
Translate this page into:
Carotid intima-media thickness and epicardial fat thickness predict precoronary artery disease status in psoriasis
Corresponding author: Dr. Shajahan Shibina, Porunnel Padinjattathil, Koottikada P O, Thattamala, Kollam - 691 020, Kerala, India. aizafiroz2016@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Girisha BS, Shibina S, Raghuraja U, Subramanyam K. Carotid intima-media thickness and epicardial fat thickness predict precoronary artery disease status in psoriasis. Indian J Dermatol Venereol Leprol 2021;87:357-63.
Abstract
Background:
Carotid intima-media thickness test is a surrogate marker of subclinical atherosclerosis. Epicardial fat thickness is an early marker of coronary artery disease. Several studies have noted that psoriasis patients have an increased risk of coronary artery disease. In the present study, we attempted to see any variation in carotid intima-media thickness and epicardial fat thickness in psoriasis patients when compared to controls.
Aims:
1) To determine the carotid intima-media thickness and epicardial fat thickness in psoriatic patients and healthy controls. 2) To evaluate the association between carotid intima-media thickness and epicardial fat thickness in psoriasis patients.
Methods:
A hospital-based study with 100 subjects (50 with psoriasis and 50 healthy controls) was conducted in the Dermatology Outpatient Department of Justice KS Hegde Charitable Hospital, a unit of KS Hegde Medical Academy affiliated to NITTE (Deemed to be University) Mangaluru. A detailed history and examination including body mass index, psoriasis area and severity index were done. Carotid ultrasound was done to measure carotid intima-media thickness and transthoracic echocardiography was done to assess epicardial fat thickness in both cases and controls. Independent sample t-test, Pearson rank correlation (r) coefficient were used for statistical analysis. P-value <0.05 was considered statistically significant. IBM Statistical Package for the Social Sciences version 22 Armonk, NY: IBM Corp was used for statistical analysis.
Results:
Mean carotid intima-media thickness in the right carotid ([0.51 ± 0.1mm vs 0.47 ± 0.1 mm] [P = 0.038]) and left carotid ([0.53 ± 0.12 mm vs 0.48 ± 0.1 mm] [P = 0.041]) were significantly increased in psoriasis patients than in controls. Mean epicardial fat thickness was significantly increased ([1.76 ± 0.66 mm vs. 1.49 ± 0.47 mm] ([P = 0.020]) in patients with psoriasis when compared with the controls. Epicardial fat thickness was positively correlated with carotid intima-media thickness in patients with psoriasis.
Limitations:
The cross-sectional design of the study, smoking among study subjects, inter and intraobserver variability of measurement of epicardial fat thickness and carotid intima-media thickness.
Conclusion:
Carotid intima-media thickness and epicardial fat thickness were increased in psoriasis patients when compared with healthy controls. Epicardial fat thickness was positively correlated with carotid intima-media thickness in cases.
Keywords
Atherosclerosis
psoriasis
transthoracic echocardiography

Introduction
Psoriasis is a chronic, immune or inflammatory mediated polygenic disorder with varying morphology, distribution, severity and course.1 It is increasingly being recognized as an independent risk factor for coronary artery disease. Younger age, longer duration of the disease and increased severity seem to increase the risk of of coronary artery disease in psoriasis patients.2,3 Multiple studies have reported that psoriasis is associated with traditional risk factors of coronary artery disease which includes hypertension, diabetes, obesity and dyslipidemia. This association may be due to the common inflammatory pathway shared by psoriasis and atherosclerosis including Th1-mediated inflammation, alterations in angiogenesis and endothelial dysfunction.4-6 Carotid intima-media thickness is considered as a marker of systemic inflammation. It predicts subclinical atherosclerosis and future cardiovascular disease events7,8 Epicardial fat is visceral adiposity that is situated between the heart and pericardium. It covers 80% of the heart surface and found to be increased in coronary artery disease.9 In psoriasis, the epicardial fat thickness was found to be significantly high and more prominent in severe disease.10 This is the first study from India where we have assessed the carotid intima-media thickness and epicardial fat thickness in psoriasis patients and tried to find any association between the two.
