Translate this page into:
Wolf's isotopic nonresponse in healed herpes zoster in erythroderma
Correspondence Address:
Gunjan Verma
PGIMER and Dr Ram Manohar Lohia Hospital, New Delhi
India
| How to cite this article: Sinha S, Verma G, Sharma P K, Ahuja A. Wolf's isotopic nonresponse in healed herpes zoster in erythroderma. Indian J Dermatol Venereol Leprol 2018;84:217-220 |
Sir,
Wolf et al. introduced “isotopic nonresponse” to describe the absence of an eruption at the site of another, unrelated, and already healed skin disease.[1] Herein, we describe a case of chronic recurrent erythroderma secondary to atopic dermatitis but sparing the site of herpes zoster affected area, thus demonstrating Wolf's isotopic nonresponse phenomenon.
A 38-year-old male presented with diffuse redness and scaling all over the body for 3 months. He gave history of many such episodes involving the whole skin in the last 4 years. His father had bronchial asthma and patient had dry itchy skin since childhood. Repeated episodes left his skin dark thickened, with increased skin markings on flexural parts. Eight months prior to this episode, he had developed herpes zoster involving the right T11 dermatome. After treatment, the lesions had resolved with minimal scarring. General physical examination was normal. Cutaneous examination showed diffuse erythema with fine whitish scales and mild induration over most of his skin. The forehead and flexural areas were lichenified while the neck had a dirty grey appearance. However, there was only mild erythema and scaling in the right T11 segment, which was previously involved by herpes zoster [Figure - 1]. The patient had not noticed any area of sparing in the earlier similar episodes prior to the development of herpes zoster.
 |
| Figure 1: Wolf's isotopic nonresponse: Mild erythema and scaling of the previously affected zone by herpes zoster (Right. T11) while the corresponding area shows lichenification |
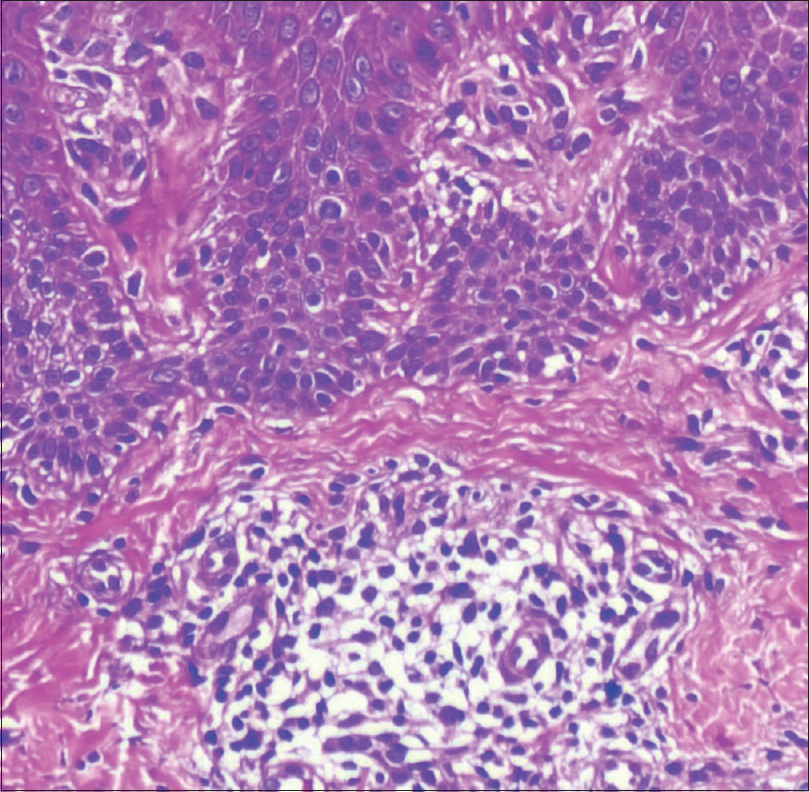
On investigation, complete hemogram was normal except eosinophilia (12%). Liver, renal, thyroid function tests, and urinalysis were in the normal range. Chest X-ray and electrocardiogram revealed no abnormalities, and Mantoux test was 5 × 5 mm. The serum immunoglobulin E level was >6400 IU/L (normal <70 IU/L). The skin biopsy from erythrodermic site showed mild hyperkeratosis, parakeratosis, acanthosis, and a dense dermal infiltrate of lymphocytes and eosinophils. The skin biopsy from the spared zoster site showed thinned epidermis and scanty dermal infiltrate with absence of eosionphils [Figure - 2]a,[Figure - 2]b,[Figure - 2]c,[Figure - 2]d. CD1a staining in the upper layer of the dermis was significantly more in the erythrodermic site. The intraepidermal region in the spared zoster site had few areas of staining for CD1a, while no such staining was present in the deeper dermis [Figure - 3]a and [Figure - 3]b.
