
Translate this page into:
Pigmented transverse nasal band: A review
Corresponding author: Prof. Rashmi Sarkar, Department of Dermatology, Lady Hardinge Medical College and Hospitals, New Delhi, India. rashmisarkar@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Agarwal K, Podder I, Sarkar R. Pigmented transverse nasal band: A review. Indian J Dermatol Venereol Leprol 2022;88:144-7.
Abstract
Pigmented transverse nasal band/groove is an asymptomatic benign condition, characterized by the development of erythematous to hyperpigmented, well-demarcated, transverse groove at the junction of middle and lower two-third of the nasal dorsum. Although the pathogenesis is unclear, embryologic origin seems to be the most plausible hypothesis. This condition is often associated other related dermatological conditions such as milia, comedones, seborrheic dermatitis and atopic dermatitis. Diagnosis is mostly clinical, while reassurance is the mainstay of therapy. In persistent cases, topical retinoids have been used. In this article, we have reviewed the different aspects of this condition including treatment, along with the recent updates to create awareness about this dermatological entity.
Keywords
Pigmented transverse nasal band
seborrheic dermatitis
transverse nasal crease
transverse nasal groove
transverse nasal line

Introduction
Pigmented transverse nasal band is an under-reported entity in dermatology. It is also known as transverse nasal line, transverse nasal strip, transverse nasal crease and stria nasi transversa.1 This entity presents at the junction of upper two-third and lower one-third of the nose, just proximal to alae nasi. Clinically, it presents as 1–2 mm hyperpigmented transverse band or groove on the dorsum of the nose which extends from end to end.2 It is widely believed to be an embryological defect.3 However, this entity has failed to garner significant interest until recently due to its asymptomatic presentation.
This article is aimed to provide a comprehensive review of this condition encompassing its etiopathogenesis, diagnosis and the various treatment modalities along with relevant review of literature.
Materials and Methods
We undertook a comprehensive English literature search across multiple databases such as PubMed, SCOPUS, EMBASE, MEDLINE and Cochrane using keywords (alone and in combination) and MeSH items such as “PTNB” AND “pigmented transverse nasal groove” AND “transverse nasal groove” AND “transverse nasal line,” “transverse nasal strip” AND “transverse nasal crease” AND “stria nasi transversa” to obtain several relevant articles, priority being given to prospective randomized controlled trials. We scanned all the relevant articles to obtain the following: observational studies – 2, case report/short communication – 10 and book chapter – 1. Additional data were obtained from the reference list of already selected articles. In case of any discrepancy, the concerned articles were discussed at research meetings to arrive at a consensus. We divided the articles into two categories: clinical studies and case report/short communication/book chapter. Each article was meticulously analyzed to obtain the following information: etiopathogenesis, clinical features, diagnosis, differentials and treatment. Articles not written in English were excluded as were clinical images and those describing other causes of transverse nasal pigmentation such as allergic rhinitis and previous cutaneous scarring.
Discussion
Epidemiology
Transverse nasal groove or its pigmented variant was first described in 1951 by Cornbleet.1 An incidence of 0.3% has been reported in the Indian population;4 thus making it a relatively rare cutaneous disorder.
It occurs sporadically in the general population. A familial basis has been reported by Anderson which is supported by an Indian study that reports 15% familial incidence.2,4 A female preponderance has also been reported by Sathyanarayana et al.4 This may be a reflection of more female patients consulting a dermatologist for this problem due to cosmetic concerns.
This condition mostly affects adolescents and young adults with incidence peaking during the 3rd decade4,5 in skin of color. However, western studies report greater prevalence amongst children.1,2 In addition, Wimmershoff et al. reported two cases that presented at birth.6 There might be a genetic7 and racial predilection8 in Caucasians.
Etiopathogenesis
The exact etiology of this condition is still unclear,4 and various etiologic theories have been proposed overtime.
Cornbleet hypothesized a developmental defect of nasal cartilage to be the primary etiologic factor.1 In the nose, there are two upper lateral nasal cartilages and two lower lateral nasal cartilages. Both upper and lower lateral cartilages are attached to each other, and the former is also attached to the under surface of the nasal bone by fibrous septae. The occurrence of transverse nasal band has been attributed to the abnormal fibrous attachments between the cartilage-cartilage and the bone-cartilage junctions.
