Translate this page into:
Zosteriform lesion over abdomen
Correspondence Address:
S Chidambara Murthy
Department of Dermatology and Venereology, S. N. Medical College and HSK Hospital and Research Centre, Navanagar, Bagalkot 587 102, Karnataka
India
| How to cite this article: Murthy S C. Zosteriform lesion over abdomen. Indian J Dermatol Venereol Leprol 2006;72:245-246 |
 |
|
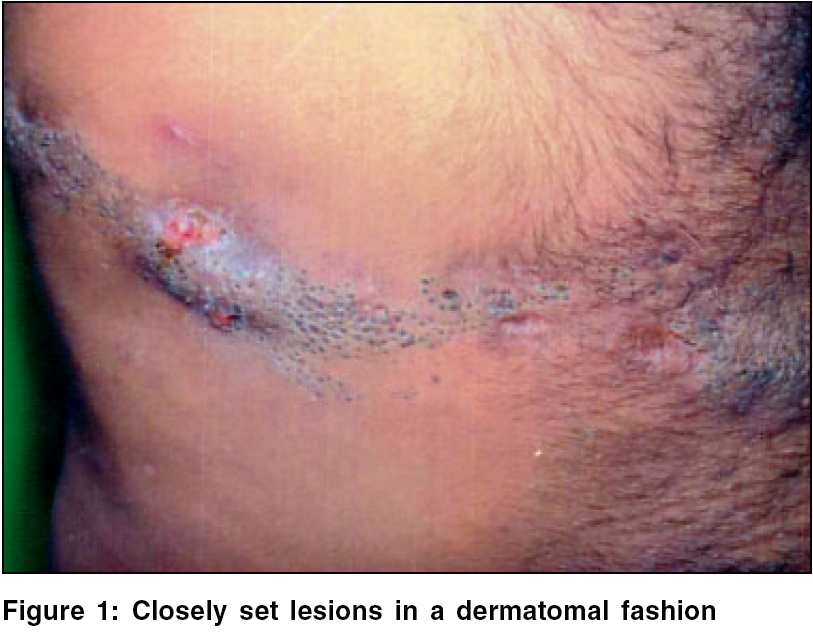
A 29-year-old male patient presented with a lesion over the right side of abdomen since birth. He had noticed a painful swelling with discharge, arising within the lesion for the last 4 days. Patient recalled of having suffered from similar episodes in the past, which used to subside with antibiotics and anti-inflammatory drugs. There was no history of skeletal, ocular or other systemic involvement. Family history was unremarkable. Cutaneous examination showed multiple, closely set pits of varying sizes with dark keratinous plugs arranged in unilateral distribution along the right T 8 dermatome [Figure - 1]. An intervening cystic inflammatory swelling with mucopurulent discharge and multiple atrophic areas was present. Systemic examination was normal.
His routine hematological, urine and biochemical examinations were normal. Chest X-ray, including X-ray of the affected part, was normal. Culture from discharge showed growth of Staphylococcus aureus . A skin biopsy from a representative site showed epidermal invaginations filled with concentric lamellae of keratin with minimal dermal inflammation
What is your diagnosis?
Diagnosis: Nevus comedonicus
Discussion
Nevus comedonicus is a developmental abnormality of the skin comprising numerous keratin-filled pits.[1] It is a rare abnormality of the skin, first described by Kofmann in 1895 as ′comedo nevus′.[2] It has many synonyms, including ′nevus acneiformis unilateralis,′ ′nevus a comedons,′ ′nevus folliculoris keratosus′[2] and ′nevus zoniforme′.[3]
Nevus comedonicus is a hamartoma; it does not contain true nevus cells.[3] It is the result of a defect in the development of the hair follicle. There is a defect or failure in the development of the mesodermal component of the pilosebaceous complex with associated imperfect differentiation of the epithelial component. The resultant follicular structure is capable of forming only soft keratin, which plugs the adnexal orifice and produces the comedones.[2]
The lesions may develop any time from birth to middle age but are usually present at birth or develop before the age of 10 years. Both sexes are equally affected. There is no familial or racial predilection.[4]
Comedo nevi comprise groups of pits filled with black keratinous plugs resembling blackheads. There may be one or several lesions in a linear, unilateral or more rarely, bilateral distribution.[1] There may be gradual extension of lesions throughout life, even after years of quiescence.[3] The most frequently affected site is the face, followed by the neck, trunk and upper arm. Rarely, non-hairy regions like palms, soles and glans are involved.[1] Lesions usually follow the course of a nerve or are localized to a single dermatome.[3]
Histopathology shows epithelial invagination into the corium, thinning of epidermis, which seems to impart a thin lining to the keratinous cysts. There may be absence or decrease of pilosebaceous elements.[3]
Complications include chronic inflammation, suppuration, fistula formation and hypertropic scarring. Rarely, benign and malignant tumors may arise. It can be associated with skeletal malformations, ocular involvement or CNS involvement. The condition has to be differentiated from familial diffuse comedones, familial dyskeratotic comedones, linear basal nevus, dilated pore nevus.[1] Histologically, epithelioma adenoides cysticum is an important differential diagnosis.[3]
Different therapeutic modalities are available, but none of them is satisfactory. Options include wide surgical excision, dermabrasion,[3] regular use of a comedo extractor,[5] 12% ammonium lactate[6] and topical retinoic acid.[1]
| 1. |
Atherton DJ. Naevi and other developmental defects. In: Champion RH, Burton JL, Burns DA. Breathnach SM, editors. Rook/ Wilkinson/ Ebling Textbook of dermatology. 6th ed. Blackwell Science: Oxford; 1998. p. 531-3.
[Google Scholar]
|
| 2. |
Wood MG, Thew MA. Nevus comedonicus. A Case with palmar involvement and review of the literature. Arch Dermatol 1968;98:111-6.
[Google Scholar]
|
| 3. |
Loria PR, Hailey CW. Nevus follicularis keratosis (Comedo Nevus). Arch Dermatol 1961;83:991-4.
[Google Scholar]
|
| 4. |
Beerman HB, Homan JB. Nevus comedonicus. Arch Klin Exp Derm 1959;208:325-41.
[Google Scholar]
|
| 5. |
Beck MH, Dave VK. Extensive nevus comedonicus. Arch Dermatol 1980;116:1048-50.
[Google Scholar]
|
| 6. |
Milton GP, DiGiovanna JJ, Peck GL. Treatment of nevus comedonicus with ammonium lactate lotion. J Am Acad Dermatol 1989;20:324-8.
[Google Scholar]
|
Fulltext Views
3,203
PDF downloads
4,134





![[Figure - 1]](#fig_ijdvl_2006_72_3_245_25796_1.jpg){kind=link}