Translate this page into:
A myriad of paraneoplastic dermatoses
Correspondence Address:
K Sobhanakumari
Department of Dermatology, Medical College, Kottayam, Kerala-686 008
India
| How to cite this article: Varghese SA, Sobhanakumari K, Issac CM, Seena P. A myriad of paraneoplastic dermatoses. Indian J Dermatol Venereol Leprol 2011;77:626 |
Sir,
Paraneoplastic dermatoses, describes those benign disorders in which there is a direct and often parallel course of the dermatosis with an underlying malignancy. Their presence serves as an important marker of a potentially-associated neoplastic process. We are reporting a case with multiple cutaneous paraneoplastic manifestations seen in association with an upper gastrointestinal (GI) malignancy.
A 76-year-old man presented with generalized, pruritic, hyperpigmented raised lesions for 4 years and hyperpigmentation over the sides of neck, axilla, and thighs for 4 years.
On examination, patient appeared emaciated; pallor was present and there was no significant lymphadenopathy or systemic findings. He had hyperpigmented velvety plaques over neck, axilla, groin, areola, and lips suggestive of acanthosis nigricans (AN); numerous verrucous papules and plaques with a stuck-on appearance over trunk, face, scalp, and proximal extremities suggestive of seborrheic keratosis [Figure - 1]; palms showed hyperkeratosis and altered dermatoglyphics suggestive of tripe palms and verrucous papules typifying verruca vulgaris seen over extensor surfaces of extremities [Figure - 2].
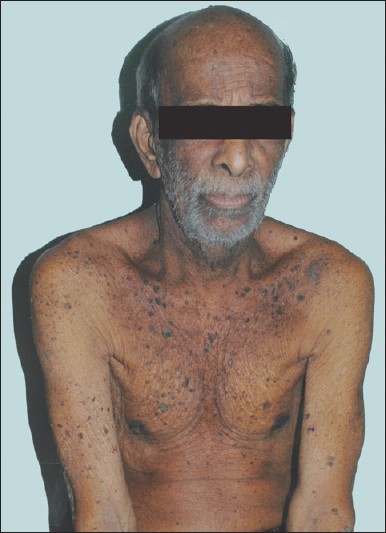 |
| Figure 1: Verrucous plaques with stuck-on appearance on the trunk, velvety hyperpigmentation over neck, flexures, and areola |
 |
| Figure 2: Tripe palms and florid cutaneous papillomatosis |
On detailed enquiry, patient revealed that he was a chronic smoker for the past 40 years. He also had difficulty in swallowing solid foods since 6 months, and had loss of weight and appetite since 3 months.
On investigation, hemogram showed an hemoglobin of 7.8 g/dl with raised erythrocyte sedimentation rate, urine routine examination was normal and stool occult blood was negative. Liver function tests, renal function tests, peripheral smear, and chest X-ray were within normal limits. Biopsies were taken from the palms, stuck-on lesions of back and verrucous plaques and were consistent with the diagnosis of tripe palms, seborrheic keratosis and florid cutaneous papillomatosis, respectively. As part of the work up for internal neoplasia, Ultrasound abdomen showed minimal wall thickening in the cardio-esophageal junction with an upper para-aortic node. Computerized tomography of abdomen and thorax showed a growth at the distal esophagus extending to the proximal stomach and enlarged para-aortic nodes. Trachea, bronchi, and lung parenchyma were normal. Oesophago-gastro-duodenoscopy showed a growth at the lower end of esophagus obstructing further passage of scope into stomach. Biopsy from the growth revealed a squamous cell carcinoma of the lower end of esophagus of poorly differentiated type. Owing to the advanced stage of the disease, our patient could only be offered palliative treatment.
The four paraneoplastic dermatoses described in our patient, ie, acanthosis nigricans, tripe palms, leser trelat sign, and florid cutaneous papillomatosis belong to a common spectrum of proliferative paraneoplastic disorders and should be viewed as part of a continuum. These conditions develop by means of a common pathogenic pathway due to an underlying malignancy that produces a factor similar to human epidermal growth factor. [1] One hypothesis suggests that the secretion of large amounts of transforming growth factor α(TGF-α) by the tumor into the circulation stimulates keratinocyte growth via an endocrine route. TGF-α is closely related to epidermal growth factor (EGF) and binds to the same receptor, EGFR. This binding induces activation of the classical mitogen-activated protein kinase (MAPK, ERK) pathway, a module of three protein kinases that is organized in a hierarchical fashion and is known to regulate basic cellular functions such as proliferation, differentiation, and migration. [2] Another hypothesis states that germline mutations in fibroblast growth factor, FGFR3 also induce a proliferative effect on keratinocytes. Strong expression of FGFR3 was frequently observed in seborrhoeic keratoses and acanthosis nigricans by immunohistochemical analysis, and that activation of FGFR3 might be a common feature in tumorigenesis in seborrhoeic keratoses and malignant acanthosis nigricans. FGFR3 might also contribute to ras/MAPK signaling in the lesions, because EGFR and FGFR3 are both transmembrane tyrosine kinase receptors (TKRs) and located upstream of the ras0 /MAPK pathway. [3] Further investigations are needed to elucidate how EGFR and FGFR3 cooperate in the pathogenesis of these cutaneous proliferative disorders.
There have been reports suggesting coexistence of acanthosis nigricans and the sign of Leser-Trιlat and florid cutaneous papillomatosis in patients with gastric adenocarcinoma [4],[5] which is the commonly associated malignancy but in our case the associated primary is a squamous cell carcinoma of the esophagus which is unusual.
| 1. |
Gheeraert P, Goens J, Schwartz RA, Lambert WC, Schroeder F, Debusscher L. Florid cutaneous papillomatosis, malignant acanthosis nigricans, and pulmonary squamous cell carcinoma. Int J Dermatol 1991;30:193-7.
[Google Scholar]
|
| 2. |
Haase I, Hunzelmann N. Activation of epidermal growth factor receptor/ERK signaling correlates with suppressed differentiation in malignant acanthosis nigricans. J Invest Dermatol 2002;118:891-3.
[Google Scholar]
|
| 3. |
Hida Y, Kubo Y, Nishio Y, Murakami S, Fukumoto D, Sayama K, et al. Malignant acanthosis nigricans with enhanced expression of fibroblast growth factor receptor 3. Acta Derm Venereol 2009;89:435-7.
[Google Scholar]
|
| 4. |
Singhi MK, Gupta LK, Bansal M, Jain V, Kachhawa D. Florid cutaneous papillomatosis with adenocarcinoma of stomach in a 35 year old male. Indian J Dermatol Venereol Leprol 2005;71:195-6.
[Google Scholar]
|
| 5. |
Yeh JS, Munn SE, Plunkett TA, Harper PG, Hopster DJ, du Vivier AW. Coexistence of acanthosis nigricans and the sign of Leser-Trelat in a patient with gastric adenocarcinoma: A case report and literature review. J Am Acad Dermatol 2000;42:357-62.
[Google Scholar]
|
Fulltext Views
2,490
PDF downloads
1,855





![[Figure - 1]](#fig_ijdvl_2011_77_5_626_84081_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_5_626_84081_f2.jpg){kind=link}