Methods
This hospital-based study was conducted from October 2016–March 2018. One hundred subjects (50 cases and 50 controls) attending the Dermatology Outpatient Department of Justice KS Hegde Charitable Hospital, a unit of KS Hegde Medical Academy affiliated to NITTE (Deemed to be University), Mangaluru were included in the study. Institutional ethics committee clearance was taken before the start of the study. All patients with age above 18 years who were consenting to participate in the study were included. Cases were defined as subjects with chronic plaque psoriasis. Controls were defined as age and sex-matched individuals without psoriasis and any clinical evidence of any other disease. Subjects attending the health check-up lounge of the hospital and attendants of patients were considered for the control group. Following exclusion criteria were used: 1) patients with erythrodermic psoriasis, pustular psoriasis, guttate psoriasis and psoriatic arthritis. 2) patients with diabetes mellitus and hypertension, cardiovascular or cerebrovascular disease, renal and liver disease. 3) subjects who were receiving lipid-lowering therapy, antihypertensive or antiplatelet aggregation drugs. 4) pregnant and lactating women. 5) a history of malignancy.
After fulfilling the selection criteria, all participants were counselled about the study and informed written consent was obtained. A detailed history was taken with emphasis on the onset, duration of the disease and a complete physical examination was done. The height and weight of the patients was measured. Waist circumference was obtained in a standardized technique using a flexible nonextendable tape by a single observer. Waist circumference was measured at the midpoint between the 12th costal lower boundary and the iliac crest. Body mass index was calculated by weight in kg divided by height in m2 and was interpreted according to the standard consensus statement for Asian Indians as follows: underweight: <18, normal body mass index: 18.0– 22.9, overweight: 23.0–24.9 and obese: >25.0.11 Site and extent of involvement of psoriatic lesions were noted. The severity of the disease was evaluated using the psoriasis area and severity index score. Psoriasis area and severity index score was graded as mild, moderate and severe with scores of <8, 8–12 and >12, respectively.12 Fasting blood sample was drawn for testing blood sugar and lipid profile.
Carotid intima-media thickness and epicardial fat thickness were measured in all the participants. Carotid intima-media thickness was measured by a trained radiologist recording ultrasonographic images of both right and left common carotid arteries with a linear transducer. The carotid intima-media thickness was measured at about 1 cm proximal to the carotid bifurcation. Measurements were obtained from four contiguous sites at 0.5 cm intervals excluding the plaque. The average of the four measurements was used for the analysis. Transthoracic echocardiography was used to measure the epicardial fat thickness and it was carried out by a trained cardiologist. Epicardial fat thickness was measured on a point over the right ventricular free wall at end-systole, perpendicular to the aortic annulus from parasternal longitudinal view for three consecutive cardiac cycles. The average of three cardiac cycles from each echocardiographic view was determined as epicardial fat thickness.13 Metabolic syndrome was diagnosed based on the South Asian Modified National Cholesterol Education Program Adult Treatment Panel III (SAM-NCEP) criteria.
Statistical analysis
Data obtained was tabulated and analyzed. IBM Statistical Package for the Social Sciences version 22 Armonk, NY: IBM Corp was used for statistical analysis. Mean values of carotid intima-media thickness of both sides and epicardial fat thickness parameters were compared between the study groups using independent sample t-test (2 groups). Association between carotid intima-media thickness right and left, epicardial fat thickness and psoriasis area and severity index scores were assessed by calculating the Pearson rank correlation (r) coefficient and the data was represented in a scatter diagram. Pearson rank correlation (r) coefficient was interpreted as follows- 0: no correlation, <0.3: poor correlation, 0.3–0.5: moderate correlation, 0.5–0.7: good correlation, >0.7: strong correlation and 1: perfect correlation.14 Linear regression analysis was done to check the effect of confounding factors. Unadjusted regression coefficient and P-values were presented. Variables with statistical significance in univariate analysis were used to compute multivariate regression analysis. The regression coefficient along with their 95% confidence interval was presented.
P-value <0.05 was considered statistically significant.
