Translate this page into:
Tuberous sclerosis in a patient with situs inversus totalis and polysplenia
2 Department of Gastroenterology, Veterans Administration Hospital (NIMTS), Athens, Greece
Correspondence Address:
Efstathios Rallis
11 Pafsaniou Street, Athens 11635
Greece
| How to cite this article: Rallis E, Giannopoulos C, Korfitis C, Kyriakos N, Liatsos C. Tuberous sclerosis in a patient with situs inversus totalis and polysplenia. Indian J Dermatol Venereol Leprol 2012;78:520 |
Sir,
Tuberous sclerosis complex (TSC) is a rare multisystem disorder, exhibiting a wide range of manifestations including the skin and resulting in the formation of hamartomas. Situs inversus (also called situs oppositus or transversus) is a rare congenital condition in which a complete, mirror-image, reversal of the thoracic and abdominal organs is seen. Polysplenia is a congenital anomaly manifesting with many smaller spleens instead of an anatomically intact one. We present a very rare case of tuberous sclerosis manifesting with situs inversus totalis and polysplenia.
A 19-year-old male patient was referred to our clinic with a well-known tuberous sclerosis since childhood. According to his history, no previous laboratory or imaging testing for the disease had been performed. His medical history included only slight dyslexia since the age of 6. No alcohol, smoking or any drug intake was reported, and no family history of situs inversus, tuberous sclerosis or other disease was mentioned.
Physical examination of the skin revealed facial angiofibromas [Figure - 1], hypomelanic macules on his arms and legs (confetti-like lesions, [Figure - 2]), hypomelanic macules on his back body (ash-leaf spots, [Figure - 3]), poliosis and 2 plaques (shagreen patches, [Figure - 3]) on the left lower back and on the gluteal region. Blood tests that were performed during his hospitalization were within normal ranges.
 |
| Figure 1: Facial angiofibromas |
 |
| Figure 2: Confetti-like lesions on the left arm of the patient |
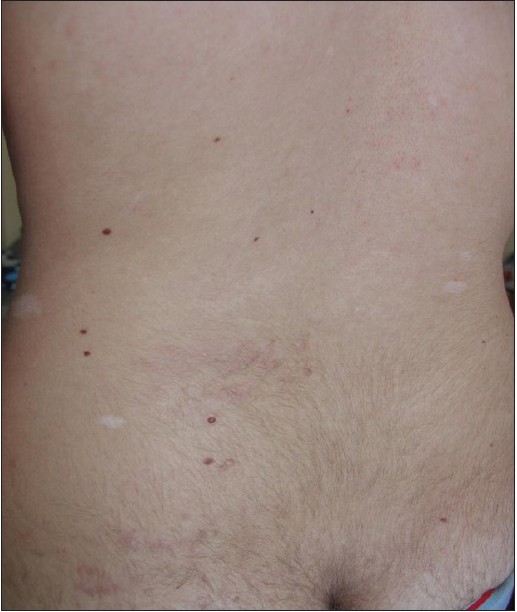 |
| Figure 3: Ash-leaf spots and shagreen patch of the back of the patient. |
Abdominal ultrasound and computed tomography (CT)-scan revealed right turn of the stomach and the liver. The gallbladder was on the left side, and polysplenia was seen on the right side [Figure - 4]. Magnetic resonance imaging and CT-scan of the brain showed subependymal nodules (multiple hamartomas), normal ventricles and no findings of malignant manifestations. High resolution CT-scan of the thorax revealed dextrocardia [Figure - 5], heart of a normal size, left turn of the aortic arch, trilobed left lung and bilobed right lung.
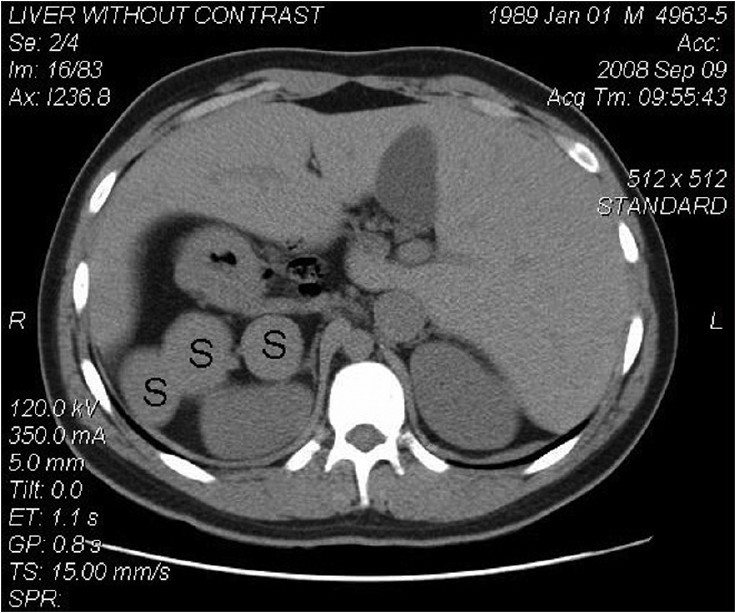 |
| Figure 4: Abdominal CT-scan: polysplenia with liver on the left side and spleens on the right side (S-spleen). |
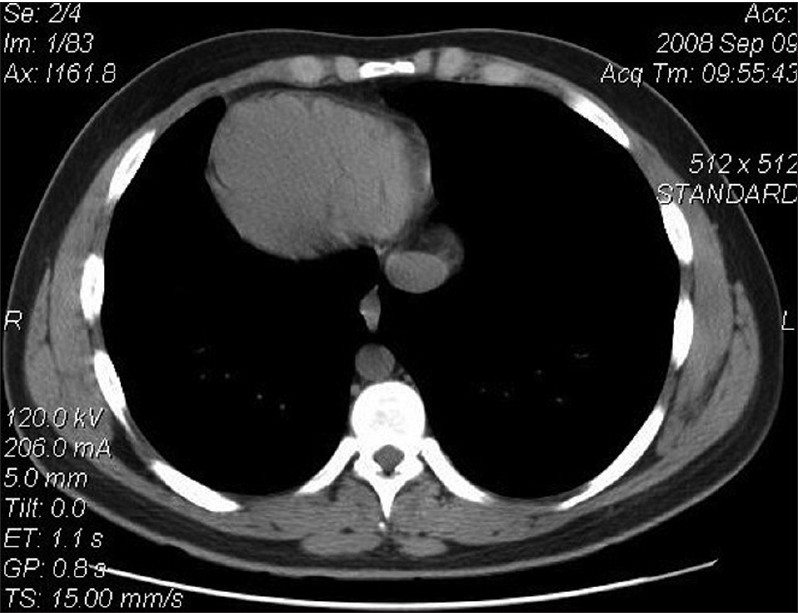 |
| Figure 5: Thoracic CT-scan: dextrocardia with normal size. |
The diagnosis of complete situs inversus with tuberous sclerosis and polysplenia was made. The patient underwent ophthalmic examination and no retinal lesions, coloboma, angiofibromas of the eyelids or papilledema were found. Neurological examination for sensory and motor function was normal. Psychiatric evaluation was performed, and no cognitive impairment or mental retardation was detected.
