
Translate this page into:
Focal dermal hypoplasia – A report of two cases with review of literature

Corresponding author: Dr. Adhyatm Bhandari, Department of Dermatology, Venereology and Leprology, AIIMS Bhopal, Madhya Pradesh, India. adhyatm.bhandari@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Denla Y, Gowda SK, M L Amulya, Bhandari A. Focal dermal hypoplasia- A report of two cases with review of literature. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_96_2024
Dear Editor,
Focal dermal hypoplasia, also called ‘Goltz syndrome’, is a rare meso-ectodermal dysplasia with X-linked dominant inheritance with PORCN mutation.1
Index case was a 17-year-old male with hypopigmented atrophic lesions distributed in a linear pattern over the entire body since birth. He was born of a non-consanguineous marriage at full term, with normal spontaneous vaginal delivery and a birth weight of 2.6 kg, and no prior family history of similar illness. There was no history of fluid-filled blisters or verrucous lesions, photosensitivity, hearing loss, mental retardation, developmental delay, hyperhidrosis, hypohidrosis, and oral papillomatosis. On examination, we observed generalised distribution of multiple discrete to confluent atrophic hypopigmented telangiectatic plaques without fat herniation along the lines of Blaschko [Figure 1]. The patient had triangular facies with freckle-like pigmentation. Oral examination revealed hypodontia, diastema, and linear enamel hypoplasia. Ocular features such as chorioretinal coloboma of the left eye and nasolacrimal duct obstruction were noted. Other features such as undescended testis, syndactyly of left fingers, and lobster claw deformity [Figure 2] of the left foot were present. Dermoscopy revealed reticulate fine vessels along with ill-defined structureless white areas and loss of pigmentary network. Lentigo-like lesions in the hypopigmented atrophic areas were also seen [Figure 3]. Genetic analysis revealed hemizygous single base pair deletion in exon10 of the PORCN gene [c.885del (p.Arg296GlyfsTer18)]. The occurrence of focal dermal hypoplasia in a male may be explained by genetic mosaicism.1
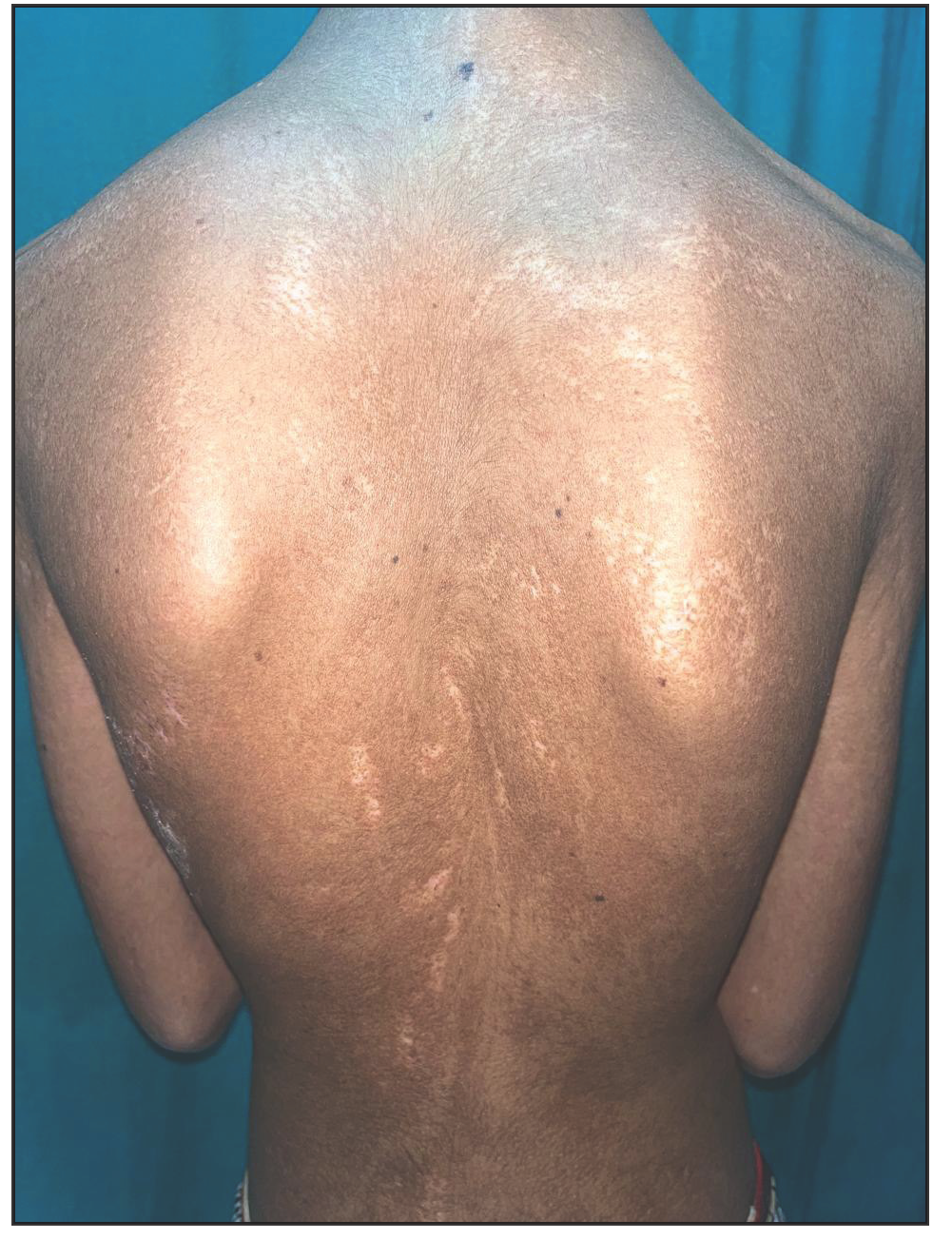
- Atrophic hypopigmented to depigmented plaques arranged along the lines of Blaschko over the back.