Therefore, the lesion occurs at the junction of two upper lateral nasal cartilages and the two lower lateral nasal cartilages. This site roughly corresponds to the junction of upper two-third and lower one-third of nose clinically. However, there can be slight variation of this clinical landmark because of the variation in size of nasal bone and cartilage among different individuals. For example, in case of a larger lower lateral nasal cartilage, the lesion may shift a few millimeters upwards.4,7
Anderson suggested a genetic predisposition, due to the inheritance of a single dominant gene.2 An embryological origin has also been proposed by Shelley et al., as the nose forms at six weeks of gestation by fusion of medial nasal process with frontonasal process.3,9 The tip of the nose has its own embryological folds or grooves, despite being a part of frontonasal process, and this accounts for the existence of pigmented transverse nasal band or line.3
Even though the above theories have been suggested to account for transverse nasal crease, the cause of pigmentation is yet not clear.7
Clinical features
Pigmented transverse nasal band or crease is situated at the junction of middle and lower third of nose [Figure 1] just proximal to alae nasi or a few millimeters above this junction, due to interindividual variation in size of nasal cartilage.7

- (a) Pigmented transverse nasal band, (b) Transverse nasal view (close-up view), (c) Aging wrinkles (courtesy Dr. Saloni Katoch), (d) Melasma involving the dorsum of nose (courtesy Dr. Surabhi Sinha)
It may present as a faint erythematous line to a groove with depth of several millimeteres.10,11 The groove is well demarcated, extends transversely along the dorsum of nose, 1–3 mm in width and about 1 mm in depth. It is more prominent in adolescents and becomes shallower with age.2 By the end of the fifth decade, only a faint hyperpigmented transverse band can be ssen.5
This condition belongs to a subset of transverse nasal lesions that have different clinical presentations.4,7 Transverse nasal groove is the earliest morphological description, subsequently, other morphologies such as line, strip, ridge and loop have been reported.4
The transverse nasal line appears as a 1–2 mm hyperpigmented, thread-like structure whereas transverse nasal strip presents as 3–5 mm hyperpigmented, transverse band, neither demonstrating any surface change nor depression.4 The ridge presents clinically as a transverse elevated lesion of about 1 mm running across the nose bridge.4 In addition to the above, a loop-like groove has been described which originates and ends in the nasolabial fold with the apex over the dorsal nasal bridge subsequently forming a triangular area between the two grooves.4
This condition is usually asymptomatic, but concomitant development of milia, pseudocomedones and cysts within the groove has been reported in some cases.12 Waller et al. proposed transverse nasal crease and transverse nasal milia as clinical variants of the same entity. The two entities occur together because the alar and the triangular cartilage attach linearly at the junction of the middle and lower third of the nose, thus produce a potential embryonic fault line in which retention cysts (milia and comedones) can occur.11
Transverse nasal groove has been reported in association with various dermatological diseases such as seborrheic dermatitis, dermatosis papulosa nigra, ichthyosis, acne vulgaris and atopic dermatitis.4,7 Among all of the above, it is most commonly associated with seborrheic dermatitis.4 Recently, Chillag et al.13 have proposed its association with atherosclerotic cardiovascular disease and proposed it as a predictive marker, however, further studies are needed to validate this claim.
Diagnosis
Pigmented transverse nasal band is an underdiagnosed entity primarily because of its asymptomatic nature and lack of awareness among the general population. These patients present to the dermatologist either due to esthetic concerns or if there is development of concomitant milia, pseudocomedones or cysts.