Results
Among the 100 subjects who participated in the study, 80 were men and 20 were women with a male:female ratio of 4:1. The youngest was 18 years old and the eldest was 68 years old. Seventy two subjects (72%) belonged to the age group of 30–50 years. Among psoriasis patients, the duration of psoriasis varied from 1 month to 288 months. Twenty nine patients (58%) had <5 years duration of psoriasis whereas 21 patients (42%) had a prolonged course of psoriasis of more than 5 years. A family history of psoriasis was seen in two (4%) and a family history of cardiovascular disease was noted in 3 (6%) of the psoriatic patients. Obesity and overweight categories based on BMI were seen in 21 (42%) and 15 (30%) of the psoriasis cases respectively. Among these patients with high body mass index, 13 patients had moderate and 17 patients had severe psoriasis area and severity index scores. There was no correlation between the duration and severity of psoriasis in our study (r-value: -0.032, P-value= 0.825). Epicardial fat thickness ranged from 0.8 to 4.1 mm. Mean epicardial fat thickness was significantly higher among psoriasis patients (1.76 ± 0.66 mm) than in controls (1.49 ± 0.47 mm) (P-value = 0.02). Epicardial fat thickness was poorly correlated with the severity of psoriasis (psoriasis area and severity index score) and the disease duration. Mean carotid intima-media thickness of both the carotids were significantly higher in psoriatic patients when compared to controls. Carotid intima-media thickness of both the carotids poorly correlated with the severity of the disease (psoriasis area and severity index score). There was a moderately positive correlation between epicardial fat thickness with carotid intima-media thickness of right carotid (r = 0.348, P = 0.013) and carotid intima-media thickness of left carotid (r = 0.374, P = 0.007) which are shown in Figures 1 and 2. Table 1 shows the various characteristics of the study population.
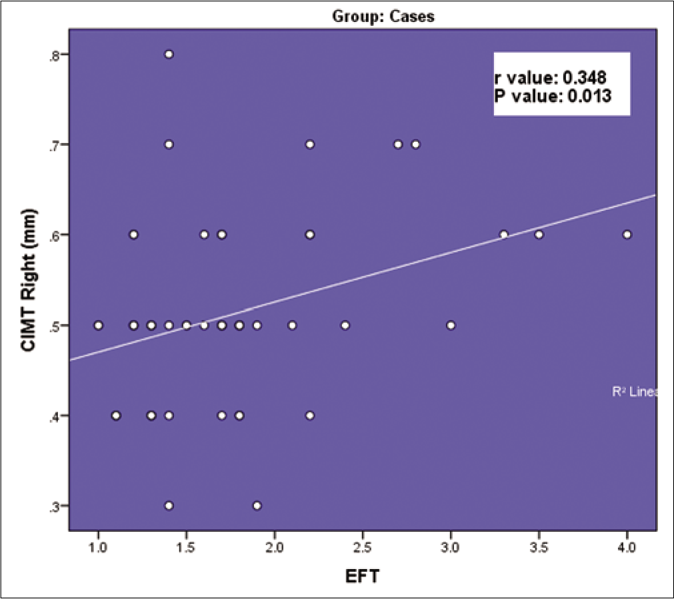
- Correlation between carotid intima-media thickness right carotid and epicardial fat thickness
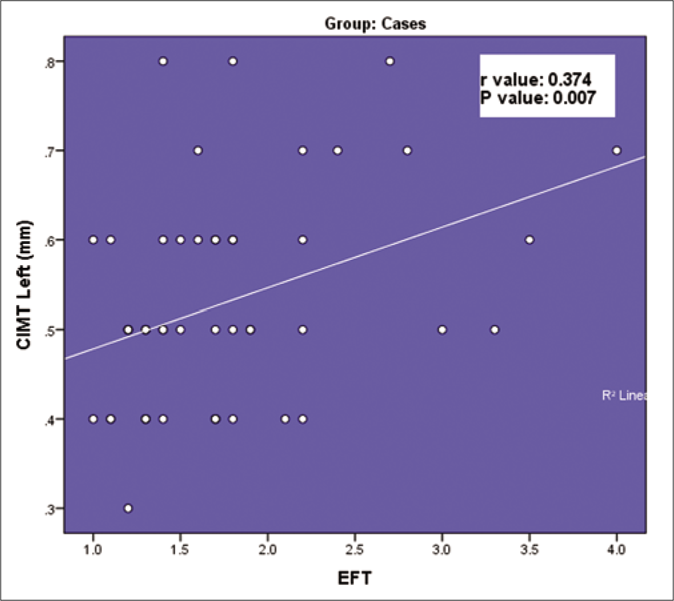
- Correlation between carotid intima-media thickness left carotid and epicardial fat thickness
| Parameters | Results | P | |
|---|---|---|---|
| Psoriasis patients | Controls | ||
| Age (years) | 41.82±12.15 | 42.2±12.33 | |
| Duration of psoriasis (months), | 66.42±62.80 | ||