- Lobster claw deformity of the left foot.
![Dermoscopy reveals a shiny white structureless area with telangiectasia (black circle), along with structureless white area (blue arrow) and lentigo-like pigmentation (red arrow) [Dermlite DL4, 10x, polarised].](/content/126/2025/0/1/img/IJDVL_96_2024-g3.png)
- Dermoscopy reveals a shiny white structureless area with telangiectasia (black circle), along with structureless white area (blue arrow) and lentigo-like pigmentation (red arrow) [Dermlite DL4, 10x, polarised].
Another case was a 23-year-old female presented with hypopigmented atrophic skin lesions, distributed almost all over her body since birth. History of delayed developmental milestones in the gross motor, fine motor, and social and language skills were present. She was born out of a non-consanguineous marriage with a normal antenatal and perinatal history. On examination, pinkish to hypopigmented atrophic plaques were distributed along the Blaschko’s lines with few areas of fat herniations. Associated features such as syndactyly, exotropia, deviated nasal septum, diastema, and left mandibular cyst were present. The patient denied genetic analysis due to financial constraint. Based on clinical features, a diagnosis of focal dermal hypoplasia was made.
Focal dermal hypoplasia classically presents as Blaschko linear depigmented atrophic lesions with telangiectasias (95%), congenital hypo or hyperpigmentation (95%), and fat herniation (65%) which typically affects the trunk and extremities. Unlike incontinentia pigmenti, this syndrome does not have morphological variation in accordance with age.1 Linear enamel hypoplasia, hypodontia, jaw cysts, clefting, and hemihypoglossia are oral malformations. Papillomatosis appears on the mucosal, perigenital, intertriginous, and perioral surfaces. Patchy alopecia, brittle or scant hair, nail dystrophy or anonychia and palmar and plantar hyperkeratosis are other cutaneous features. Skeletal changes include syndactyly, polydactyly, oligodactyly, ectrodactyly, lobster claw deformity, and osteopathia striata (vertical banding of epiphysis and metaphysis of bones on radiography).1,2 Vertebral anomalies include scoliosis, kyphosis, vertebral body fusions, and spina bifida. Ocular anomalies comprise coloboma, strabismus, microphthalmia and nystagmus. Intellectual disability has been reported in 15%subjects. A minority may have defects in other organ systems, including auditory, cardiac, abdominal wall defects, malrotation of the gut, duodenal atresia, and renal malformations. Structural abnormalities of the kidneys and urinary system, such as hydronephrosis, fused or horseshoe kidneys, cystic renal dysplasia and hypoplastic kidney can result in recurrent urinary tract infections and urine reflux.2,3 Focal dermal hypoplasia has been linked to neurological symptoms such as myelomeningocele, Arnold-Chiari malformation, and hydrocephalus.3 The hair shafts may exhibit anomalies, such as atrophic hair with smaller diameters, flattened hair, trichorrhexis nodosa, pili torti and pili trianguli et canaliculi when examined under the scanning electron microscopy.4
Skin biopsies from the erythematous lesions reveal acanthosis and mild epidermal hyperkeratosis, with or without subepidermal clefts, and mild dermal eosinophilic infiltrates, whereas the basal cell layer is hyperpigmented and the epidermal atrophy is seen in atrophic lesions. Immediately below the epidermis, a wedge-shaped area of scar formation composed of fibroblasts and parallel bundles of hyaline collagen are described. Due to degeneration of dermal collagen fibres, the fatty tissue often reaches the epidermis resulting in heterotopic fat deposition.5
Genetic analysis reveals a mutation in the PORCN gene, which encodes for endoplasmic reticulum protein with O-acyltransferase activity, involved in the post-translational processing of the wingless-type mouse mammary tumour virus integration site (Wnt) protein, which is involved in meso-ectodermal tissue development. The hemizygous PORCN gene mutation [c.885del (p.Arg296GlyfsTer18)] at exon 10 present in our first case has not been reported in the 1000 genomes, gnomAD (v3.1), gnomdAD (v2.1) and TOPMed.6
To conclude, this case report highlights the unusual occurrence of a rare disease – Goltz syndrome – in males due to mosaicism.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of AI-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Focal dermal hypoplasia with a De novo mutation p.E300* of PORCN gene in a male infant. Indian J Dermatol. 2016;61:700.
- [CrossRef] [PubMed] [Google Scholar]
- Focal dermal hypoplasia (Goltz syndrome): A cross-sectional study from Eastern India. Indian J Dermatol. 2017;62:498-504.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Focal dermal hypoplasia: Report of a case with myelomeningocele, Arnold-Chiari malformation and hydrocephalus with a review of neurologic manifestations of Goltz syndrome. Pediatr Dermatol. 2014;31:220-4.
- [CrossRef] [PubMed] [Google Scholar]
- Dermatologic findings of focal dermal hypoplasia (Goltz syndrome) Am J Med Genet C Semin Med Genet. 2016;172C:44-51.
- [CrossRef] [PubMed] [Google Scholar]
- Multidisciplinary approach to Gorlin-Goltz syndrome: From diagnosis to surgical treatment of jawbones. Maxillofac Plast Reconstr Surg. 2022;44:25.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Focal dermal hypoplasia in a male patient due to mosaicism for a novel PORCN single nucleotide deletion. J Eur Acad Dermatol Venereol. 2011;25:592-5.
- [CrossRef] [PubMed] [Google Scholar]




