
Translate this page into:
A solitary cutaneous plaque unmasking systemic cryptococcosis in an iatrogenically immunosuppressed Indian patient
Corresponding author: Dr. Vishal Gupta, Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi. doctor.vishalgupta@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ahuja R, Pragya P, Karthick Kumar V, Dixit S, Sethi P, Singh G, et al. A solitary cutaneous plaque unmasking systemic cryptococcosis in an iatrogenically immunosuppressed Indian patient. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_864_2024
Dear Editor,
Cutaneous involvement in systemic cryptococcosis is rare and generally presents as widespread skin lesions. We describe a patient who presented with a solitary cutaneous plaque, which upon further evaluation, revealed systemic cryptococcosis.
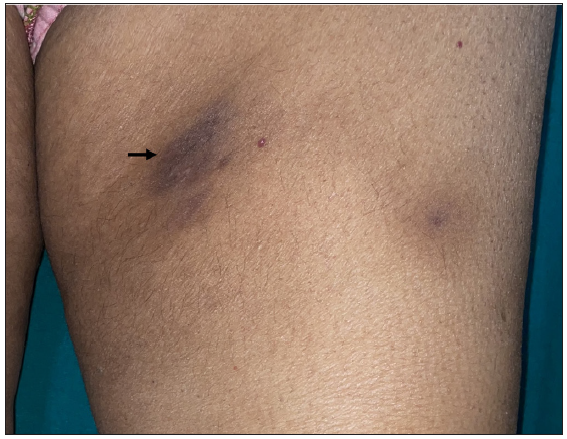
A 48-year-old woman from North India presented with a gradually increasing asymptomatic hyperpigmented plaque on her left inner thigh present for two months. The plaque was non-tender and firm in consistency [Figure 1]. There was no regional lymphadenopathy. Her past medical history included hypertension (controlled on metoprolol and amlodipine) and membranous glomerulonephritis diagnosed three years ago, for which she was being treated with oral prednisolone (10-30 mg/day) and repeated cycles of rituximab. With clinical possibilities of lupus panniculitis, calcifying panniculitis, and thrombophlebitis, a skin punch biopsy was performed from the plaque. Histopathological examination revealed a dense deep dermal granulomatous infiltrate with histiocytes and giant cells containing round to oval pale basophilic yeast forms (5-10 μ in size) suggestive of cryptococcus [Figure 2a-b]. These fungal elements were highlighted on the Periodic acid-Schiff stain [Figure 2c]. On further inquiry, the patient denied fever, weight loss, or other systemic complaints, notably headache, neck stiffness, or neurological deficits. Fungal culture from skin biopsy and blood were negative at six weeks. Enzyme linked immune sorbent assay for human immunodeficiency virus 1 and 2 was negative. Whole-body positron emission tomography scan and contrast-enhanced magnetic resonance imaging of the brain did not reveal any systemic focus of increased uptake or cryptococcoma, respectively. Her serum and cerebrospinal fluid (CSF) tested positive for cryptococcal antigen by latex agglutination assay. CSF analysis was within normal limits except for increased mononuclear cells (20/mm3, range 0-5/mm3), while India ink preparation was negative. In accordance with treatment guidelines, the patient was initiated on liposomal amphotericin B (4 mg/kg/day) along with flucytosine (50 mg/kg/day-renal modified dose) for one month. She was then shifted to oral fluconazole (800 mg/day) for two months (consolidation phase), which resulted in significant softening and flattening of the plaque [Figure 3]. She is now on one-year maintenance therapy with fluconazole (200 mg/day).
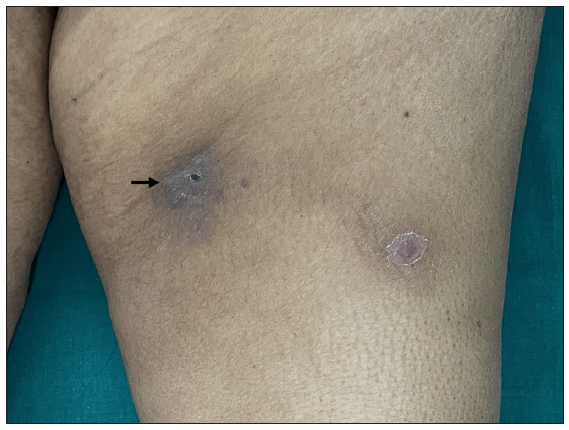
- A solitary well-defined hyperpigmented, firm plaque (black arrow) on the left inner thigh at baseline (The smaller lesion laterally, with a collarette of scale, is a resolving furuncle).