| mean±SD | |||
| Current alcoholic, n (%) | 13 (26) | 5 (10) | |
| Current smoker, n (%) | 16 (32) | 6 (12) | |
| Nail involvement, n (%) | 24 (48) | ||
| Scalp involvement, n (%) | 26 (52) | ||
| PASI, mean±SD | 12.80±4.929 | ||
| BMI (kg/m2), mean±SD | 24.25±2.63 | 22.66±2.48 | 0.002* |
| Systolic BP (mmHg), | 122.24±9.89 | 118.44±8.55 | 0.043* |
| mean±SD | |||
| Diastolic BP (mmHg), | 81.32±7.89 | 81.44±7.82 | 0.939 |
| mean±SD | |||
| Hip circumference (cm), | 90.70±9.72 | 92.92±8.34 | 0.223 |
| mean±SD | |||
| Waist circumference (cm), | 96.14±10.41 | 97.44±8.30 | 0.492 |
| mean±SD | |||
| Waist-hip ratio, mean±SD | 0.90±0.04 | 0.90±0.01 | 0.742 |
| CIMT left (mm), mean±SD | 0.53±0.12 | 0.48±0.1 | 0.041* |
| CIMT right (mm), mean±SD | 0.51±0.1 | 0.47±0.1 | 0.038* |
| Average CIMT (mm), | 0.52±0.1 | 0.48±0.08 | 0.015* |
| mean±SD | |||
| EFT (mm), mean±SD | 1.76±0.66 | 1.49±0.47 | 0.020* |
The prevalence of metabolic syndrome was significantly high in psoriasis cases than in controls (29 [58%] vs 18 [36%] odds ratio = 2.46, 95% confidence interval 1.02–5.95; P = 0.028). We compared mean carotid intima-media thickness and mean epicardial fat thickness in subjects with metabolic syndrome and those without metabolic syndrome and found no statistical significance implying metabolic syndrome was not influencing carotid intima-media thickness and epicardial fat thickness in our study population. To see the effect of obesity on the epicardial fat thickness and carotid intima-media thickness, we did a comparison of median carotid intima-media thickness and median epicardial fat thickness across body mass index categories and found that they were not significantly different.
Linear regression analysis was done to check the effect of factors influencing carotid intima-media thickness and epicardial fat thickness among the study population. During univariate analysis, carotid intima-media thickness was found to be significantly affected by serum triglycerides as shown in Table 2. Univariate linear regression analysis of epicardial fat thickness showed a statistically significant association with age and systolic blood pressure. During multivariate linear regression analysis, after controlling potential confounding variables, the factors which showed statistically meaningful association were age and systolic blood pressure as shown in Table 3.
