Translate this page into:
Lupus erythematosus tumidus
2 Department of Pathology, Government Medical College, Calicut, Kerala, India
Correspondence Address:
Jaheersha Pakran
19/89 Nellicode housing colony, Kavu stop, Chevayur P.O.,Calicut - 673 016, Kerala
India
| How to cite this article: Pakran J, George M, Rajan U, Lekha T, Muhammed K. Lupus erythematosus tumidus. Indian J Dermatol Venereol Leprol 2011;77:253 |
Sir,
Lupus erythematosus tumidus (LET) is a variant of cutaneous lupus erythematosus (CLE). We report a case of LET, which presented with fever, myalgia, and skin lesions showing "illusion of vesicles" mimicking Sweet′s syndrome.
A 43-year-old housewife presented with 6 year history of recurrent episodes of red raised skin lesions over sun-exposed areas. She was not on medications prior to the onset of skin lesions. Her local physician was treating her as recurrent Sweet′s syndrome with intermittent courses of systemic steroids and each time the lesions healed without leaving any post-inflammatory changes with remissions lasting between 2 and 12 months. She was referred to us for the present episode of extensive skin lesions associated with low-grade fever and myalgia of 1 week duration. Examination showed erythematous edematous plaques, some annular, of size 1--5 cm, distributed over the face, V area of neck and upper back [Figure - 1], and erythematous edematous plaques with areas showing illusion of vesicles over both forearms [Figure - 2]. Hemogram showed a total leukocyte count of 8200 with a differential count of 60% neutrophils and 38% lymphocytes. The erythrocyte sedimentation rate was 50. Other biochemical tests including the ANA profile were normal. A skin biopsy from both lesions showed upper dermal edema, dense peri-vascular and peri-appendageal lymphocytic infiltrate, and nuclear dust [Figure - 3]. Epidermis showed scanty areas of vacuolar basal cell degeneration. Colloidal iron stain demonstrated increased mucin deposition in the dermis, which was more pronounced in the skin lesion from the forearm. Direct immunofluorescence (DIF) from the skin lesion was negative. She did not meet the ARA criteria for systemic lupus erythematosus (SLE) after thorough investigation. A diagnosis of LET was made according to the criteria put forward by Kuhn et al. [1] Remission was induced with systemic steroids and maintained with hydroxychloroquine and topical sunscreens. She was asymptomatic on 5 months follow-up.
 |
| Figure 1: Erythematous edematous plaques, some annular, distributed over the face, ears and V area of the neck |
 |
| Figure 2: Erythematous edematous plaques with areas showing illusion of vesicles (arrows) over the right forearm |
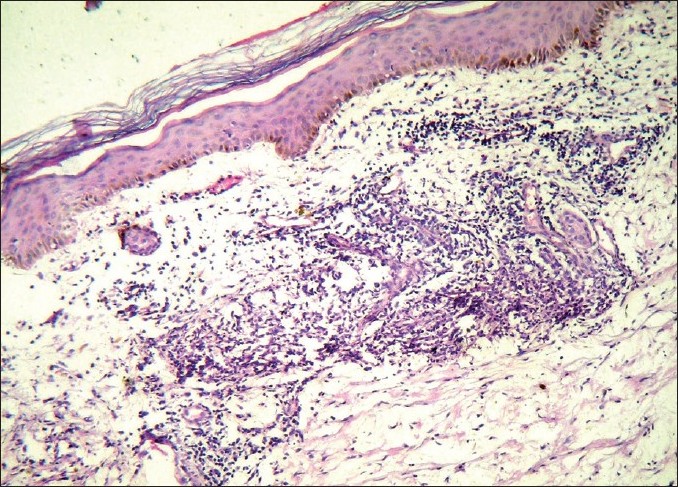 |
| Figure 3: Skin biopsy shows normal epidermis except for scanty areas of vacuolar basal cell degeneration; upper dermal edema and peri-vascular and peri-appendageal lymphocytic infiltration in the dermis (H and E, ×100) |
In Gilliam′s classification, LET is included as a subset of chronic CLE. But in recent years Kuhn et al, have contributed profoundly toward delineating LET as a distinct subset of cutaneous LE. They put forward diagnostic criteria for LET [1] as well as "The Dusseldorf classification of cutaneous LE" [2] that included a new group of LE-specific skin lesions called "intermittent cutaneous LE" (ICLE) under which comes the subset of LET.