No cosmetic or other treatment was required. During a close clinical and laboratory 6-month follow-up, the patient remained clinically well.
TSC has been genetically determined with an autosomal dominant inheritance. It is caused by inactivating mutations in either the tuberous sclerosis 1 (TSC1) or in TSC2 genes. [1] The TSC1 and TSC2 genes provide instructions for producing proteins called hamartin and tuberin, respectively. These 2 proteins are considered responsible for the control of cell growth and size.
Situs inversus is presented worldwide with no racial predilection. The male to female incidence is 1:1. [2] If the heart is seen in the right side of the thorax, this condition is called as situs inversus with dextrocardia or situs inversus totalis. If the heart remains on the normal left side of the thorax, this condition is known as situs inversus with levocardia or situs inversus incompletus. Situs inversus totalis can be associated with primary ciliary dyskinesia, known as Kartagener syndrome. [3]
Both tuberous sclerosis and situs inversus represent 2 rare conditions occurring in humans. Various studies have estimated the incidence of tuberous sclerosis between 1 in 5,800 to 27,000. [4] Furthermore, the prevalence of situs inversus varies among different populations, but is less than 1 in 10,000 people. [2] Situs inversus incompletus is considered a much rarer condition (1 in 22,000 of the general population). Hence, the co-existence of tuberous sclerosis and situs inversus has been very rarely reported [5],[6] in the literature.
Concomitant polysplenia has been reported in situs inversus complex with variations extending from asplenia- the total absence of splenic tissue- to polysplenia. [2] The majority of cases with polysplenia are sporadic although some have been referred with an autosomal recessive inheritance.
Due to the limited number of cases, it is not currently known whether there is an underlying genetic cause for the co-existence of these 3 conditions in our patient, or it constitutes a coincidence.
| 1. |
Napolioni V, Curatolo P. Genetics and molecular biology of tuberous sclerosis complex. Curr Genomics 2008;9:475-7.
[Google Scholar]
|
| 2. |
Wilhelm A, Holbert JM. Situs inversus imaging. Available from: http://emedicine.medscape.com. [Last accessed 2012 Mar 18].
[Google Scholar]
|
| 3. |
Kinney TB, DeLuca SA. Kartagener's syndrome. Am Fam Physician 1991;44:133-4.
[Google Scholar]
|
| 4. |
Irvine AD, Mellerio JE. Genetics and genodermatoses. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's textbook of Dermatology. 8 th ed. Oxford, UK: Wiley-Blackwell; 2010. p. 15.1-15.97.
th ed. Oxford, UK: Wiley-Blackwell; 2010. p. 15.1-15.97.'>[Google Scholar]
|
| 5. |
Sarenilas L. Tuberous sclerosis with situs inversus. J Ment Defic Res 1968;12:108-10.
[Google Scholar]
|
| 6. |
Neumann HP, Brüggen V, Berger DP, Herbst E, Blum U, Morgenroth A, et al. Tuberous sclerosis complex with end-stage renal failure. Nephrol Dial Transplant 1995;10:349-53.
[Google Scholar]
|
Fulltext Views
2,865
PDF downloads
2,752





![[Figure - 1]](#fig_ijdvl_2012_78_4_520_98099_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_4_520_98099_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_4_520_98099_u3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2012_78_4_520_98099_u4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2012_78_4_520_98099_u5.jpg){kind=link}