| Parameter | Univariate analysis regression coefficient | 95% Confidence interval | P | |
|---|---|---|---|---|
| Lower | Upper | |||
| Age | 0.201 | −0.001 | 0.003 | 0.162 |
| Gender (baseline=man) | −0.173 | −0.090 | 0.022 | 0.231 |
| Smoking | −0.068 | −0.030 | 0.015 | 0.501 |
| Alcoholic | −0.001 | −0.024 | 0.023 | 0.991 |
| BMI category 25/above obesity | 0.150 | −0.010 | 0.69 | 0.137 |
| Systolic BP | 0.233 | 0.000 | 0.005 | 0.104 |
| Diastolic BP | 0.193 | −0.001 | 0.005 | 0.179 |
| MetS | 0.023 | −0.023 | 0.041 | 0.823 |
| FBS | 0.064 | −0.001 | 0.003 | 0.529 |
| Serum cholesterol | 0.134 | 0.000 | 0.001 | 0.183 |
| TGL | 0.215 | 0.000 | 0.001 | 0.031* |
| HDL | −0.120 | −0.002 | 0.000 | 0.233 |
| LDL | 0.051 | 0.000 | 0.001 | 0.616 |
| VLDL | 0.147 | 0.000 | 0.003 | 0.146 |
| PASI | 0.196 | −0.002 | 0.010 | 0.173 |
P <0.05 - significant*. BMI: body mass index, FBS: fasting blood sugar, TGL: triglycerides, HDL: high-density lipoprotein, LDL: low-density lipoprotein, VLDL: very-low-density lipoprotein, PASI: psoriasis area and severity index, BP: blood pressure, MetS: metabolic syndrome
| Parameter | Univariate analysis regression coefficient | 95% Confidence interval | P | Multivariate analysis regression coefficient | P | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Age | 0.292 | 0.005 | 0.023 | 0.003* | 0.232 | 0.021* |
| Gender (baseline=man) | −0.191 | −0.565 | 0008 | 0.057 | ||
| Smoking | 0.048 | −0.108 | 0.176 | 0.635 | ||
| Alcoholic | 0.089 | −0.083 | 0.217 | 0.378 | ||
| BMI category 25/above- obese | −0.012 | −0.267 | 0.238 | 0.909 | ||
| Systolic BP | 0.279 | 0.005 | 0.029 | 0.005* | 0.214 | 0.033* |
| Diastolic BP | 0.066 | −0.010 | 0.020 | 0.513 | ||
| MetS | 0.142 | −0.066 | 0.397 | 0.160 | ||
| FBS | 0.183 | −0.006 | 0.02 | 0.203 | ||
| Serum cholesterol | 0.000 | −0.004 | 0.004 | 0.996 | ||
| TGL | −0.023 | −0.003 | 0.002 | 0.823 | ||
| HDL | −0.130 | −0.011 | 0.002 | 0.198 | ||
| LDL | −0.051 | −0.005 | 0.003 | 0.612 | ||
| VLDL | 0.018 | −0.010 | 0.012 | 0.860 | ||
| Psoriasis area index | 0.194 | −0.012 | 0.064 | 0.177 | ||
*P<0.05 - significant. BMI: body mass index, FBS: fasting blood sugar, TGL: triglycerides, HDL: high-density lipoprotein, LDL: low-density lipoprotein, VLDL: very-low-density lipoprotein, PASI: psoriasis area and severity index, MetS: metabolic syndrome
Discussion
Psoriasis as an independent risk factor for cardiovascular aggravation was first proposed by Gelfand et al.15 The underlying process is atherosclerosis which results from an interaction between the immune mechanisms and metabolic abnormalities within the vessel wall. Boehncke et al. coined the term “psoriatic march” to explain the progression of atherosclerosis in psoriatic disease.16 Carotid intima-media thickness is a noninvasive, diagnostic tool to identify early stages of subclinical atherosclerosis. The pathogenesis of accelerated atherosclerosis and increased risk of coronary artery disease in psoriasis is unknown but is likely to be multifactorial as described below.15-18
Psoriasis patients have a higher incidence of conventional cardiovascular risk factors such as obesity, diabetes, hypertension and low physical activity when compared to those without psoriasis
Both psoriasis and coronary artery disease share common risk factors such as smoking and alcohol consumption
Some medications used to treat psoriasis also contributes to the increased risk of coronary artery disease in psoriatic patients. Usage of methotrexate was associated with hyperhomocysteinemia, a risk factor for coronary artery disease. Acitretin and cyclosporine result in lipid abnormalities. Moreover, cyclosporine use causes elevated blood pressure
Misdiagnosis and inadequate treatment of coronary artery disease in patients with psoriasis
Both psoriasis and atherosclerosis are chronic inflammatory diseases with an overlap of inflammatory markers and mediators in cutaneous lesions of psoriasis and atherosclerotic plaques.
