Translate this page into:
SCORTEN: Does it need modification?
Correspondence Address:
S S Vaishampayan
Dermatologist, 155 Base Hospital c/o 99 APO
India
| How to cite this article: Vaishampayan S S, Das A L, Verma R. SCORTEN: Does it need modification?. Indian J Dermatol Venereol Leprol 2008;74:35-37 |
Abstract
Background: Toxic epidermal necrolysis (TEN) is a drug induced acute life threatening condition with mortality ranging from about 15 to 60%. A 'severity of illness' score termed as SCORTEN has been developed to predict mortality in TEN cases at the time of admission. It is calculated by giving one point for each of predetermined seven variables, evaluated during first 24 hours of admission. Total score ranging from 1-7 predicts a probability of mortality from 0.03 to 0.90. Aim: A prospective study was conducted to analyze efficacy of 'SCORTEN' in TEN cases to predict mortality during their management. Methods: All cases of TEN reporting for management to the hospital were assessed using 'SCORTEN' on day one and day five to predict probable mortality, this data was then compared with ultimate outcome. Results: During the study period, we treated 10 cases of TEN, all induced by drugs, patient's age ranging from 03 to 70 years and body surface area (BSA) involvement from 10 to 95%. Three cases succumbed to death. These cases were analyzed with SCORTEN to predict probability of mortality at the time of admission and day five. We encountered some variations from the original study. It was observed that if patients are analyzed with SCORTEN on a daily/alternate day basis, it will serve as a better predictor of mortality. Conclusion: Body surface area (BSA) involvement and age probably need more weightage in calculations. Besides malignancy, tuberculosis and pre-existing diabetes also need to be included while predicting mortality.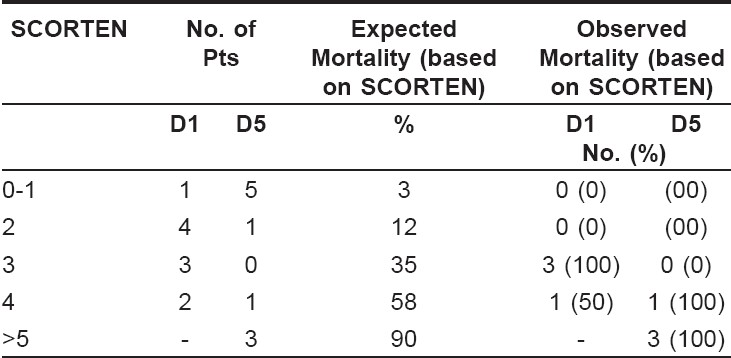
Introduction
Toxic epidermal necrolysis (TEN) is a drug related, acute life threatening dermatological disease. Apoptosis of cells causes erosion of mucous membranes, extensive detachment of epidermis and severe constitutional symptoms. Stevens-Johnson syndrome (SJS) and TEN are considered variants within a continuous spectrum, SJS or SJS-TEN overlaps being milder forms. This classification is based on percentage of denuded skin. [1]
The incidence of TEN is reported to be 0.4-2 cases per million populations per year. [2] In India exact incidence of this near fatal disease is not known and seems to be increasing due to indiscriminate use of drugs. This severe disease is reported to have a mortality rate ranging from 15 to 40% with frequent disability in survivors. Various prognostic factors already known are advancing age, maximal body surface area (BSA) detachment and increased blood urea levels. [3] Another major cause of death in TEN has been reported to be bronchial epithelial detachment.
There are several severity-of-illness scores being used in ICUs to estimate the probability of hospital mortality. Specific scores have been developed for burn patients (age plus percentage of BSA burned) since general ICU scores can not be extrapolated on them and so is the case of acute dermatoses like TEN. A score termed as SCORTEN was developed by Basutji-Gatin et al. in year 2000, as a severity-of-illness score for TEN. [4] It is a validated predictor of mortality in TEN patients when seen at the time of admission. The score is calculated by giving 01 point for each of the following 07 clinical variables during the first 24 hours of evaluation;
- Age more than 40 years
- Malignancy
- Heart rate> 120/minute
- Initial epidermal detachment> 10% of BSA
- Serum urea level> 28 mgm/dl (40 mgm/dl in Indian settings)
- Serum glucose levels> 250 mgm/dl and
- Serum bicarbonate levels < 20 mEq/dl.
