Translate this page into:
Appraisal of transverse nasal groove: A study
Correspondence Address:
Belagola D Sathyanarayana
Department of Dermatology, Adichunchanagiri Institute of Medical Sciences, BG Nagara, Karnataka - 571 448
India
| How to cite this article: Sathyanarayana BD, Basavaraj HB, Nischal KC, Swaroop MR, Umashankar PN, Agrawal DP, Swamy SS, Okram S. Appraisal of transverse nasal groove: A study. Indian J Dermatol Venereol Leprol 2012;78:439-442 |
Abstract
Background: Transverse nasal groove is a condition of cosmetic concern which awaits due recognition and has been widely described as a shallow groove that extends transversely over the dorsum of nose. However, we observed variations in the clinical presentations of this entity, hitherto undescribed in literature. Aims: We conducted a clinicoepidemiological study of transverse nasal lesions in patients attending our outpatient department. Methods: We conducted a prospective observational study. We screened all patients attending our out-patient department for presence of transverse nasal lesions, signs of any dermatosis and associated other skin conditions. Results: One hundred patients were recruited in the study. Females (80%) predominated over males. Most patients were of 15-45 years age group (70%). Majority of the transverse nasal lesions were classical transverse nasal groove (39%) and others included transverse nasal line (28%), strip (28%), ridge (4%) and loop (1%). Seborrhoeic diathesis was the most common condition associated with transverse nasal lesion. Conclusions: Occurrence of transverse nasal line, strip, ridge and loop, in addition to classical transverse nasal groove implies that latter is actually a subset of transverse nasal lesions. Common association of this entity with seborrheic dermatitis, seborrhea and dandruff raises a possibility of whether transverse nasal lesion is a manifestation of seborrheic diathesis.Introduction
Transverse nasal groove (TNG) was first described in 1951 by Cornbleet, as a minor cutaneous defect and has been referred to as transverse nasal strip, stria nasi transversa and transverse nasal line. [1],[2] They are well-demarcated grooves of 1-3-mm width and about 1-mm depth that extends transversely across the dorsum of nose, at the junction of upper two-third and lower one-third of the nose, just proximal to alae nasi. [3] They are more prominent in children and tend to improve spontaneously overtime during third and fourth decade of life and becomes less apparent and shallower; [3] finally by the end of fifth decade only a faint band of pigment may remain. [4] TNG seems to be more common than indicated, but because of its asymptomatic nature, only a few case reports have been published. [2],[3],[4],[5],[6] Sometimes the affected individuals may develop large patulous follicles, severe acne and scales within the groove. [4]
With increased aesthetic awareness among the general population, it is not infrequent that a dermatologist gets a patient with this concern. In addition to the classical description of this entity, we came across variations in its presentation which was not described in literature. Hence, we took up this study to appraise our knowledge regarding this interesting entity and its association with other dermatoses.
Methods
We conducted this prospective clinicoepidemiological observational study between January 2010 and May 2011 at our rural tertiary care center after ethical board approval. All patients attending the dermatology outpatient department were observed and screened for well-demarcated lesions present transversely across the nasal bridge proximal to alae nasi. Detailed pertinent history with respect to the onset, progression of the lesion, any associated dermatosis on the lesion or elsewhere, any treatment taken for the same was noted and thorough clinical examination was done. Duration of lesion and family history were given special emphasis. Signs of any disease or other dermatoses, if any, were noted and patient was evaluated and treated for the dermatosis, for which he/she had actually visited the dermatology clinic.
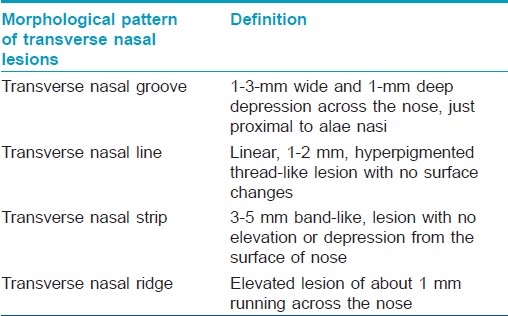
Transverse nasal lesions were closely observed and various morphological patterns were noted and classified as groove, line, strip or ridge [Table - 1]. Histopathological examination was not performed due to aesthetic concerns.