The diagnosis of transverse nasal crease is essentially clinical, because of its typical presentation. Family history of similar lesions and other associated dermatological conditions such as seborrheic dermatitis, ichthyosis, acne vulgaris and atopic dermatitis may provide additional diagnostic clues. Detailed laboratory or histopathological investigations are mostly not required. Moreover, its histopathological study is usually avoided as a biopsy adjacent to the cartilaginous portion of nose is considered to be dangerous.5
Recently, dermoscopy has emerged as a non-invasive, rapid diagnostic modality, and it has been performed in this condition also [Figure 2]. On dermoscopy, transverse nasal crease demonstrates intermittent, thin, white transverse streaks which are more prominent at the center of nose and gradually fade away toward the periphery. It is hypothesized that these streaks represent fibrosed adhesions to the nasal cartilage. There may be the presence of microcomedones and milia in the white streaks which are better visible on dermoscopy although inconspicuous clinically. These retention cysts appear as white round structures, 0.5–1 mm in diameter indicating milia or as white to brown spots <0.5 mm in diameter representing microcomedones.14
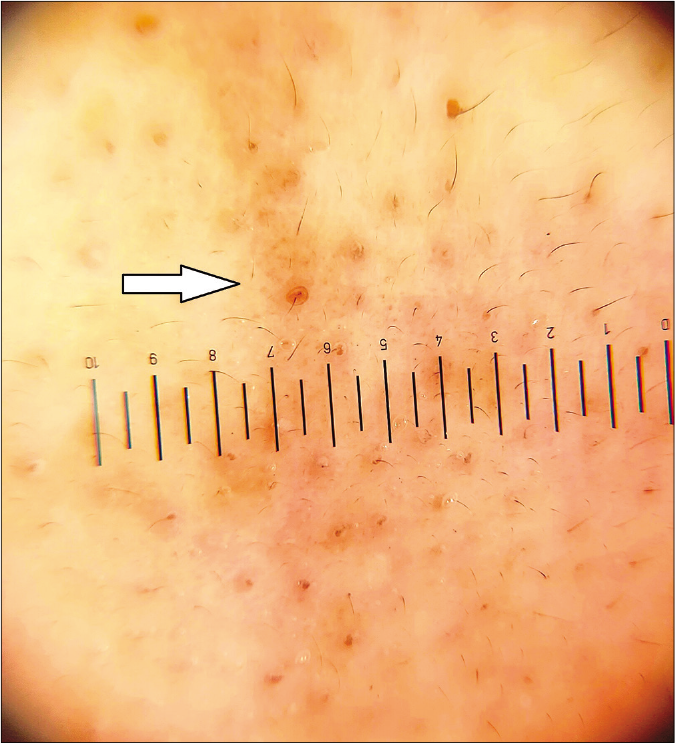
- Pigmented transverse nasal band showing brownish dot on dermoscopy indicative of microcomedone, Heine Delta 20 T (×10)
Differential diagnosis
Pigmented transverse nasal band or crease needs to be differentiated from other transverse lesions on the nose such as crease of allergic rhinitis (allergic salute) and wrinkles of photoaging/chronological aging [Figure 1c]. The distinguishing clinical features have been tabulated below [Table 1]. Another important and common differential is seborrheic melanosis which is characterized by the formation of a brown-black pigmented line along the nasal creases and angle of the mouth (contrary to pigmented transverse nasal band that presents as a band on dorsum of nose). In some cases of alkaptonuria, nasal pigmentation may be observed, but it is usually localized near the tip without any band-like disposition. Associated skin thickening may be an additional finding (contrary to band-like pigmentation on dorsal nose in transverse nasal groove without thickened skin).15 Occasionally, melasma may occur on the dorsum of nose resembling transverse nasal strip [Figure 1d]; however, it can be differentiated by the classical involvement of malar areas.