Studies using the carotid intima-media thickness as a marker, have shown significantly higher prevalance of subclinical atherosclerosis in psoriatic arthritis patients.19-20 Hypertension, raised total cholesterol, increased low-density lipoprotein- cholesterol, elevated triglycerides, high apoB/apoA-1 ratio, raised serum leptin, insulin resistance and longer duration of the disease are known risk factors for subclinical atherosclerosis in psoriasis patients leading to higher carotid intima-media thickness.21,22 We found significantly high carotid intima-media thickness in psoriatic patients compared to controls.. Smoking, obesity and systolic blood pressure were the significant risk factors noted in our study population. Maintaining a healthy lifestyle by the cessation of smoking, reduction in weight, daily exercise and regular monitoring of blood pressure will alleviate the risk of development of atheroma in psoriasis patients. In addition, one has to keep in mind the fact that psoriasis itself can increase the risk of atherosclerosis without any atherogenic risk factors, as demonstrated by Altekin et al.23
Epicardial fat thickness is ectopic visceral fat which is known to secrete inflammatory cytokines such as tumor necrosis factor-α and interleukin (IL)-6. These pro-inflammatory and proatherogenic mediators were found to affect coronary arteries.13 A systematic review and meta analysis found that epicardial fat thickness, measured by echocardiography was significantly increased in patients with coronary artery disease than those without it.9 Meenakshi et al. noted that epicardial fat thickness was independatly and linearly associated with coroanry artery disease and its severity.24 Epicardial fat thickness is measured at end-systole or end-diastole and it can be affected by age, gender and race. A normal upper limit value for epicardial fat thickness has not been established yet.25 Figure 3 shows epicardial fat thickness in a patient of psoriasis. A study on Asian subjects, undergoing first coronary angiography for chest pain found that epicardial fat thickness >3 mm, measured by transthoracic echocardiography, was an independent risk factor for coronary artery disease.26 Eroğlu suggested, epicardial fat thickness >5mm measured by transthoracic echocardiography as abnormal.25 A study on white subjects found that epicardial fat thickness of 9.5mm and 7.5 mm predict metabolic syndrome in men and women, respectively.27 The epicardial fat thickness ranged from 0.8 to 4.1 mm in our study and it was significantly higher in psoriasis patients compared to controls (P = 0.020). It is a noteworthy observation that previous studies had included manifest coronary artery disease hence, the epicardial fat thickness was higher in them. Table 4 shows the epicardial fat thickness in psoriatic patients in various studies. As none of our patients had evident coronary artery disease and other comorbid conditions, the epicardial fat thickness was relatively lesser. Other factors such as genetic makeup, cultural and social differences in the south Indian population which formed our study population could have contributed to this finding. A Turkish study with psoriasis patients and control group having similar SCORE project risk scores (which determines the 10 year risk of fatal cardiovascular disease), found that epicardial fat thickness was high in patients with psoriasis. They also found that epicardial fat thickness was significantly correlated with metabolic syndrome in psoriasis patients.28 Small sample size (31cases vs 32 controls) was the limiting factor of this study. At present, there is enough evidence for the association of coronary artery disease and its risk factors with psoriasis. Since epicardial fat thickness was significantly high in psoriatic patients compared to controls in our study, we could assume that it reflects a precoronary artery disease status. Another observation we made was an independent association of age and systolic blood pressure with epicardial fat thickness. Both age >45 years and systemic hypertension of 140/90 mmHg are known as traditional risk factors for coronary artery disease. We believe epicardial fat thickness may serve as a marker for future coronary artery disease in psoriatic patients.
