Translate this page into:
Comparative efficacy of narrow-band ultraviolet B phototherapy alone and its combination with topical 8-methoxypsoralen in psoriasis
Correspondence Address:
V K Jain
16/6J, Medical Campus, Rohtak - 124001, Haryana
India
| How to cite this article: Jain V K, Jangra S, Aggarwal K. Comparative efficacy of narrow-band ultraviolet B phototherapy alone and its combination with topical 8-methoxypsoralen in psoriasis. Indian J Dermatol Venereol Leprol 2010;76:666-670 |
Abstract
Background: Very few studies using the combination of topical 8-methoxypsoralen (8-MOP) and narrow-band ultraviolet B (NBUVB) have been performed, especially in Indian patients. A combination of oral psoralen with NBUVB has been shown to have a superior efficacy as compared with NBUVB alone in psoriasis. Aims: Comparison of the efficacy of topical psoralen NBUVB (combination) versus NBUVB alone in psoriasis. Methods: Thirty patients with plaque psoriasis were taken up for the study and NBUVB phototherapy was given twice weekly. The target lesions on one side were treated with 0.1% topical 8-MOP 15 min before the irradiation. The treatment period was 12 weeks or 24 exposures. Results: The number of treatment sessions and cumulative NBUVB doses were lower in the combination therapy as compared with NBUVB monotherapy, although the differences were not statistically significant. Conclusion: To conclude, topical 8-MOP enhances the therapeutic effects of NBUVB therapy without increasing the incidence of adverse effects.Introduction
Psoriasis is a common, chronic, disfiguring, inflammatory and proliferative condition of the skin in which both genetic and environmental influences have a critical role. [1] Its prevalence in different populations varies from 0.1% to 11.8% according to published reports. [2] Psoriasis may occur at any age, but it is uncommon under the age of 10 years and is most likely to appear between the ages of 15 and 30 years. [3] Various treatment modalities include topical agents, phototherapy and systemic agents. Several studies have shown that topical 8-methoxypsoralen (8-MOP) and ultraviolet A (UVA;PUVA) is a relatively effective modality for different types of psoriasis. [4] The combination of psoralens with narrow-band ultraviolet B (NBUVB) is less well established than with UVA. [5] In view of the paucity of studies using such a combination, especially in the Indian population, this study has been undertaken.
Methods
Thirty adult patients of chronic plaque psoriasis from our department were recruited for this prospective study from August 2008 to August 2009. The study was ethically justified by the Post Graduate Board of Medicine and Allied Sciences, Pt. B. D. Sharma, Post Graduate Institute of Medical Sciences. Patients with stable plaque psoriasis not exceeding 50% of body surface area involvement were included in this study and no blinding was performed.
Exclusion criteria included patients <16 years of age, pregnant females or lactating mothers, those with renal or hepatic disease, photosensitivity or polymorphic light eruptions. Patients already treated with oral retinoids, systemic therapy/PUVA within the previous 8 weeks, topical therapy/UVB phototherapy within the past 4 weeks or taking immunosuppressive agents were also excluded.
Detailed history regarding the age of onset, family history and history of initiating or precipitating factors was recorded. Physical examination and detailed dermatological examination including target plaque scoring, were performed and also presence of any other dermatological condition was noted. Relevant hematological and biochemical investigations such as complete blood counts, blood urea, sugar, serum aspartate transaminase/serum alanine transaminase and electrolytes were carried out in all patients. A chest X-ray was also performed at baseline to rule out any lung pathology.
UV therapy unit for NBUVB phototherapy had 16 tube lights of 100 W each (Philips TL-01) with a peak wavelength of 312 nm and 8-MOP 0.1% solution were the materials used.
Treatment protocol
Target plaque scoring
In this assessment method, two plaques of psoriasis of approximately the same size were selected from similar sites on the left and right sides of the body.
Morphological scoring of psoriatic plaques was carried out by evaluation of three parameters, i.e. erythema, scaling and thickness, each of which were graded on a severity scale of 0-4, where:
0 = nil
1 = mild
2 = moderate
3 = severe
4 = very severe
The sum of scores for each parameter gave the target plaque score. The target plaque score had a potential range of 0-12. [6]
Treatment schedule
Treatment was started after obtaining written informed consent. 8-MOP solution was applied to the target plaque on the right side 15 min prior to irradiation. NBUVB phototherapy was administered twice a week for 3 months. An initial NBUVB dose of 280 mJ/cm 2 was started. The irradiation dose was increased by 20% of the previous dose on each subsequent visit. In case of mild erythema, the irradiation dose was held constant for subsequent treatments or until resolution of symptoms. If symptomatic erythema (burning, pain or blistering) developed, the irradiation dose was decreased by 50% of the burning dose and, thereafter, the dose was increased by 10% on subsequent visits. [7] During each treatment, the affected parts were exposed, the eyes were protected by UV blocking goggles and the genitalia were shielded. All the patients were examined by the same dermatologist at each visit for up to 3 months. Target plaque scoring was carried out again at 4, 8 and 12 weeks of therapy separately for both the target plaques. After the side that achieved 95% reduction of the scores first, it was occluded and NBUVB was continued on the other side till 95% reduction or 12 weeks of completion for that side. Lesional photograph was performed at baseline and thereafter at monthly intervals.