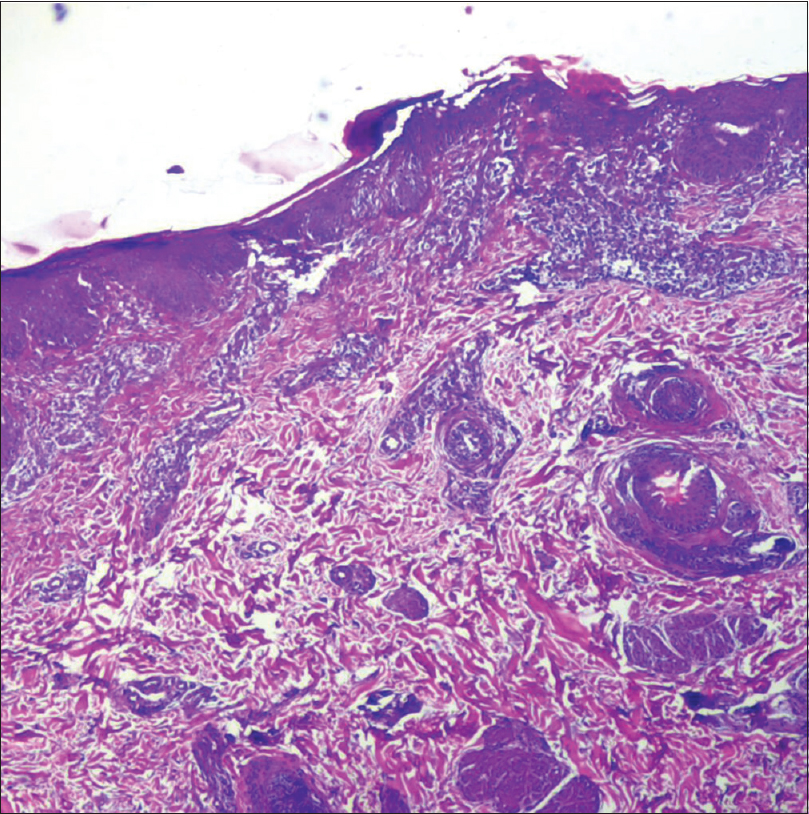 |
| Figure 2a: Dense infiltrate comprising lymphocytes and eosinophil in the dermis in erythrodermic site (×4) |
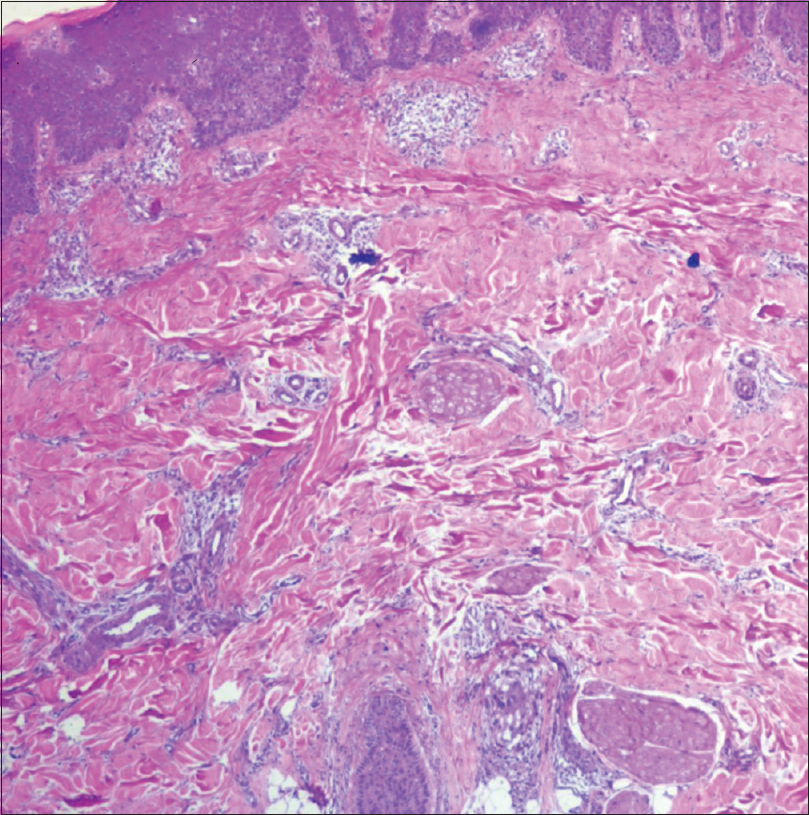 |
| Figure 2b: Scanty infiltrate in herpes zoster affected site (×4) |
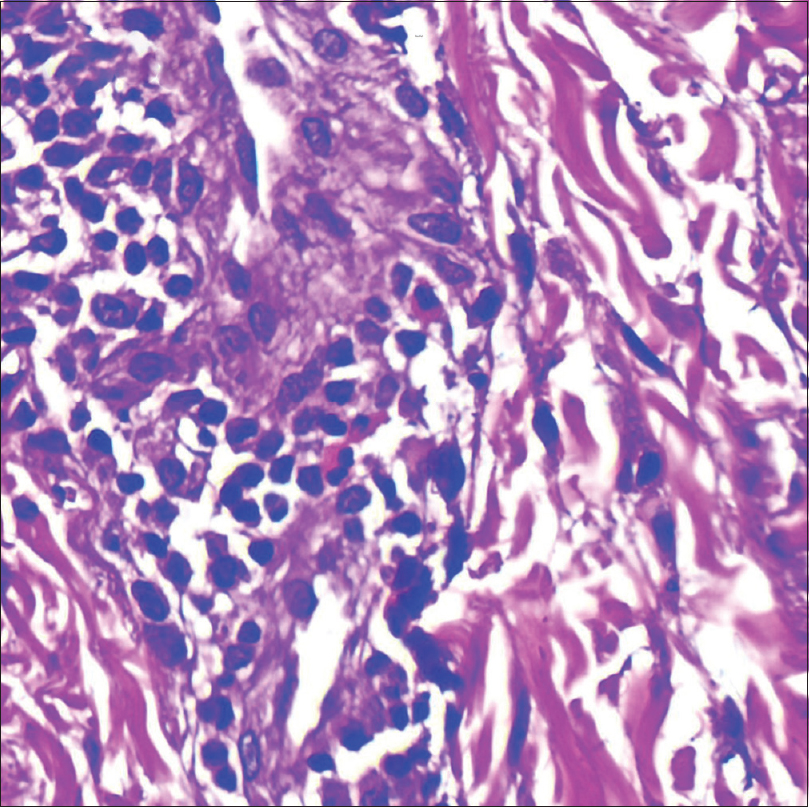 |
| Figure 2c: Lots of eosinophils in the erythrodermic skin (×40) |
 |
| Figure 2d: Absent eosinophils in herpes zoster affected site (×40) |
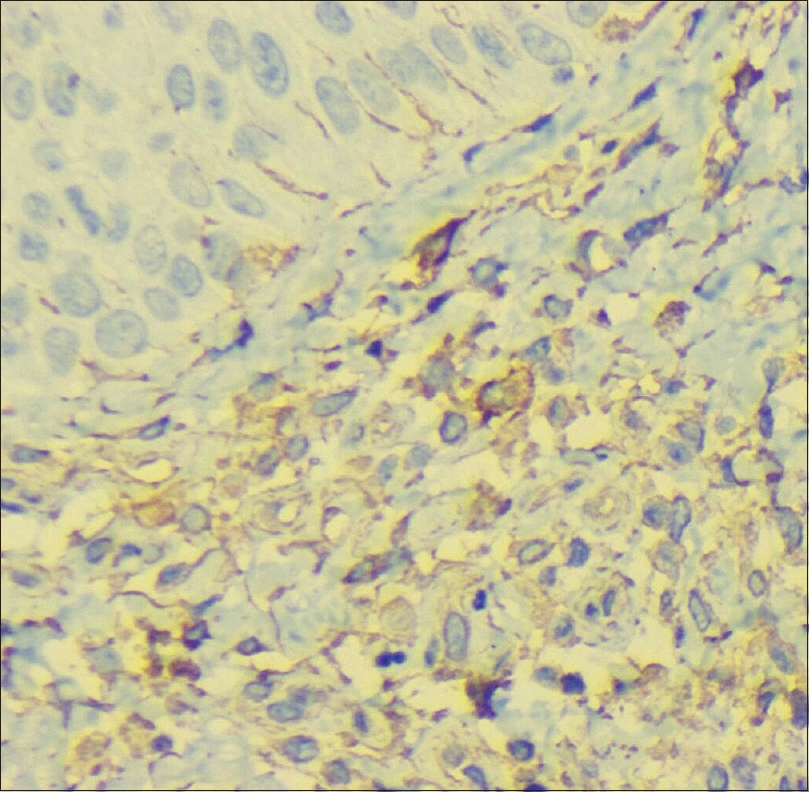 |
| Figure 3a: A significantly higher number of CD1a staining (immunohistochemistry) in the upper dermis in the erythrodermic site |
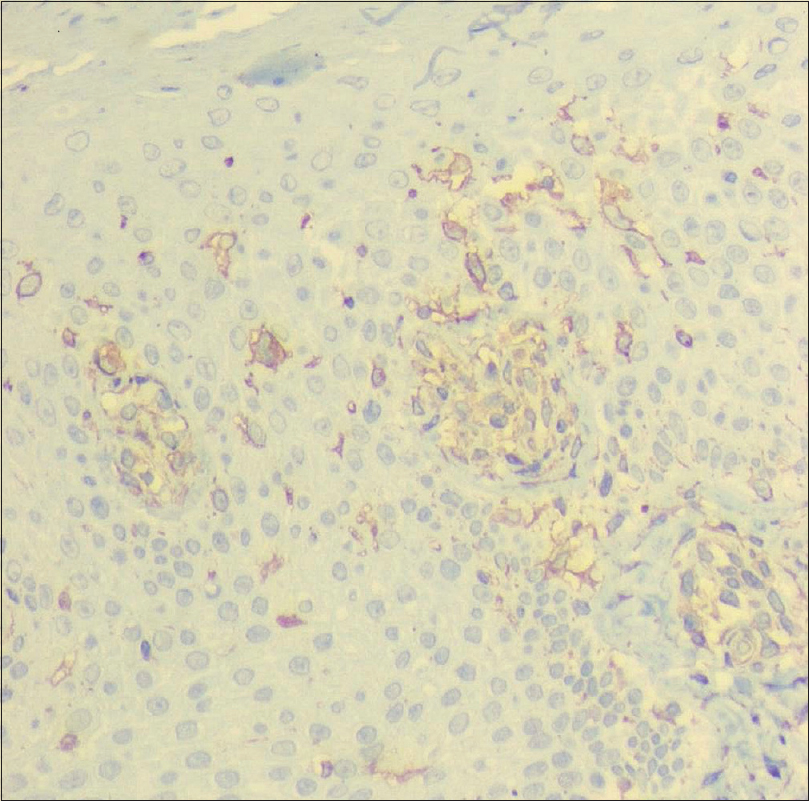 |
| Figure 3b: Compared to the healed zoster site having few areas of staining for CD1a, absent staining in the deeper dermis |
The term isotopic nonresponse is known as Wolf's postherpetic isotopic nonresponse because the most commonly spared lesion is a previous herpes infection. It is defined as the sparing of an eruption (dysimmune reactions, tumor spread) at the site of another unrelated and already healed skin disease (varicella zoster virus/herpes simplex virus).[2],[3],[4],[5] A large body of evidence has shown that the skin, the nervous system, and immunity are closely associated by cytokines and neuropeptides (neuroimmunocutaneous system). When this system is destabilized in a given district, by any cause (nerve lesion or infection, e.g. herpes zoster, amputation trauma, radiodermatitis), the district itself becomes a vulnerable site, prone to harbor locus minoris resistentiae or be rejected locus maioris resistentiae by a wide range of immunity-related disorders (opportunistic infections, primary or metastatic tumors, immune reactions). This innovative unifying concept has been termed as “the immunocompromised district.”