
Translate this page into:
Wound infection by Pantoea agglomerans after penetrating plant injury
-
Received: ,
Accepted: ,
How to cite this article: Olmos-Alpiste F, Martín-Ezquerra G, Pujol RM. Wound infection by Pantoea agglomerans after penetrating plant injury. Indian J Dermatol Venereol Leprol 2022;88:633-5.
Abstract
Pantoea agglomerans is a ubiquitous gram-negative bacterium that has been linked to skin and joint infections secondary to plant injuries. Herein we report a 58-year-old woman who presented with 2 erythematous nodules with purulent discharge on the anterior aspect of the right leg that developed after a penetrating plant injury. The patient was initially treated with amoxicillin-clavulanic acid, cloxacillin and clindamycin without improvement. P. agglomerans was isolated from both exudate and skin biopsy cultures. Healing of the lesions was achieved after the spontaneous release of a retained plant fragment and treatment with cotrimoxazole. Identification of P. agglomerans in persistent exudative lesions should alert the clinician regarding a possible previous plant injury and retained vegetal fragments. Conventional antibiotic treatment and the extraction of retained foreign bodies usually lead to complete resolution.
Keywords
Foreign body
Pantoea agglomerans
vegetal trauma
wound infection

Introduction
Pantoea agglomerans, formerly known as Enterobacter agglomerans or Erwinia herbicola, is a facultative anaerobic gram-negative bacillus belonging to Enterobacteriaceae family.1 It has been linked to skin and joint infections secondary to plant injuries. P. agglomerans should be suspected as the etiologic agent in cases of penetrating trauma by vegetal matter that remains refractory to conventional antimicrobial therapy.
Case Report
A 58-year-old woman presented to our Department for evaluation of two painful exudative nodules over her right leg. The patient worked as a biologist in a National Park in Congo and reported a penetrating injury with a plant on the anterior aspect of the lower right leg 3 weeks before consultation. She had a febrile episode 48 hours after injury and shortly after she noticed a discrete swelling and the appearance of an ill-defined erythematous raised lesion with purulent discharge at the wound site. She was initially treated with amoxicillin-clavulanic acid for 7 days, and afterwards with clindamycin and cloxacillin without definite improvement. Debridement was also attempted on a fluctuant abscess distally, but yielded no purulent material and led to the formation of the second ulcerated nodule.
Physical examination revealed an apparently healthy patient with two erythematous ulcerated nodules, 3 cm in diameter each with central purulent discharge on the outer aspect of the right leg [Figure 1a]. No enlarged regional lymph nodes were present and no similar lesions were noted elsewhere.

- Diffuse swelling and two erythematous nodules on the lateral aspect of the right leg, with central ulceration and purulent discharge
A 4mm punch biopsy revealed epidermal necrosis and ulceration accompanied by dermal lymphohistiocytic infiltrate with occasional neutrophils and eosinophils. Gram, Periodic acid-Schiff, Ziehl-Neelsen and Grocott stains did not show microorganisms [Figure 2]. Two cultures of the purulent exudate were performed, along with biopsy cultures for bacteria, fungi and mycobacteria. Pantoea agglomerans was isolated in Chocolate agar PolyViteX (CHOC-PVX) and MacConkey cultures from both exudate and biopsy samples, showing sensitivity to amoxicillin-clavulanic acid, ciprofloxacin, clindamycin, cotrimoxazole, cephalosporins and aminoglycosides. After a careful examination, a 0.6 x 6cm brownish plant fragment was observed to emerge spontaneously from the proximal ulcer, being later identified as belonging to Haumania liebrechtsiana, a plant present in Congo, Gabon, Democratic Republic of Congo and Angola [Figure 1b]. Treatment with cotrimoxazole 160/800 mg twice a day for 21 days was prescribed leading to clinical improvement within 5 days and complete resolution of the lesions in one month.