Grades of erythema and any adverse effects like perilesional irritation, perilesional tenderness, lesional irritation, burning sensation and itching were recorded at each visit.
Results
The study included 20 males and 10 females. The maximum number of patients (63%) were seen in the age group of 21-40 years. Maximum number of the patients had body surface area involvement <10%. The total duration of disease in the patients, at the time of inclusion in this study, ranged between 3 months and 35 years.
The treatment protocol was strictly followed by most of the patients as the patients were taken for the study only when the patient opted to come twice weekly for the treatment. There were slight deviations by few patients only and one patient dropped out from the study.
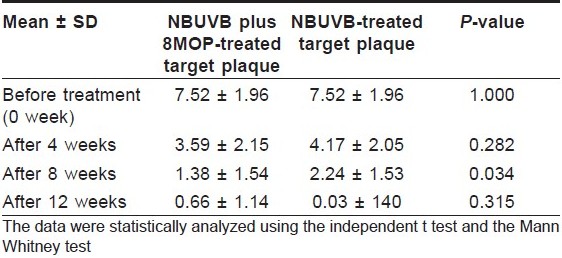
The two sides were comparable at the start of the treatment schedule and the severity scores were 7.52 ± 1.96 on the NBUVB + 8-MOP and 7.52 ± 1.96 on the NBUVB-alone sides.
The target plaque scoring at 4, 8 and 12 weeks of treatment ranged from 0 to 7 (mean 3.59 ± 2.15), 0 to 4 (mean 1.38 ± 1.54) and 0 to 4 (mean 0.66 ± 1.14) on the combination side. Target plaque scoring of the target plaques treated with NBUVB alone at 4, 8 and 12 weeks of therapy had a range of 0-7 (mean 4.17 ± 2.05), 0-5 (mean 2.24 ± 1.53) and 0-4 (mean 1.03 ± 1.40), respectively [Table - 1].
The results were compared for the two target plaques in terms of target plaque score, number of treatment sessions, number of weeks of treatment, maximum dose of NBUVB and the cumulative dose of NBUVB required for 95% reduction of scores or at 12 weeks.
The difference in the mean target plaque scores was significant only at 8 weeks of treatment and insignificant at 4 weeks and at the end of the treatment therapy (P > 0.05).
The total number of treatment sessions given on both the sides had a range of 8-24, with a mean of 17.21 ± 6.16 on the combination therapy side as compared with 19.14 ± 5.40 on the NBUVB monotherapy side (P-value 0.209), indicating that lesser number of treatment sessions were required for clearance in the NBUVB plus 8-MOP-treated group.
The mean maximum dose given on the combination side was 1415.24 ± 529.64 as compared with 1551.45 ± 510.24 on the NBUVB-alone side.
The cumulative doses required for either 95% reduction of the scores or at 24 weeks were smaller for the combination therapy group [Figure - 1] and [Figure - 2] as compared with the NBUVB monotherapy-treated group [Figure - 3] and [Figure - 4], although the differences were not statistically significant.
 |
| Figure 1 :Patient 1 – at the start of treatment |
 |
| Figure 2 :Patient 1 – at 12 weeks |
 |
| Figure 3 :Patient 2 – at the start of treatment |
 |
| Figure 4 :Patient 2 – at 12 weeks |
Although there is no significant difference between most outcome measures, the scores were lower for almost all values on the NBUVB + 8-MOP-treated side as compared with that on the NBUVB-alone side, showing that 8-MOP enhances the therapeutic effects of NBUVB.
Of 30 patients, 20 on the combination side and 17 on the NBUVB-alone side had more than 95% reduction of the scores. Five patients from the combination side and three from the NBUVB-alone side had more than 75% reduction of the scores, and the difference was not found to be statistically significant. More than 50% reduction was achieved in one and seven patients on the combination and NBUVB-alone sides respectively. Three patients on both the sides had <50% reduction of the scores. The condition worsened in one patient on the combination side and none on the NBUVB-alone side.