[6] Postherpetic isotopic nonresponse is an example of locus maioris resistentiae. T regulator cells may persist at these sites and Langerhans cells may be less in number, and/or in antigen presenting capacity, which may further lead to increased resistance to dysimmune reactions at these sites. This pathomechanism possibly lies at the heart of the Wolf's isotopic nonresponse.[6] Our patient had decreased staining for CD1a in the previously zoster affected site vis-à-vis erythrodermic site. Also, eosinophils were lesser in the erythroderma-spared site in this case. Skin biopsies from the healed herpes zoster affected dermatomes in earlier studies have shown a similar reduction in the Langerhans cells and the dermal nerve network.[7],[8] Fukuda et al. also found lymphocytic infiltration, eosinophils, CD1a, and ICAM1 expressing cells to be lesser in the spared areas.[9]
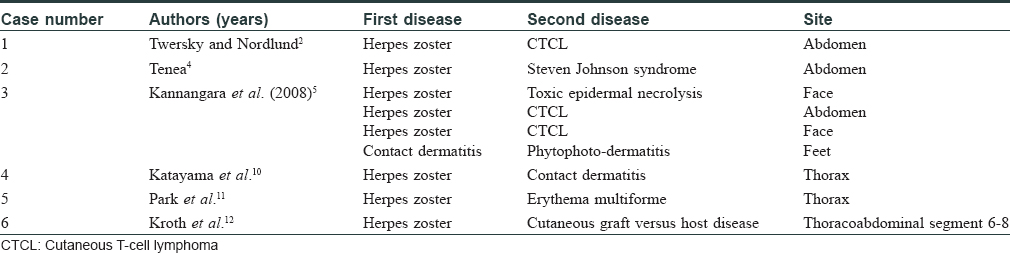
Twersky and Nordlund hypothesized that epidermotropic lymphocytes interact with Langerhans cells, and epidermotropism would be absent in areas without Langerhans cells.[2] Tenea et al. described similar sparing of herpes zoster virus area by Stevens Johnson syndrome due to carbamazepine, and they suggested that the virus increases Th1 cytokine profile with overexpression of tumor necrosis factor-α, interferon-γ, interleukin-2, and limits the presentation of viral peptides by major histocompatibility complex class I, II. [Table - 1] lists reports of this rare phenomenon in the literature. Most authors agree that decreased number of Langerhans cells and a dysregulated immune response (due to less antigen presentation) are probably responsible for the nonresponse.