Translate this page into:
Reactive perforating collagenosis with a giant lesion at the site of healed herpes zoster
Correspondence Address:
Ashok Krishnarao Ghorpade
BK D-18, Sector 9, Bhilai, Chhattisgarh-490 006
India
| How to cite this article: Ghorpade AK. Reactive perforating collagenosis with a giant lesion at the site of healed herpes zoster. Indian J Dermatol Venereol Leprol 2011;77:202-203 |
Sir,
A 63-year-old male presented with asymptomatic skin lesions at the site of healed herpes zoster on left side of chest and back for the previous 3 weeks. He had been treated 2 months earlier for herpes zoster at the same site with oral acyclovir tablets, topical acyclovir cream, and tablet diclofenac sodium 50 mg twice daily. The lesions healed in 2 weeks with residual pigmentation, scarring, and mild post-herpetic neuralgia.
Cutaneous examination showed multiple grouped and discrete, keratotic, mildly scaly papular lesions 2--5 mm diameter, on left side of chest and back [[Figure - 1]a] and a giant, fish-shaped, raised plaque with adherent brownish leathery crust at the raised edges and surrounding hyper pigmentation, about 80 mm Χ 60 mm in size [[Figure - 1]b] with scars of healed herpes zoster. Routine hematology and urine examination, blood glucose estimation, urea, serum creatinine, and thyroid functions were normal. Histopathology from a papular lesion and the plaque revealed similar findings with cup-shaped epidermal invagination having parakeratotic stratum corneum and necrotic debris. The mildly acanthotic epidermis had perforating channels containing collagen fibers at several places [Figure - 2]. Masson-Trichrome stain revealed vertically oriented collagen fibers in upper dermis, ready to initiate formation of the perforating channels [Figure - 3]. After confirming the diagnosis of reactive perforating collagnosis, topical retinoic acid cream 0.025% was prescribed. The skin lesions completely subsided in 3 months without any recurrence during a 2 year follow-up.
 |
| Figure 1: (a) Keratotic and umbilicated skin lesions with a big plaque, at the site of healed herpes zoster on left side of chest. (b) Close-up of the giant, scissor shaped lesion with chamois leather like crust along with scars of herpes zoster |
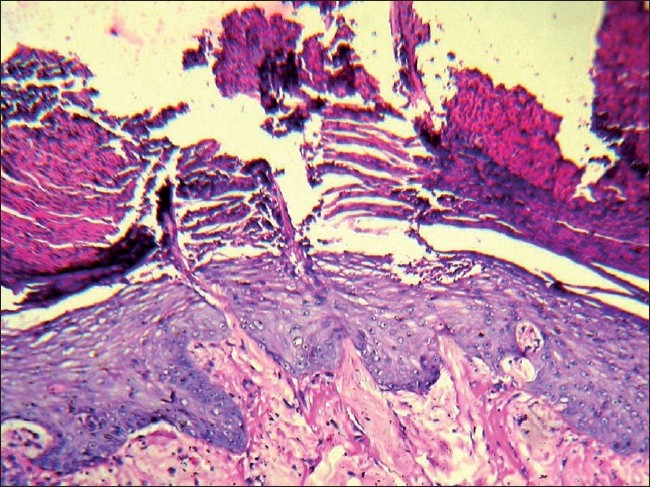 |
| Figure 2: Histopathology showing a parakeratotic plug with bluish necrotic debris and perforating channels in the epidermis (H and E, ×100) |
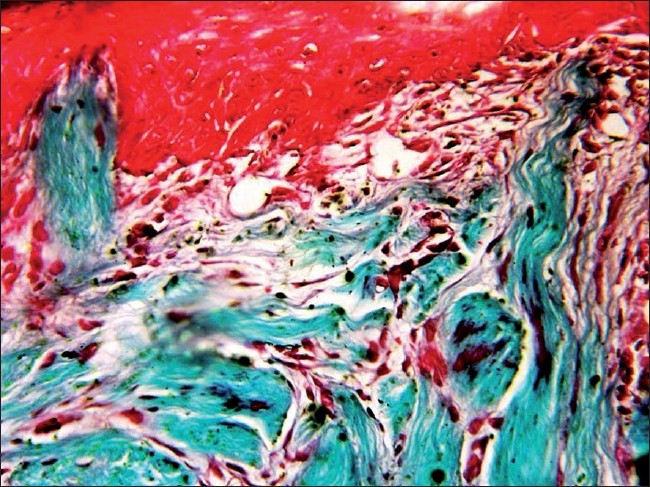 |
| Figure 3: Vertically oriented collagen fibers, perforating the epidermis from below (Masson-Trichrome stain, ×400) |
Reactive perforating collagenosis (RPC) manifesting at the site of healed herpes zoster is quite rare with only two previous reports. [1],[2] The development of a new disease at the site of healed lesions of some unrelated disease is known as "isotopic response of Wolf". Wyburn-Mason [3] were the first to report 25 cases manifesting with malignant tumors at the site of healed herpes zoster. The term "isotopic response," for such an occurrence was coined by Wolf et al. [4] It usually follows viral infections, namely herpes zoster, herpes simplex, or varicella. The subsequent conditions may be granuloma annulare, Kaposi′s sarcoma, metastasis, lymphoma, leukemia cutis, pseudolymphoma, sarcoid, tinea, angiosarcoma, Bowen′s disease, tuberculoid, and vasculitic granuloma. The less frequent conditions are acneiform eruptions, lichen sclerosus et atrophicus, solar degeneration, furunculosis, lichen planus, and reactive perforating collagenosis. [5],[6]
The time lag between the primary and the subsequent diseases is variable and could extend up to several years. Acneiform eruptions and granuloma annulare appear within a few days, whereas furunculosis, fungal infections, and pseudolymphoma manifest within 1 month of resolution of the primary condition. The initial disease should have healed completely before the onset of the subsequent disease, for labeling it as an isotopic response.