Side-effects
In the present study, we recorded that the side-effects were higher on the combination side as compared with NBUVB alone, but these were minor side-effects. Mild erythema was noted in almost all the patients. Itching was complained by 12 patients during the treatment sessions, which was present on almost all the lesions. Hyperpigmentation was noted in most of the patients which became darker with further application of 8-MOP on the test target plaques. The pigmentation was marked in six patients even after the solution was removed after the phototherapy session. Burning was noted after phototherapy on all the plaques in three patients. Treatment therapy was tolerated well by all the patients except one who developed marked burning, oozing, erythema and crusting on the 8MOP-treated side and discontinued the treatment after seven treatment sessions.
Discussion
Topical therapy has been, and remains, the primary therapeutic option for the treatment of limited psoriasis and NBUVB, is a safe and effective modality for attaining long-term remissions.
Psoralens are chemical compounds derived from certain plants such as Ammimajus found in Egypt and the Indian plant, babachee, which is also called as Psoralea corylifolia. [8] Psoralen and many of its derivatives are naturally occurring tricyclic furocoumarins. The derivative most widely used in photochemotherapy is 8-MOP (methoxsalen, xanthotoxin), which is principally of plant origin but is available as a synthetic drug. 4, 5, 8-trimethyl psoralen (TMP, trioxsalen) is a synthetic compound that is less phototoxic after oral administration and is primarily used for the treatment of vitiligo. Newer psoralens under research are 5-MOP (bergapten, 3-carbethoxypsoralen and angelicin). [9],[10]
The exact mechanism by which psoralens produce cutaneous photosensitivity reactions is not precisely known. The mode of action of psoralens does not occur at one level but occurs at several levels simultaneously including cellular DNA, RNA proteins, mitochondria, cell membrane lipids, etc. In the normal skin or in the skin of psoriatic patients, psoralen-induced skin photosensitization involves two distinct types of reactions occurring independently of each other and concurrently when psoralen-treated skin is exposed to 320-400 nm radiation.
- Type I is an anoxic reaction not requiring oxygen and the site of cellular damage is primarily in the DNA of cell nuclei.
- Type II is a sensitized reaction dependent on oxygen and involves the formation of oxygen reactive species such as 0 2 , 02 - and free radicals.
PUVA causes photoconjugation of psoralens to DNA and subsequent suppression in mitosis, DNA synthesis and cell proliferation. It is also possible that PUVA may affect specific cells such as lymphocytes or polymorphonuclear leucocytes that are believed to be involved in the pathophysiology of psoriasis. [11]
The combination of oral psoralens and UVA (320-400 nm) has been used for many years, and the therapeutic effect of psoralen and ultraviolet radiation of wavelength <320 nm has been studied less extensively.
It seems likely that the mechanism of action of psoralen UVB therapy is both through a direct therapeutic effect of 311 nm radiation on psoriasis as well as through psoralen-mediated photochemical responses.
de Berker et al. [12] reported the results of a randomized trial in patients with plaque-type psoriasis comparing conventional PUVA with psoralenUVB therapy in 100 patients. They concluded that psoralenUVB treatment of psoriasis is as effective as PUVA.
The combination of psoralens with NBUVB is less well established than with UVA. Sakuntabhai et al. [13] were among the first to report the use of oral 8-MOP with whole-body NBUVB (TL-01) irradiation. In a left and right comparison study, they showed that the side that received the combination cleared faster than the contralateral lesion receiving only NBUVB treatment.
A study was conducted by Seckin et al. [14] to find out whether topical psoralen NBUVB provides any additional benefit to NBUVB alone in psoriasis, wherein a target lesion on one side was treated with 1% 8-MOP gel 30 min before UVB radiation and the target lesion on the other side served as control. Target lesion scores decreased significantly on both sides. The mean percentage of decreases was greater on the 8-MOP-applied sides compared with the control sides for all assessments and the authors concluded that 8-MOP gel plus narrowband has greater efficacy than NBUVB alone in psoriasis. Asawanonda et al. [5] reported the role of topical 8-MOP cream in targeted NBUVB phototherapy, the combination of which resulted in fewer sessions and lower cumulative UVB doses to clear psoriatic lesions, and proposed that in patients who do not respond well to targeted treatment alone, topical 8-MOP should be added.
In another study by Amornpinyokeit et al., [15] addition of 0.1% 8-MOP cream was shown to enhance the therapeutic effects of targeted NBUVB significantly without increasing the incidence of side-effects. Similarly, in our study, it was observed that the combination of NBUVB with topical 8-MOP resulted in fewer sessions and lower maximum and total cumulative dosages. However, the results were not statistically significant at the end of the treatment schedule.