Results
During January 2010 to May 2011, 30552 cases were screened. A total of 100 consecutive patients with transverse nasal skin lesions were recruited in the study after informed consent (incidence 0.33%). TNG was found to be more common in females (80%). Study subjects were divided into five age groups and majority belonged to 15-30 years age group (42%), followed by 30-45 years (28%). Only one case presented in the age group of 60-75 years. Fifteen patients (15%) had family members with similar condition.
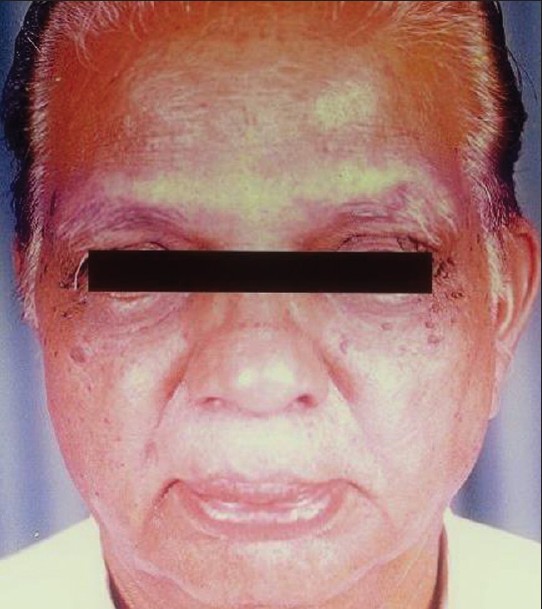
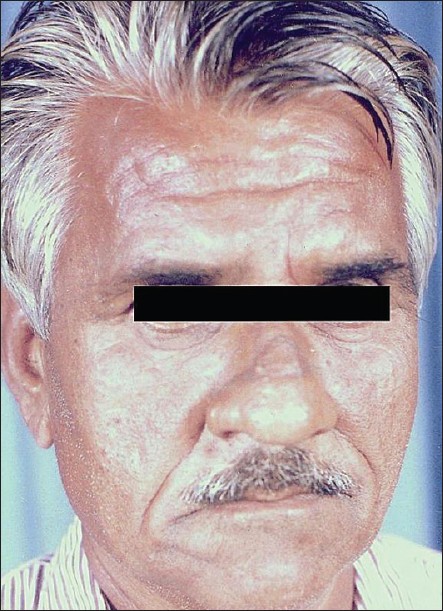
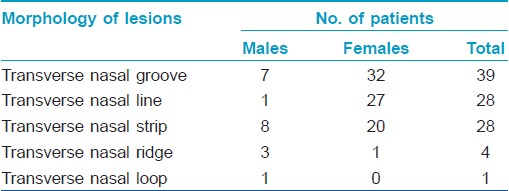
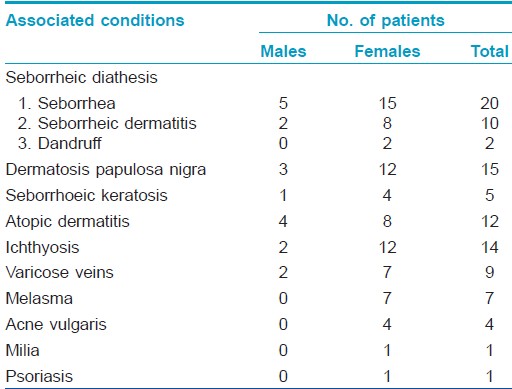
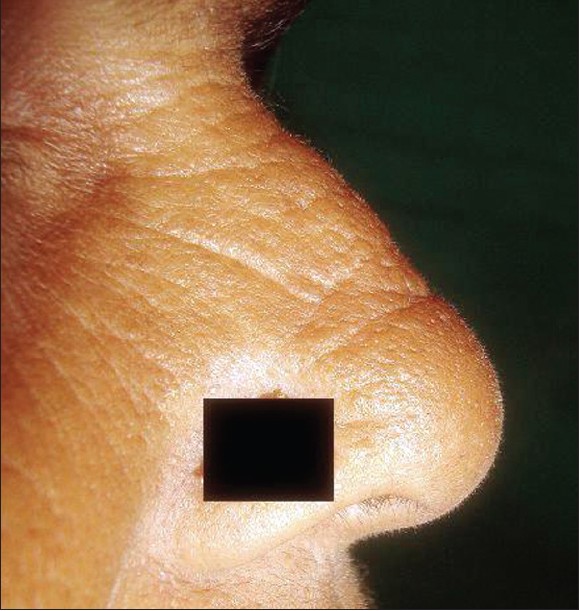
Majority of patients presented with classical TNG (39%) [Figure - 1]. An equal number of cases presented as transverse nasal line (28%) [Figure - 2] and transverse nasal strip (28%) [Figure - 3]. Four patients (4%) presented with transverse nasal ridge. The ridge was smooth in all patients but one, who had a beaded appearance [Figure - 4]. The beaded appearance was due to presence of patulous open comedones over the ridge. Lastly, in one case [Table - 2], in addition to the classical transverse nasal grove, we observed a loop-like groove which had its origin and end point in the nasolabial fold with its apex over the dorsal nasal bridge; thus forming a triangular area between the two grooves [Figure - 5]. Various other dermatological conditions observed in these patients were seborrheic diathesis, dermatosis papulosa nigra, seborrheic keratosis, ichthyosis, atopic dermatitis, acne vulgaris, milia and psoriasis [Table - 3]. Patients with seborrheic diathesis included those having seborrhea or seborrheic dermatitis or dandruff.
 |
| Figure 1: Transverse nasal groove with mild seborrheic dermatitis |
 |
| Figure 2: Transverse nasal line with melasma. |
 |
| Figure 3: Transverse nasal strip |
 |
| Figure 4: Transverse nasal ridge with seborrheic keratosis and achrochordons |
 |
| Figure 5: Transverse nasal groove with loop |
Discussion