[10],[11],[12] To the best of our knowledge, there are no cases reported showing Wolf's isotopic nonresponse from India. How, if at all, the decreased numbers of the dermal Langerhans cells and denervation are responsible for the sparing of the previously healed herpes zoster site by generalized cutaneous eruptions can only be a matter of speculation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Wolf R, Brenner S, Ruocco V, Filioli FG. Isotopic response. Int J Dermatol 1995;34:341-8.
[Google Scholar]
|
| 2. |
Twersky JM, Nordlund JJ. Cutaneous T-cell lymphoma sparing resolving dermatomal herpes zoster lesions: An unusual phenomenon and implications for pathophysiology. J Am Acad Dermatol 2004;51:123-6.
[Google Scholar]
|
| 3. |
Kannangara AP, Fleischer AB Jr. Yosipovitch G, Ragunathan RW. Herpes zoster virus associated 'sparing phenomenon': Is it an innate possess of HZV or keratinocyte cytokine (s) mediated or combination? J Eur Acad Dermatol Venereol 2008;22:1373-5.
[Google Scholar]
|
| 4. |
Tenea D. Carbamazepine-induced Stevens-Johnson syndrome sparing the skin previously affected by herpes zoster infection in a patient with systemic lupus erythematosus: A reverse isotopic phenomenon. Case Rep Dermatol 2010;2:140-5.
[Google Scholar]
|
| 5. |
KannangaraAP, Fleischer AB, Yosipovitch G. The sparing phenomenon. A case series of the inverse Koebner and related phenomena. Our Dermatol Online2013;4:35-9.