To conclude, the combination of topical 8-MOP with NBUVB phototherapy is an effective treatment modality in the therapeutic armamentarium for the treatment of localized psoriasis and can be added in patients who do not respond to NBUVB phototherapy. However, longer term prospective studies with larger sample size are required to delineate clearly the magnitude of the additional therapeutic effect achieved by combining topical 8-MOP and NBUVB in the treatment of psoriasis.
| 1. |
Griffiths CEM, Camp RDR, Barker JNWN. Psoriasis. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology, 7 th ed. London: Blackwell Scientific Publication; 2004. p. 351-69.
th ed. London: Blackwell Scientific Publication; 2004. p. 351-69.'>[Google Scholar]
|
| 2. |
Raychaudhuri SP, Farber EM. The prevalence of psoriasis in the world. J Eur Acad Dematol Venereol 2001;15:16-7.
[Google Scholar]
|
| 3. |
Gudjonsson JE, Elder JT. Psoriasis. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick's Dermatology in General Medicine, 7 th ed. USA: The McGraw Hill Companies; 2008. p. 169-93.
th ed. USA: The McGraw Hill Companies; 2008. p. 169-93. '>[Google Scholar]
|
| 4. |
De Rie MA, Van Eendenburg JP, Versnick AC, Stolk LM, Bos JD, Westerhof W. A new psoralen-containing gel for topical PUVA therapy: Development, and treatment results in patients with palmoplantar and plaque-type psoriasis, and hyperkeratotic eczema. Br J Dermatol 1995;132:964-9.
[Google Scholar]
|
| 5. |
Asawanonda P, Amornpinyokeit N, Nimnuan C. Topical 8-methoxypsoralen enhances the therapeutic results of targeted narrowband ultraviolet B phototherapy for plaque-type psoriasis. J Eur Acad Dermatol Venereol 2008;22:50-5.
[Google Scholar]
|
| 6. |
Das S, Lloyd JJ, Walshaw D, Diffey BL, Farr PM. Response of psoriasis to sunbed treatment: Comparison of conventional ultraviolet A lamps with new higher ultraviolet B - emitting lamps. Br J Dermatol 2002;147:966-72.
[Google Scholar]
|
| 7. |
An appraisal of narrowband (TL-01) UVB phototherapy. British Photodermatology Group Workshop Report (April 1996). Br J Dermatol 1997;137:327-30.
[Google Scholar]
|
| 8. |
Gupta AK, Anderson TF. Psoralen photochemotherapy. J Am Acad Dermatol 1987;17:703-34.
[Google Scholar]
|
| 9. |
Hφnigsmann H, Jaschke E, Gschnait F, Brenner W, Fritsch P, Wolff K. 5-Methoxypsoralen (Bergapten) in photochemotherapy of psoriasis. Br J Dermatol 1979;101:369-78.
[Google Scholar]
|
| 10. |
Dubertret L, Averbeck D, Zagdela F, Bisagni E, Moustacchi E, Touraine R, et al. Photochemotherapy (PUVA) of psoriasis using 3-carbethoxy psoralen, a non- carcinogenic compound in mice. Br J Dermatol 1979;101:379-89.
[Google Scholar]
|
| 11. |
Srinivas CR, Pai S Psoralens. Ind J Dermatol Venereol Leprol 1997;63:276-87.
[Google Scholar]
|
| 12. |
de Berker DA, Sakuntabhai A, Diffey BL, Matthews JN, Farr PM. Comparison of psoralen-UVB and psoralen-UVA photochemotherapy in the treatment of psoriasis. J Am Acad Dermatol 1997;36:577-81.
[Google Scholar]
|
| 13. |
Sakuntabhai A, Diffey BL, Farr PM. Response of psoriasis to psoralen-UVB photochemotherapy. Br J Dermatol 1993;128:296-300.
[Google Scholar]
|
| 14. |
Seckin D, Usta I, Yazici Z, Senol A. Topical 8-methoxypsoralen increases the efficacy of narrowband ultraviolet B in psoriasis. Photodermatol Photoimmunol Photomed 2009;25:237-41.
[Google Scholar]
|
| 15. |
Amornpinyokeit N, Asawanonda P. 8-Methoxypsoralen cream plus targeted narrowband ultraviolet B for psoriasis. Photodermatol Photoimmunol Photomed 2006;22:285-9.
[Google Scholar]
|
Fulltext Views
3,107
PDF downloads
2,773





![[Table - 1]](#tbl_ijdvl_2010_76_6_666_72464_t1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2010_76_6_666_72464_f2.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2010_76_6_666_72464_f3.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2010_76_6_666_72464_f4.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2010_76_6_666_72464_f5.jpg){kind=link}