| Pigmented transverse nasal band | Crease of allergic rhinitis | Wrinkles due to photoaging or old age |
|---|---|---|
| Usually presents as a solitary lesion | Mostly a collection of short, transverse wrinkles | Multiple creases in number |
| The band does not disappear on stretching the skin | The creases disappear on stretching the skin | The wrinkles flatten on stretching the skin |
| The band usually occupies the full width of nose | These are short creases which do not extend the full width of nose | Short wrinkles not involving the full nasal width |
| May be associated with other dermatological disorders such as seborrheic dermatitis, dermatosis papulosa nigra, ichthyosis, acne vulgaris and atopic dermatitis. | Always associated with allergic rhinitis “allergic crease,” “allergic salute” (constant upward rubbing of the nose) and “allergic shiner” (darkening of the lower eyelid) constitute the three facial hallmarks of patients of allergic rhinitis the three facial hallmarks of patients of allergic rhinitis. | Associated with other signs of photoaging such as dyspigmentation, senile comedones, loose and lax skin |
Treatment
Pigmented transverse nasal band or crease is an asymptomatic condition and requires minimal intervention. However, dermatologists need to be aware of this disorder, and reassurance is needed to allay the cosmetic concerns. In severe cases, topical retinoids may be tried which have shown some improvement in this condition, especially when associated with milia and comedones.7 Similarly, mild-to-moderate potency topical steroids may show some improvement if associated with seborrheic dermatitis, especially mitigating the inflammatory features such as erythema, scaling and pruritus. No systemic therapy has been tried for it till date and there is not much evidence in the present literature regarding use of physical modalities such as lasers and peels. Any surgical intervention should be strictly avoided, to prevent damage to underlying structures such as nasal cartilage and transverse nasal vein.16
Authors’ comment
The authors feel that reassurance should be the cornerstone of managing this condition, as it is essentially a benign condition with cosmetic concerns only. However, in persistent cases or anxious patients, topical retinoids may be used to provide symptomatic benefit. The prognosis of the condition is also good because of its asymptomatic nature. It does not interfere with daily activities of the individual.
Conclusion
Pigmented transverse nasal band or transverse nasal crease is an asymptomatic lesion seen on dorsum of nose, mostly affecting the females. The diagnosis is essentially clinical because of its typical presentation. Dermoscopy is an adjunct investigation which may help to clinch the diagnosis. Several seborrheic conditions may be associated with this condition along with atopic dermatitis. It needs to be differentiated from related clinical entities such as allergic nasal crease and aging wrinkles to institute appropriate treatment. However, its association with cardiovascular diseases as a predictive marker needs more large-scale studies to corroborate this view. Because of its benign nature, reassurance is usually sufficient. However, in persistent cases, topical retinoids may be used to lighten the pigmentation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Transverse nasal stripe at puberty (stria nasi transversa) AMA Arch Derm Syphilol. 1951;63:70-2.
- [CrossRef] [Google Scholar]
- The transverse nasal line: An embryonic fault line. Br J Dermatol. 1997;137:963-5.
- [CrossRef] [Google Scholar]
- Appraisal of transverse nasal groove: A study. Indian J Dermatol Venereol Leprol. 2012;78:439-42.
- [CrossRef] [Google Scholar]
- A survey for transverse nasal groove. Indian J Dermatol Venereol Leprol. 1989;55:105-7.
- [Google Scholar]
- Transverse nasal groove. A rare embryological error in nature. Hautarzt. 2001;52:828-30.
- [CrossRef] [Google Scholar]
- Pigmented transverse nasal band: A distinct presentation. J Cosmet Dermatol. 2019;18:301-2.
- [CrossRef] [Google Scholar]
- The “nasal crease“. A physical sign of allergic rhinitis. JAMA. 1960;174:1204-6.
- [CrossRef] [Google Scholar]
- The developing human In: Clinically Oriented Embryology (5th ed). Philadelphia, PA: WB Saunders Company; 1993.
- [Google Scholar]
- Transverse nasal line associated with congenital persistent milia. Dermatology. 2000;200:151-2.
- [CrossRef] [Google Scholar]
- Transverse nasal crease and transverse nasal milia: Clinical variants of the same entity. Arch Dermatol. 2012;148:1037-9.
- [CrossRef] [Google Scholar]
- Milia cysts along the nasal groove in a child. Clin Exp Dermatol. 1993;18:289-90.
- [CrossRef] [Google Scholar]
- Transverse nasal crease with milia and comedones: Dermoscopic observation. J Dermatol. 2018;45:e126-7.
- [CrossRef] [Google Scholar]
- A late diagnosis of alkaptonuria in an elderly patient. Eur Ger Med. 2017;8:178-80.
- [CrossRef] [Google Scholar]
- On distension of the nasal arch (transverse nasal vein) in children; its pathology and treatment. Br Med J. 1887;2:459-71.
- [CrossRef] [Google Scholar]