[Google Scholar]
|
| 6. |
Ruocco V, Brunetti G, Puca RV, Ruocco E. The immunocompromised district: A unifying concept for lymphoedematous, herpes-infected and otherwise damaged sites. J Eur Acad Dermatol Venereol 2009;23:1364-73.
[Google Scholar]
|
| 7. |
Muller SA, Winkelmann RK. Cutaneous nerve changes in zoster. J Invest Dermatol 1969;52:71-7.
[Google Scholar]
|
| 8. |
Oaklander AL. The density of remaining nerve endings in human skin with and without postherpetic neuralgia after shingles. Pain 2001;92:139-45.
[Google Scholar]
|
| 9. |
Fukuda H, Sato Y, Usami N, Yokouchi Y, Mukai H. Contact dermatitis caused by bufexamac sparing the eruption of herpes zoster. J Dermatol 2012;39:405-7.
[Google Scholar]
|
| 10. |
Katayama H, Karube S, Ueki Y, Yaoita H. Contact dermatitis sparing the eruption of herpes zoster and its periphery. Dermatologica 1990;181:65-7.
[Google Scholar]
|
| 11. |
Park H, Kang Y, Lee U. Erythema multiforme sparing regressing herpes zoster lesion: “Reverse isotopic phenomenon?” J Am Acad Dermatol 2008;58:AB40.
[Google Scholar]
|
| 12. |
Kroth J, Tischer J, Samtleben W, Weiss C, Ruzicka T, Wollenberg A, et al. Isotopic response, Köbner phenomenon and Renbök phenomenon following herpes zoster. J Dermatol 2011;38:1058-61.
[Google Scholar]
|
Fulltext Views
3,407
PDF downloads
1,891





![[Figure - 1]](#fig_ijdvl_2018_84_2_217_224642_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_2_217_224642_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_2_217_224642_f3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2018_84_2_217_224642_t8.jpg){kind=link}