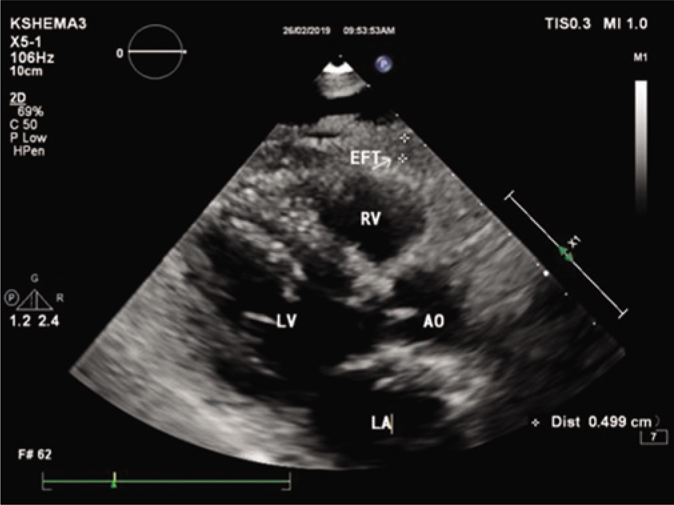
- Measurement of epicardial fat thickness by transthoracic echocardiography
| Study | Place | Method of measurement | Mean EFT in psoriasis patients | Mean EFT in controls | P |
|---|---|---|---|---|---|
| Bacaksiz et al.10 | Turkey | TTE | 5.7±1.2 mm | 4.1±1.0 mm | <0.001* |
| Bulbul Sen et al.13 | Turkey | TTE | 7.3±0.5 mm | 6.5±0.5 mm | < 0.01* |
| Balci et al.17 | Turkey | MDCT | 13.8±8.4 cm2 | 9.7±6.4 cm2 | 0.002* |
| Akyildiz et al.28 | Turkey | TTE | 6.4±2.6 mm | 5.1±1.9 mm | 0.027* |
| Torres et al.29 | Portugal | MDCT | 101.4±55.52 mL | 92.2±38.33 mL | <0.001* |
| Present | India | TTE | 1.76±0.66 mm | 1.49±0.47 mm | 0.020* |
*P <0.05 - significant. TTE: transthoracic echocardiography, EFT: epicardial fat thickness, MDCT: multidetector computed tomography
The epicardial fat thickness and carotid intima-media thickness were positively correlated in patients with psoriasis in our study. Torres et al., in Portuguese subjects, found that epicardial fat thickness was high in psoriasis, independent of age, sex and abdominal visceral fat, compared to controls. They used multidetector computed tomography for measuring epicardial fat thickness and included psoriasis patients with PASI>10. Epicardial fat thickness was associated with subclinical atherosclerosis in psoriasis patients in their study.29 Bulbul Sen et al. also found that epicardial fat thickness was correlated with carotid intima-media thickness in patients with psoriasis.13 As carotid intima-media thickness is associated with subclinical atherosclerosis and epicardial fat thickness with precoronary artery disease state, combining these markers for screening psoriasis patients will help in recognition of the disease, before manifest coronary artery disease sets in. Intervention strategies for coronary artery disease, if instituted at this stage may significantly reduce morbidity and mortality. As we were unable to find previous studies, this is probably the first study from India correlating epicardial fat thickness and carotid intima-media thickness in psoriasis patients.
Limitations
Small sample size
The cross-sectional design of the study, where the patients were not under regular follow-up
The gold standard method for assessing epicardial fat thickness is magnetic resonance imaging and it was not used. As epicardial fat thickness has a 3-dimensional distribution, 2D echo may not give accurate information.
Both carotid intima-media thickness and epicardial fat thickness measurements could have inter- and intra-observer variability.
Smoking could have affected the final outcome of the study.
Conclusion
Epicardial fat thickness was positively correlated with carotid intima-media thickness in chronic plaque psoriasis.
Acknowledgment
We would like to thank the NITTE (Deemed to be University) for providing financial assistance in the form of a research grant to conduct this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
This study was financially supported by a research grant given to Dr. Girisha B S from NITTE (Deemed to be University).
Conflicts of interest
There are no conflicts of interest.
References
- Psoriasis: Epidemiology, clinical features, and quality of life. Ann Rheum Dis. 2005;64(Suppl 2):ii18-23.
- [CrossRef] [PubMed] [Google Scholar]
- Psoriasis: Classical and emerging comorbidities. An Bras Dermatol. 2015;90:9-20.
- [CrossRef] [PubMed] [Google Scholar]
- Psoriasis and risk of nonfatal cardiovascular disease in U.S. women: A cohort study. Br J Dermatol. 2012;166:811-8.
- [CrossRef] [PubMed] [Google Scholar]
- Comorbidities in psoriasis. Indian J Dermatol Venereol Leprol. 2013;79(Suppl 7):S10-7.
- [CrossRef] [PubMed] [Google Scholar]
- Psoriasis and risk of heart failure: A nationwide cohort study. Eur J Heart Fail. 2014;16:743-8.
- [CrossRef] [PubMed] [Google Scholar]
- Psoriasis and cardiovascular comorbidities: Focusing on severe vascular events, cardiovascular risk factors and implications for treatment. Int J Mol Sci. 2017;18
- [CrossRef] [PubMed] [Google Scholar]
- Imaging atherosclerosis by carotid intima-media thickness in vivo: How to, where and in whom. ? Maedica (Buchar). 2012;7:153-62.