The probability of death predicted by this score is as follows: 0-1 points- 0.03; 2 points- 0.12; 3 points- 0.35; 4 points- 0.58; 5 to 7 points- 0.90. A probability of 0.90 means approximate 90 of 100 patients with TEN are expected to die. SCORTEN has been used extensively in large number of studies with good to excellent accuracy in predicting death in TEN cases. Since this score is relatively new, a study was conducted to find out applicability of SCORTEN in TEN patients in Indian settings.
Methods
A prospective study was carried out at Command Hospital, Pune for 24 months. A total of 10 cases were diagnosed to have TEN/SJS-TEN out of nearly 23000 cases seen in OPD during the study period. All the cases diagnosed to have TEN, were subjected to a standard battery of ICU protocol of investigations on day one, following which each case was analyzed using SCORTEN. Same battery of tests and analysis were also carried out on day five and prediction of mortality on both days as predicted by SCORTEN was later compared with final outcome.
Results
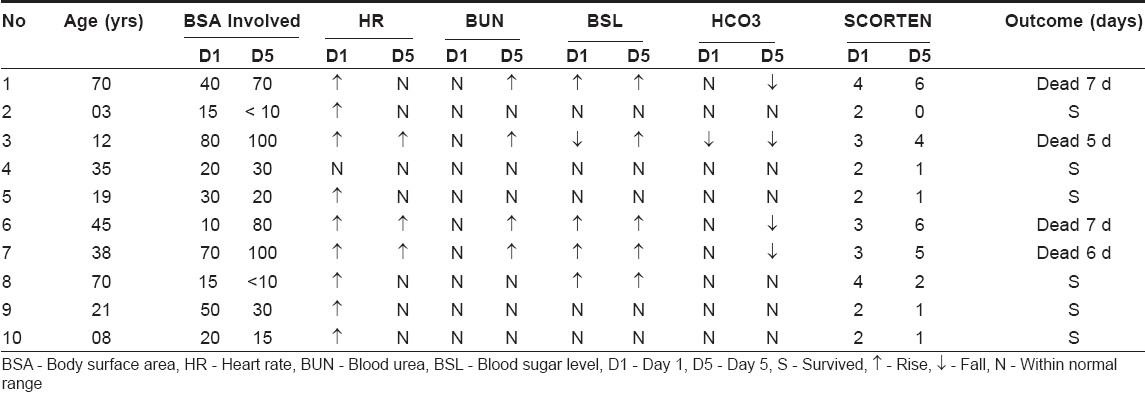
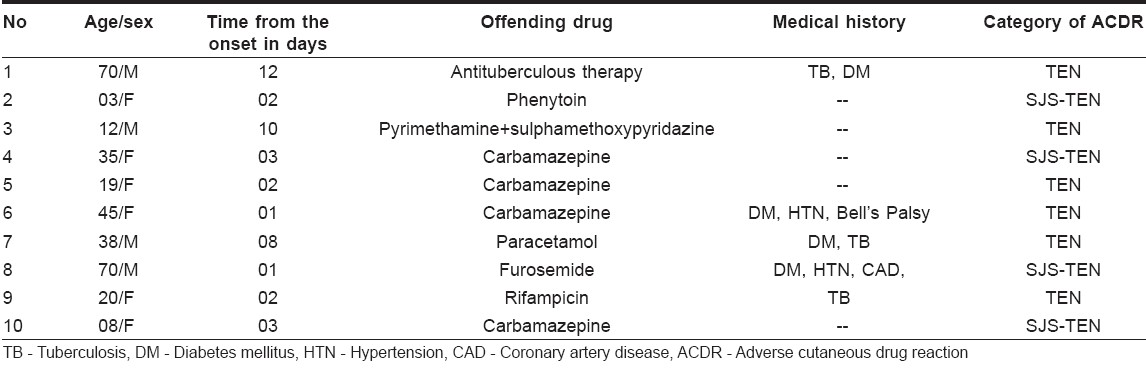
Since total number of patients was only 10 statistical analysis could not be done. We treated 10 cases of TEN with age ranging from 03 to 70 years and BSA involvement being 15 to almost 100%. Anticonvulsants were the commonest (5/10) drugs implicated, anti-tuberculous therapy being the next (2/10) common causative drug category. Paracetamol was thought to be the precipitating cause of TEN in one case. Many patients were on multiple drugs.