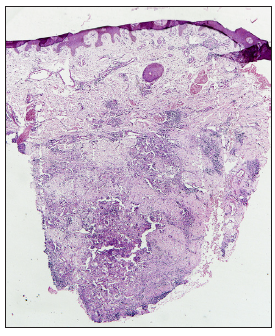
- Dense nodular infiltrate in the mid and deep dermis (Haematoxylin and eosin, 20x)
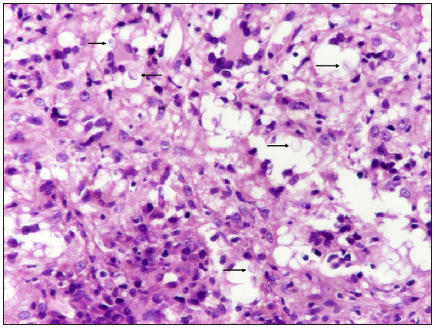
- Infiltrate is composed of histiocytes, lymphocytes, and plasma cells, accompanied by numerous giant cells containing pale basophilic oval yeast forms -black arrow (Haematoxylin and eosin, 400x)
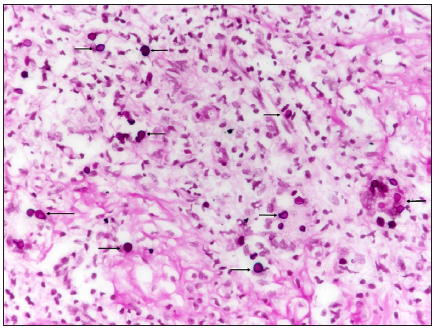
- Encapsulated fungal yeast forms - black arrow (Periodic acid-Schiff, 400x)
- Solitary plaque on the thigh. Softening and flattening of the plaque (black arrow) after the end of consolidation phase.
Cryptococcosis, primarily affecting immunocompromised individuals, is commonly caused by the encapsulated yeast Cryptococcus neoformans and can affect various organs, including the central nervous system, lungs, and skin.1 A 15-year French study revealed that cutaneous involvement was observed in 5.4% (n = 108/1974) of all cases of cryptococcosis, with primary cutaneous cases comprising 25.9% of this subset.2
Cutaneous involvement in systemic cryptococcosis usually presents with generalised skin lesions of variable morphologies, including molluscum-like umbilicated papules, acneiform lesions, purpura, vesicles, nodules, abscesses, ulcers, and draining sinuses. In primary cutaneous cryptococcosis, skin lesions are typically confined to a single area, primarily on exposed skin sites, appearing as solitary lesions resembling subcutaneous nodules, ulcer, cellulitis, whitlow, or even localized infiltrative erythema.2-4
Our patient presented with a non-specific solitary plaque on the thigh. Cryptococcosis was not clinically suspected, and the diagnosis was made only through histopathology. Surprisingly, further investigations revealed cryptococcal antigenemia in the blood and subsequently in the CSF. Rare cases of solitary skin lesions presenting as large tumours and cellulitis in disseminated cryptococcosis have been reported in literature.5,6 Our case was iatrogenically immunosuppressed due to the treatment of membranous glomerulonephritis, which increased her risk for this opportunistic infection. Asymptomatic cryptococcal antigenemia is much less common in immunocompromised patients compared to immunocompetent individuals (6% versus 40%). Central nervous system (CNS) involvement is quite common in immunocompromised patients with cryptococcal antigenemia (71-89%),7 and can be asymptomatic in about half of these cases.8
Through this case, we aim to highlight an unusual clinical presentation of systemic cryptococcosis. Dermatologists should remain alert to the possibility of non-descript skin lesions being a manifestation of atypical infections in immunosuppressed patients. Systemic dissemination should be excluded even in the absence of widespread skin lesions or overt clinical symptoms.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS. 2009;23:525-30.
- [CrossRef] [PubMed] [Google Scholar]
- Primary cutaneous cryptococcosis: A distinct clinical entity. Clin Infect Dis. 2003;36:337-47.
- [CrossRef] [PubMed] [Google Scholar]
- Cutaneous cryptococcus: Marker for disseminated infection. BMJ Case Rep. 2015;2015:bcr2015210898.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Disseminated cryptococcosis manifested as a single tumor in an immunocompetent patient, similar to the cutaneous primary forms. An Bras Dermatol. 2016;91:29-31.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Disseminated cryptococcosis presenting initially as lower limb cellulitis in a renal transplant recipient - a case report. BMC Nephrol. 2018;19:18.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Underlying cryptococcal diseases and the correlation with serum cryptococcal antigen titers in hospitalized HIV-infected patients screened positive for cryptococcal antigenemia. Front Cell Infect Microbiol. 2020;10:170.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Clinical analysis in immunocompetent and immunocompromised patients with pulmonary cryptococcosis in western China. Sci Rep. 2020;10:9387.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