-
Haumania liebrechtsiana retained plant fragment
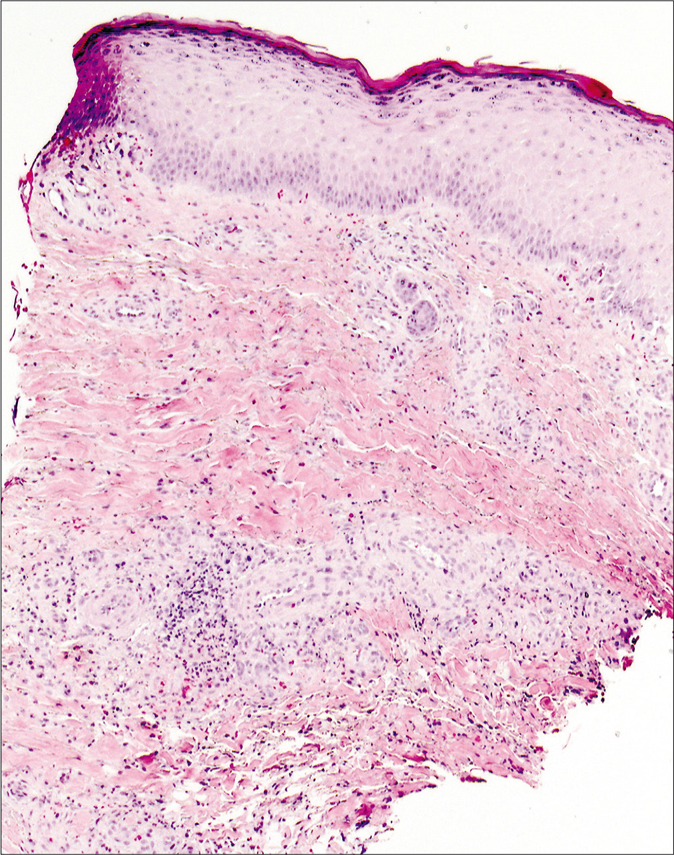
- Epidermal necrosis and ulceration accompanied by dermal lymphohistiocytic infiltrates with occasional neutrophils and eosinophils (H and E, ×100)
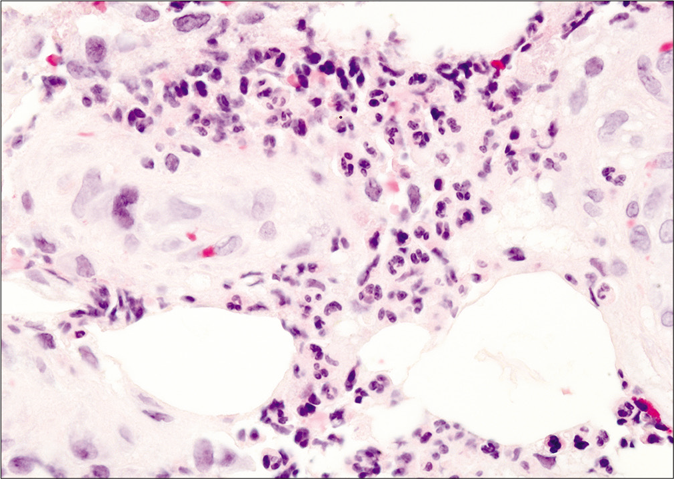
- Close-up view showing a perivascular lymphohistiocytic infiltrate with abundant neutrophils (H and E, ×400)
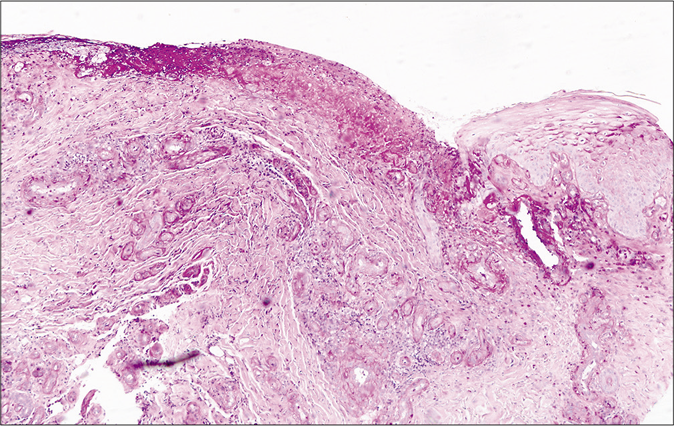
- Additional stains did not show the presence of any microorganism (Periodic Acid Schiff stain, ×100)
Discussion
Pantoea agglomerans, initially considered a ubiquitous contaminant (usually isolated from plants, fruits, vegetables, soil or animal feces), is nowadays considered a potential opportunistic pathogen giving rise to infections in two particular scenarios: a) local or regional infections after inoculation following a trauma with vegetal matter and b) disseminated infections in hospitalized immunosuppressed patients.2,3
Several nosocomial P. agglomerans epidemics in the form of bacteremia secondary to exposure to contaminated materials, hip prosthesis infections, endophthalmitis, peritonitis, pneumonias and hepatic abscesses have been described.2,3 Furthermore, P. agglomerans has been related to skin and joint infections after a penetrating trauma with a plant thorn or material often as a result of recreational or professional exposure (agriculture, gardening). Several reports of cellulitis and wound infections have been described.4,5 Inflammatory changes may appear several weeks or even months after trauma and, depending on the site or depth of injury, septic arthritis,6 synovitis,7 soft tissue infection or even periostitis and osteomyelitis2 may develop.
