
Jeong SY, Shin JB, Yeo UC, Kim WS, Kim IH. Low-fluence Q-switched neodymium-doped yttrium aluminum garnet laser for melasma with pre-or post-treatment triple combination cream. Dermatol Surg 2010;36:909-18.
[Google Scholar]
|
| 6. |
Sarkar R, Kaur C, Bhalla M, Kanwar AJ. The combination of glycolic acid peels with a topical regimen in the treatment of melasma in dark-skinned patients: A comparative study. Dermatol Surg 2002;28:828-32.
[Google Scholar]
|
| 7. |
Sardana K, Chugh S, Garg V. Are Q-switched lasers for Nevus of Ota really effective in pigmented skin? Indian J Dermatol Venereol Leprol 2012;78:187-9.
[Google Scholar]
|
| 8. |
Hurley ME, Guevara IL, Gonzales RM, Pandya AG. Efficacy of glycolic acid peels in the treatment of melasma. Arch Dermatol 2002;138:1578-82.
[Google Scholar]
|
| 9. |
David JG. Pigmented lesions, tattoos, and disorders of hypopigmentation. In: Laser Dermatology: Pearls and Problems. I st ed. Massachusetts: Blackwell Publishing; 2008. p. 91-3.
[Google Scholar]
|
| 10. |
Henry HL. Pigmentation and hypopigmentation: Benign pigmented lesions. In: Christian Raulin, Syrus Karsai, editors. Laser and IPL Technology in Dermatology and Aesthetic Medicine. I st ed. London: Springer-Verlag; Berlin: Heidelberg; 2011. p. 151-53.
[Google Scholar]
|
| 11. |
Jang WS, Lee CK, Kim BJ, Kim MN. Efficacy of 694-nm Q-switched ruby fractional laser treatment of melasma in female Korean patients. Dermatol Surg 2011;37:1133-40.
[Google Scholar]
|
Fulltext Views
3,294
PDF downloads
2,046





![[Figure - 1]](#fig_ijdvl_2013_79_3_420_110771_u1.jpg){kind=link}