- [Google Scholar]
- Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force, Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. 2008;21:93-111.
- [CrossRef] [PubMed] [Google Scholar]
- Is echocardiographic epicardial fat thickness increased in patients with coronary artery disease? A systematic review and meta-analysis. Electron Physician. 2018;10:7249-58.
- [CrossRef] [PubMed] [Google Scholar]
- Epicardial fat thickness in patients with psoriasis vulgaris. Turk Kardiyol Dern Ars. 2014;42:47-54.
- [CrossRef] [PubMed] [Google Scholar]
- Consensus statement for diagnosis of obesity, abdominal obesity and the metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical management. J Assoc Physicians India. 2009;57:163-70.
- [Google Scholar]
- The psoriasis area and severity index is the adequate criterion to define severity in chronic plaque-type psoriasis. Dermatology. 2005;210:194-9.
- [CrossRef] [PubMed] [Google Scholar]
- Increased epicardial fat tissue is a marker of subclinical atherosclerosis in patients with psoriasis. Br J Dermatol. 2013;169:1081-6.
- [CrossRef] [PubMed] [Google Scholar]
- Biostatistics series module 6: Correlation and linear regression. Indian J Dermatol. 2016;61:593-601.
- [CrossRef] [PubMed] [Google Scholar]
- Risk of myocardial infarction in patients with psoriasis. JAMA. 2006;296:1735-41.
- [CrossRef] [PubMed] [Google Scholar]
- The 'psoriatic march': A concept of how severe psoriasis may drive cardiovascular comorbidity. Exp Dermatol. 2011;20:303-7.
- [CrossRef] [PubMed] [Google Scholar]
- Patients with psoriasis have an increased amount of epicardial fat tissue. Clin Exp Dermatol. 2014;39:123-8.
- [CrossRef] [PubMed] [Google Scholar]
- Psoriasis and cardiovascular disease risk factors: The HUNT study, Norway. J Eur Acad Dermatol Venereol. 2018;32:776-82.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and risk factors of atherosclerosis in patients with psoriatic arthritis. Semin Arthritis Rheum. 2007;36:203-9.
- [CrossRef] [PubMed] [Google Scholar]
- High prevalence of subclinical atherosclerosis in psoriatic arthritis patients without clinically evident cardiovascular disease or classic atherosclerosis risk factors. Arthritis Rheum. 2007;57:1074-80.
- [CrossRef] [PubMed] [Google Scholar]
- Association of carotid intima-media thickness with leptin and apoliprotein b/apoliprotein a-I ratio reveals imminent predictors of subclinical atherosclerosis in psoriasis patients. Acta Medica (Hradec Kralove). 2014;57:21-7.
- [CrossRef] [PubMed] [Google Scholar]
- A study of cardio-metabolic risk profile in patients with psoriasis. J Assoc Physicians India. 2013;61:798-803.
- [Google Scholar]
- Determination of subclinical atherosclerosis in plaque type psoriasis patients without traditional risk factors for atherosclerosis. Turk Kardiyol Dern Ars. 2012;40:574-80.
- [CrossRef] [PubMed] [Google Scholar]
- Epicardial fat thickness: A surrogate marker of coronary artery disease-Assessment by echocardiography. Indian Heart J. 2016;68:336-41.
- [CrossRef] [PubMed] [Google Scholar]
- How do we measure epicardial adipose tissue thickness by transthoracic echocardiography? Anatol J Cardiol. 2015;15:416-9.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship of epicardial adipose tissue by echocardiography to coronary artery disease. Heart. 2008;94:e7.
- [CrossRef] [PubMed] [Google Scholar]
- Threshold values of high-risk echocardiographic epicardial fat thickness. Obesity (Silver Spring). 2008;16:887-92.
- [CrossRef] [PubMed] [Google Scholar]
- Epicardial fat thickness is independently associated with psoriasis. Dermatology. 2014;228:55-9.
- [CrossRef] [PubMed] [Google Scholar]
- Epicardial adipose tissue and coronary artery calcification in psoriasis patients. J Eur Acad Dermatol Venereol. 2015;29:270-7.
- [CrossRef] [PubMed] [Google Scholar]