The exact reason for the occurrence of this response is not clear. Several factors including immunologic changes, namely increased sensitivity to tissue antigens in the primary viral infection or the scarring, altered microcirculation, rearrangement of collagen and an imperfect skin barrier, causing an impairment of local immunological mechanisms and the release of neuropeptides from the damaged cutaneous nerves, probably make the area a " locus minoris resistentiae."
RPC occurs in genetically predisposed individuals, in whom a mild superficial trauma like scratches, insect bites, or abrasions causes necrobiosis of collagen in the papillary dermis, which is extruded through channels in the epidermis. The lesions are asymptomatic, hyperpigmented, umbilicated, keratotic papules about 6 mm diameter, mostly seen on traumatic sites and spontaneously heal in 6-8 weeks time, with hypopigmentation or a slight scar. In acquired reactive perforating collagenosis, the skin lesions are similar to RPC, but are found in long standing diabetes mellitus, renal disease, hypothyroidism, liver disease, neurodermatitis, and hyperparathyroidism. [7]
Giant RPC manifesting as an isotopic response after herpes zoster is very unusual. A report of giant acquired RPC had the biggest lesions of around 1--2 cm. [8] The present case had a giant lesion measuring about 8 cm Χ 6 cm, in addition to the classical lesions. It was differentiated from porokeratosis of Mibelli by the absence of a raised, ridge-like border with a thin furrow in the center of the ridge, and histopathology. Detailed studies of more patients with "Wolf′s isotopic response" may help in understanding its exact pathomechanism, the reason for localization and causation of some diseases and for the supposed relation if any, between herpes zoster and malignancies, granulomatous disorders, and infections. [5],[6] Awareness about this condition, which might be under-reported, could help in detecting it more often than at present.
| 1. |
Bang SW, Kim YK, Whang KU. Acquired reactive perforating collagenosis: Unilateral umbilicated papules along the lesions of herpes zoster. J Am Acad Dermatol 1997;36:778-9.
[Google Scholar]
|
| 2. |
Lee HN, Lee DW, Lee JY, Cho BK. Two cases of reactive perforating collagenosis arising at the site of healed herpes zoster. Int J Dermatol 2001;40:191-2.
[Google Scholar]
|
| 3. |
Wyburn-Mason R. Malignant change arising in tissues affected by herpes. Br Med J 1955;2:1106-9.
[Google Scholar]
|
| 4. |
Wolf R, Brenner S, Ruocco V, Filioli FG. Isotopic response. Int J Dermatol 1995;34:341-8.
[Google Scholar]
|
| 5. |
Ghorpade A. Wolf's isotopic response- lichen planus at the site of healed herpes zoster in an Indian woman. Int J Dermatol 2010;49:234-5.
[Google Scholar]
|
| 6. |
Ghorpade A. Wolf's isotopic response: Furuncles at the site of healed herpes zoster in an Indian male. Int J Dermatol 2010;49:105-7.
[Google Scholar]
|
| 7. |
Ghorpade A, Ramanan C. Clinico-pathologic challenge: Umbilicated keratotic papules in an Indian child. Int J Dermatol 2010;49:382-4.
[Google Scholar]
|
| 8. |
Hoque SR, Ameen M, Holden CA. Acquired reactive perforating collagenosis: four patients with a giant variant treated with allopurinol. Br J Dermatol 2006;154:759-62.
[Google Scholar]
|
Fulltext Views
2,201
PDF downloads
1,180





![[Figure - 1]](#fig_ijdvl_2011_77_2_202_77468_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_2_202_77468_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_2_202_77468_u3.jpg){kind=link}