TNG is rare cutaneous disorder, for which patients seldom presents to a dermatologist for its treatment. The incidence of transverse nasal lesions was 0.33% in our study group. It is totally asymptomatic and rarely bothersome to the patient. It has a higher preponderance for females over males (4:1). It occurs sporadically in general population. Familial cases have been reported. [3] In our study, we found 15% of positive family history which is quite significant.
Wimmershoff et al., reported two cases of TNG and both of his patients had onset of TNG since birth. [6] However, none of our patients gave similar history. In contrast to a higher incidence of TNG reported in children in previous western studies, [1],[3] we observed it to be more common in 15-45 year (70%) age group; this implies that this is a condition of adolescents and adults. This observation is in concordance with report of Pavithran. [4] We also observed a lower prevalence in older age groups, correlating with the previous studies. [4]
The exact etiology of this disorder is not known. It has been considered as an embryological defect, where, alar and triangular cartilages attach themselves in a linear transverse fashion. [2] Genetic origin has also been proposed. [3] We regard the occurrence of these lesions at the site of junction of the two upper lateral and two lower lateral cartilages of the nose. Both upper and lower lateral cartilages are attached to each other and the upper lateral cartilage to the undersurface of nasal bone by fibrous septa. The occurrence of lesions can be related to fibrous attachments present between the cartilage-cartilage and the bony-cartilaginous junctions. Clinically, most lesions observed in our study were present a few millimeters higher to the junction of upper two-third and lower one-third of the nose. There is a vague possibility of this clinical landmark coinciding with the point of attachment of the upper and lower lateral cartilages. This is because of variation in the size of both nasal bone and the cartilages in different individuals. The ratio in size of both the upper and lower lateral cartilages can also alter the position of this clinical landmark. A larger lower lateral cartilage will tend to shift the lesion upwards whereas a smaller cartilage may cause vice versa.