The exact prevalence of LET is unknown. Sex incidence seems to be almost equal. Mean age of onset is in the fourth or fifth decade. History of photosensitivity is often present. [3] Clinically LET is characterized by indurated succulent urticaria like single or multiple plaques with a bright red or violaceous color and smooth surface on sun-exposed areas. Individual lesions can disappear spontaneously within days or weeks without scarring even if the disease recurs chronically sometimes for several years.
There are reports of association of LET with SLE and DLE. [3] So it is advisable to do baseline workup for systemic involvement in LET patients. We speculate that the association of fever and myalgia with onset of skin lesions in our patient signifies a progression toward SLE.
Histologically, LET lesions show peri-vascular and peri-adnexal cellular infiltrates in the papillary, and reticular dermis composed mostly of lymphocytes along with upper dermal edema and interstitial mucin deposition, which can be confirmed by alcian blue or colloidal iron staining. [3] In contrast to DLE and SCLE lesions, epidermal atrophy or alteration at the dermo-epidermal junction are either absent or only present as scattered and focally restricted parts of vacuolar degeneration at DEJ. DIF and ANA are less frequently positive in LET patients compared to DLE and SCLE. Provocative photo-testing can induce lesions of LET in more than 70% of patients. [1]
Illusions of vesicles, though originally described for Sweet′s syndrome, implies only upper dermal edema. [4] In our case the upper dermal edema was prominent enough to cause illusion of vesicles on the surface of the lesions accounting for the previous erroneous diagnosis of Sweet′s syndrome by her local physician. Colloidal iron stain can help to differentiate LET from other differential diagnosis like PLE and Jessner′s lymphocytic infiltration of skin, where there is no mucin deposition. [5]
Photo-protective measures and antimalarials can effectively control LET. Other treatment options include topical and systemic corticosteroids, topical tacrolimus, and methotrexate. [3]
| 1. |
Kuhn A, Richter-Hintz D, Oslislo C, Ruzicka T, Megahed M, Lehmann P. Lupus erythematosus tumidus - a neglected subset of cutaneous lupus erythematosus: Report of 40 cases. Arch Dermatol 2000;136:1033-41.
[Google Scholar]
|
| 2. |
Kuhn A, Ruzicka T. Classification of cutaneous lupus erythematosus. In: Kuhn A, Lehmann P, Ruzicka T, editors. Cutaneous lupus erythematosus. Berlin: Springer; 2005. p. 53-7.
[Google Scholar]
|
| 3. |
Kuhn A, Bein D, Bonsmann G. The 100 th anniversary of lupus erythematosus tumidus. Autoimmun Rev 2009;8:441-8.
[Google Scholar]
|
| 4. |
Cohen PR, Honigsmann H, Kurzrock R. Acute febrile neutrophilic dermatosis (Sweet syndrome). In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick's Dermatology in General Medicine. 7th ed. New York: McGraw-Hill; 2008. p. 289-95.
[Google Scholar]
|
| 5. |
Weyers W, Bonczkowitz M, Weyers I. LE or not LE-that is the question: An unsuccessful attempt to separate lymphocytic infiltration from the spectrum of discoid lupus erythematosus. Am J Dermatopathol 1998;20:225-32.
[Google Scholar]
|
Fulltext Views
4,387
PDF downloads
3,374





![[Figure - 1]](#fig_ijdvl_2011_77_2_253_77492_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_2_253_77492_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_2_253_77492_f3.jpg){kind=link}