Translate this page into:
Epidermolytic hyperkeratosis with a rare digital contracture
Correspondence Address:
Sudip Das
NRS Medical College and Hospital, Skin, STD and Leprosy Department, Room no-18 and 19, OPD Building, NRS Medical College and Hospital, Kolkata-14
India
| How to cite this article: Das S, Roy AK, Kar C, Maiti A. Epidermolytic hyperkeratosis with a rare digital contracture. Indian J Dermatol Venereol Leprol 2007;73:280 |
Abstract
A sixteen year-old male patient with no history of consanguinity in the family, reported with patchy, thickened lichenified plaques over the whole body. Some areas had normal skin while some were Blaschkoid lesions. The child had delayed milestones along with hypogonadism. Digital contracture with palmoplantar keratoderma was present. Histopathology showed characteristic vacuolar degeneration of the upper epidermis and suprabasilar keratinocytes with hyperkeratosis.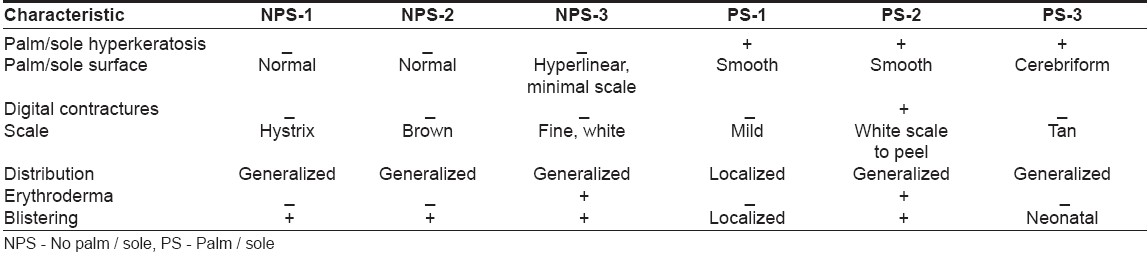
Introduction
Epidermolytic hyperkeratosis (EHK) is transmitted as an autosomal dominant trait with a prevalence of approximately 1 in 200,000 to 300,000. However, there is a high frequency of spontaneous mutation and as many as one-half of the cases have no family history and have new mutational events. [1]
Case Report
We report a 16 year-old male patient from Murshidabad with patchy hyperkeratosis all over the body and face, present since a year of age. The lichenified plaques were extensive on the knees, elbows and all flexors. There were also linear streaks of similar lichenified rugose plaques. The patient complained of generalized itching, palmoplantar keratoderma and digital contractures of both hands involving middle, ring and little fingers. Both palms and soles showed keratoderma, but there was no uniform thickening in palms and soles and a transgrediens pattern was seen. There was no history of erythroderma or collodion baby at any point of time during the evolution of the disease. The patient had reported a retarded growth and delayed developmental milestones. The size of the testis was 3 cm x 3 cm (smaller). Routine semen analysis revealed oligospermia with very sluggish motility. There was no history of any similar disease or consanguinity in the family. Histopathology revealed vacuolar degeneration of the upper epidermis and suprabasilar keratinocytes with hyperkeratosis compatible with the clinical diagnosis.
Discussion
Sporadic EHK due to postzygotic spontaneous mutation during embryogenesis can present in a mosaic pattern of skin involvement. Areas of hyperkeratosis alternating with normal skin are often distributed in streaks along Blaschko′s lines. [3] The characteristic histopathology of vacuolar degeneration of epidermis and associated hyperkeratosis are the hallmarks of the disease.
A useful differentiating characteristic feature is the presence or absence of severe palmar / plantar hyperkeratosis. Three subtypes have palm / sole involvement (PS-type), while the other three have no palm / sole involvement (NPS-type) [Table - 1].
We therefore report this case of EHK (PS-2) type with occasional linear Blaschkoid strips of hyperkeratotic lesions, possibly suggesting a sporadic mosaic mutation of hystrix pattern of EHK. Digital contracture and palmoplantar hyperkeratosis in association with EHK is reported in PS variants. Only PS-2 types have shown digital contracture, [2] as seen in our patient. Retarded growth and delayed developmental milestones are not very common in EHK. We report this case because of these atypical features.
| 1. |
Digiovanna JJ, Bale SJ. Clinical heterogeneity in epidermolytic hyperkeratosis. Arch Dermatol 1994;130:1026-9.
[Google Scholar]
|
| 2. |
Nazzaro V. Epidermolytic hyperkeratosis: Generalized form in children from parents in systematized linear form. Br J Dermatol 1990;122:417-9.
[Google Scholar]
|
| 3. |
Christophers E, Mrowietz U. Psoriasis. In : Freedberg IM, et al , editors. Fitzpatrick's dermatology in general medicine. 6 th ed. The McGraw-Hill: USA; 2003. p. 407-27.
th ed. The McGraw-Hill: USA; 2003. p. 407-27.'>[Google Scholar]
|
Fulltext Views
1,588
PDF downloads
1,298





![[Table - 1]](#tbl_ijdvl_2007_73_4_280_33652_1.jpg){kind=link}