The location of an additional loop-like groove, mentioned above, can be related with the site of attachment of nasal bone and the two upper lateral cartilages which are attached together by fibrous septa, similar to the junction of two cartilages present below.
In one case, multiple transverse groove-like lesions were present over the nose. These lesions are basically wrinkles seen in old age or photoaging [Figure - 6]. In contrary to TNG, on stretching the skin between thumb and index finger, these lines become less prominent or flatten. In addition, these lesions were short, not extending to the full breadth of the nose, were multiple in numbers and also present over other areas of face. Two reports of multiple, short wrinkles or crease over the nose which disappear on stretching has been described with allergic rhinitis. [3],[7] TNG remains prominent even after skin is stretched.
 |
| Figure 6: Wrinkle of photoaging resembling transverse nasal groove |
The various morphological presentations of this entity were observed. Previously only a groove had been described. We, in our study observed lesions in the form of a line, strip, ridge and a loop in addition to the groove which was the most common presentation. This implies that, TNG is not a single entity but a subset of transverse nasal lesions.
We found seborrhea to be present in 20%, seborrheic dermatitis in 10% and dandruff in 2% of patients. Pavithran also found a very high incidence of seborrheic dermatitis (76.66%) in patients with TNG. Another common association noted was dermatosis papulosa nigra (15%). Ichthyosis was observed in 14% and atopic dermatitis in 12% of cases. A total 9% of cases presented with varicose veins. Overall, a seborrheic association of 32% has been found which is quite significant. With this data, TNG could be considered a manifestation of seborrheic diathesis.
In all, TNG is an interesting cutaneous defect and forms a subset of transverse nasal lesions which comprises of groove, line, strip, ridge and a loop. The site and morphology of the lesion could vary in different individuals relating to above discussed factors. So far, only few studies have been reported worldwide, including one from India. Considering its idiopathic origin and increasing cosmetic concerns, we look forward to larger studies including the histopathological findings to further enlighten our knowledge over this condition.
Acknowledgments
The authors would like to thank the patients for providing consent to use patients photographs in this article.
| 1. |
Cornbleet T. Transverse nasal stripe at puberty (Stria nasi transversa). AMA Arch Derm Syphilol 1951;63:70-2.
[Google Scholar]
|
| 2. |
Shelly WB, Shelly ED, Pansky B. The transverse nasal line: An embryonic fault line. Br J Dermatol 1997;137:963-5.
[Google Scholar]
|
| 3. |
Anderson PC. Familial transverse nasal groove. Arch Dermatol 1961;84:316-7.
[Google Scholar]
|
| 4. |
Pavithran K. A survey of transverse nasal groove. Indian J Dermatol Venereol Leprol 1989;55:105- 7.
[Google Scholar]
|
| 5. |
White SJ. Transverse nasal stripe. Arch Dermatol 1951;64:791.
[Google Scholar]
|
| 6. |
Wimmershoff MB, Hohenleutner U, Landthaler M. Transverse nasal groove. A rare embryological error in nature. Hautarzt 2001;52:828-30.
[Google Scholar]
|
| 7. |
Bowen R, Balyeat RM. Facial and dental abnormalities due to perennial nasal allergy in childhood. South Med J 1934;27:933- 8.
[Google Scholar]
|
Fulltext Views
6,575
PDF downloads
2,385





![[Table - 1]](#tbl_ijdvl_2012_78_4_439_98073_b1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2012_78_4_439_98073_u4.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_4_439_98073_u5.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_4_439_98073_u6.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2012_78_4_439_98073_u7.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2012_78_4_439_98073_b2.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2012_78_4_439_98073_u8.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2012_78_4_439_98073_b3.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2012_78_4_439_98073_u9.jpg){kind=link}