Females outnumbered males (6:4) as reported in some text books. Details of patient data (including SCORTEN and mortality data) are given below [Table - 1],[Table - 2]. Out of the ten patients, 5 had stopped probable offending drug themselves before reporting to us, but 2 of them died. In the remaining 5, probable offending drugs (mostly multiple) were stopped by us immediately on reporting.
Discussion
After analyzing above data it is clear that none of the patients had malignancy but 4 out of 10 had pre-existing diabetes mellitus and 03 of them died. Tuberculosis was seen in 3 patients and 2 out of 3 died. Thus in Indian sub-continent probably these systemic diseases and other severe systemic illnesses need to be given weightage equal to malignancy. Age had no effect on the ultimate mortality but more male 3/4 died as compared to females 1/6. As is well known, ultimate cause of death was septicemia in all 4 cases who died, despite best possible management in a tertiary care hospital.
In SCORTEN analysis, % of BSA involvement entails 01 point, equal to other six parameters, however it is a well known fact (as observed in this study too) that BSA involvement of> 40% had very poor prognosis. Therefore BSA involvement of> 40% should be given more weightage as in burn scores.
Analysis of data given in Table numbers 02 and 03 reveals that patient number 1, 3, 5 and 6 who ultimately died had SCORTEN of either 3 or 4 on day 01 (these scores have a predicted mortality of 35 to 50%) and in all of them SCORTEN increased to 5 or 6 on day 05 (at these scores prediction of mortality rate rises to more than 90%). Thus it is apparent that expected mortality based on SCORTEN of day 05 is more accurate than SCORTEN calculated on first day.
Though this study involves only 10 cases, following amendment are recommended keeping in mind the conditions prevalent in the Indian sub-continent. a) Percentage (%) of BSA involvement be given graded points e.g. 10-30% = 01 point,> 30% = 02 points. b) Besides malignancy other systemic diseases like pre-existing diabetes mellitus, tuberculosis, cardiac disorders, other severe chronic diseases should also be included while calculating SCORTEN. c) SCORTEN analysis should be done on first as well as fifth day to get more accurate picture and prognosis.
Larger and longer studies are required to further authenticate and confirm these observations so that a modified and better SCORTEN may evolve.
| 1. |
Bastuji-Garin S, Rzany B, Stern NH, Naidi L, Roujeau JC. Clinical classification of cases of toxic epidermal Necrolysis, Stevens-Johnson syndrome and erythema multiforme. Arch Dermatol 1993;129:92-6.
[Google Scholar]
|
| 2. |
Roujeau JC, Kelly JP, Naldi L, Rzany B, Stern RS, Anderson T, et al. Medication use and the risk of Stevens-Johnson syndrome and toxic epidermal Necrolysis. N Engl J Med 1995;333:1600-7.
[Google Scholar]
|
| 3. |
Revuz J, Penso D, Roujeau JC, Guillaume JC, Payne CR, Wechsler J, et al. Toxic epidermal Necrolysis: Clinical findings and prognostic factors in 87 patients. Arch Dermatol 1987;123:1160-5.
[Google Scholar]
|
| 4. |
Bastuji-Garin S, Fouchard N, Bertochi M, Roujeau JC, Revux J, Wolkenstein P. SCORTEN: A severity of illness score for toxic epidermal Necrolysis. J Invest Dermatol 2000;115:149-53.
[Google Scholar]
|
Fulltext Views
5,921
PDF downloads
2,416





![[Table - 1]](#tbl_ijdvl_2008_74_1_35_38405_1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2008_74_1_35_38405_2.jpg){kind=link}