Histopathological examination often shows nonspecific findings, with dense dermal lymphohistiocytic infiltrate with a variable number of neutrophils. Plant-related fragments (splinter, thorns) may be identified, which can be accompanied by a foreign body granulomatous response with abundant histiocytes and multinucleated giant cells.8 In our case, the retained foreign body was deeply located and skin biopsy showed only a non-specific inflammatory infiltrate and failed to detect foreign bodies.
A previous history of plant injury and the observation of persistent inflammatory changes, erythematous nodules or suppurative ulcers refractory to conventional antimicrobial therapy should raise the diagnostic suspicion of wound infection by P. agglomerans. However, in some instances, previous trauma may be unnoticed and the definitive diagnosis could only be established after the isolation of P. agglomerans from the exudate.
In a proportion of cases, retained thorns or plant fragments are present and extraction of these foreign bodies seem mandatory for healing.9 However, the radiolucent nature and a possible migration beyond the inoculation site may hinder their identification. Imaging tests such as ultrasonography or magnetic resonance imaging can be useful tools to identify and locate retained foreign materials.4,5,10
P. agglomerans is usually sensitive to synthetic penicillins, ciprofloxacin, gentamicin, third-generation cephalosporins and cotrimoxazole and may show resistance to ampicillin and to first- and second-generation cephalosporins due to beta-lactamase production.1 Although isolated reports of successful treatment with cotrimoxazole has been described, whenever possible, treatment should be guided by antibiotic sensitivity results.5 The removal of the retained foreign bodies combined with antibiotic therapy, seems to be the most effective treatment to achieve a complete and rapid recovery. In our case, the initial lack of response to amoxicillin-clavulanic acid treatment was probably due to the persistence of the retained foreign body.
An increased awareness regarding this clinical picture seems important. In order to avoid unnecessary diagnostic delays, promptly detect and remove retained plant fragments, and prescribe adequate antibiotic treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Pantoea agglomerans, a plant pathogen causing human disease. J Clin Microbiol. 2007;45:1989-92.
- [CrossRef] [PubMed] [Google Scholar]
- Pantoea agglomerans: A mysterious bacterium of evil and good, Part III. Deleterious effects: Infections of humans, animals and plants. Ann Agric Environ Med. 2016;23:197-205.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical and microbiological characteristics of Pantoea agglomerans infection in children. J Infect Public Health. 2018;11:304-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pantoea agglomerans-An underestimated pathogenic agent in penetrating trauma involving vegetative material. J Eur Acad Dermatol Venereol. 2016;30:1025-6.
- [CrossRef] [PubMed] [Google Scholar]
- Retained hawthorn fragment in a child's foot complicated by infection: Diagnosis and excision aided by localization with ultrasound. J Foot Ankle Surg. 2010;49:161-5.
- [CrossRef] [PubMed] [Google Scholar]
- Isolation of Pantoea agglomerans in two cases of septic monoarthritis after plant thorn and wood sliver injuries. J Clin Microbiol. 2000;38:460-1.
- [Google Scholar]
- Case report: Subacute synovitis of the knee after a rose thorn injury: Unusual clinical picture. Clin Orthop Relat Res. 2008;466:3138-42.
- [CrossRef] [PubMed] [Google Scholar]
- Pantoea agglomerans as an indicator of a foreign body of plant origin in cases of wound infection. J Wound Care. 2013;22:182, 184-5
- [CrossRef] [PubMed] [Google Scholar]
- Pantoea agglomerans as a cause of septic arthritis after palm tree thorn injury; case report and literature review. Arch Dis Child. 2003;88:542-4.
- [CrossRef] [PubMed] [Google Scholar]




