Translate this page into:
1. Solitary, horny projection on hand
2 Departments of Pathology, BLDEA's SBMP Medical College, Hospital and Research Centre, Bijapur, India
Correspondence Address:
Arun C Inamadar
Department of Dermatology, Venereology and Leprosy, BLDEA's SBMP Medical College, Hospital and Research Centre, Bijapur - 586103, Karnataka
India
| How to cite this article: Inamadar AC, Palit A, Sampagavi V V, Yelikar B R. 1. Solitary, horny projection on hand. Indian J Dermatol Venereol Leprol 2004;70:325-326 |
 |
|
 |
|
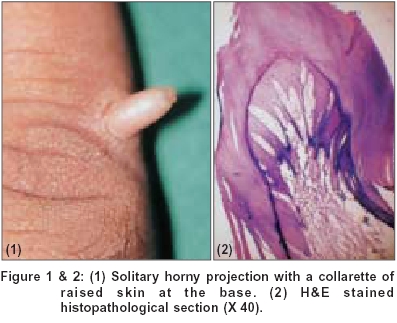
A middle aged motor mechanic presented with a horny projection on right little finger of two years duration. The lesion was asymptomatic except for physical inconveniences. On examination, a 0.5 cm long, non-tender, firm, skin coloured growth with a rough surface was found projected vertically from the ulnar border of right little finger [Figure - 1]. The base of the lesion was surrounded by a raised collarette of skin. Hematoxylin and eosin stained section of excision biopsy is shown in [Figure - 2].
What is the Diagnosis?
Answer to Quiz No. 1
Diagnosis: Acquired digital fibrokeratoma
The H & E stained histopathological section shows [Figure - 2] hyperkeratosis, acanthosis and branching rete ridges in the epidermis. The dermis (core of the lesion) showed thick collagen fibres and blood vessels arranged along the long axis of the lesion. Base of the lesion showed proliferation of numerous blood vessels. On the basis of histopathological findings, a diagnosis of acquired digital fibrokeratoma was made. There was no recurrence of the lesion on follow up.
DISCUSSION
Acquired digital fibrokeratoma presents as a solitary, elongated or dome-shaped lesion with a characteristic collarette of raised skin at the base.[1] Most common sites of occurrence are fingers and toes but lesions on palms and soles can occur. Often the lesion emerges from beneath the proximal nail fold with a narrow base and hyperkeratotic tip (acquired periungual fibrokeratoma). In the latter case, the lesions may be multiple and grow on the nail plate causing longitudinal grooves. Occasionally, acquired digital fibrokeratoma may be pedunculated and the surface may appear warty. The condition occurs solely in adults and is believed to result from trauma.[2]
Histopathologically, epidermis is hyperkeratotic and acanthotic. The core of the lesion is formed by thick, dense collagen bundles oriented across the vertical axis and scanty thin elastic fibers. Vascular proliferation may be observed.[3] Histopathological variations like increased number of fibroblasts and dermal edema separating collagen fiber bundles may be observed.[4]
Clinically the condition may be mistaken as a rudimentary, supernumerary digit, which occurs at the base of the fifth finger, but is present since birth and usually bilateral. Histologically, presence of numerous nerve bundles at the base distinguishes the latter from acquired digital fibrokeratoma.[5] Other conditions to be differentiated are cutaneous horn, viral wart and dermatofibroma. Periungual lesions are to be differentiated from Koenen tumour of tuberous sclerosis.[6] The hyperkeratotic tip of the periungual lesion differentiates it from garlic clove fibroma.
The condition is benign and surgical excision is curative. Periungual lesions arising below proximal nail folds are to be excised with due care, not to damage the matrix, which may result in permanent nail dystrophy.[4]
| 1. |
Mackie RM. Soft tissue tumours. In: Champion RH, Burton JL, Burns DA, Breathnach SM, editors. Textbook of Dermatology. Vol-3, 6th Ed. Oxford: Blackwell Science; 1998. p. 2347-72.
[Google Scholar]
|
| 2. |
Berger RS, Spielvogel RL. Dermal papule on a distal digit. Arch Dermatol 1988;124:1559.
[Google Scholar]
|
| 3. |
Verallo VVM. Acquired digital fibrokeratomas. Br J Dermatol 1968;80:730.
[Google Scholar]
|
| 4. |
Dawber RPR, Baran R, Barker de D. Disorders of nails. In: Champion RH, Burton JL, Burns DA, Breathnach SM, editors. Textbook of Dermatology.Vol-4, 6th Ed. Oxford: Blackwell Science; 1998. p. 2815-68.
[Google Scholar]
|
| 5. |
Heenan PJ. Tumours of the fibrous tissue involving the skin. In: Elder D, Elenitsas R, Jaworsky C, Johnson B Jr., editors. Lever's Histopathology of Skin. 8th Ed. Philadelphia: Lippincott-Raven; 1997. p. 847-87.
[Google Scholar]
|
| 6. |
Kint A, Baron R. Histopathologic study of Koenen tumours. Are they different from acquired digital fibrokeratoma? J Am Acad Dermatol 1988;18:369-72.
[Google Scholar]
|
Fulltext Views
2,950
PDF downloads
2,212





![[Figure - 1]](#fig_ijdvl_2004_70_5_325_12854_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2004_70_5_325_12854_2.jpg){kind=link}