Translate this page into:
A novel mutation in LAMA3A gene in a child with laryngo-onycho-cutaneous syndrome from the Indian subcontinent
Correspondence Address:
PSS Ranugha
Department of Dermatology, JSS Medical College and Hospital, JSSAHER, Mysore, Karnataka
India
| How to cite this article: Ranugha P, Shastry V. A novel mutation in LAMA3A gene in a child with laryngo-onycho-cutaneous syndrome from the Indian subcontinent. Indian J Dermatol Venereol Leprol 2020;86:555-559 |
Sir,
Laryngo-onycho-cutaneous or Shabbir syndrome (OMIM 245660) is a rare autosomal recessive epithelial disorder confined to the Punjabi Muslim population.[1] Herein, we present a child with laryngo-onycho-cutaneous syndrome demonstrating a new mutation in LAMA3A gene.
A 2-year-old Bangladeshi girl, born out of non-consanguineous parentage, presented with a history of hoarse cry since birth and spontaneous blistering, automatic reddish growths from eyelids, wounds on the body and discoloration of nails since 6 months of age. On examination, we noted superficial erosions and ulcers with exuberant granulation tissue (ranging in size from 7× 4 to 15× 4 cm) on the right cheek, upper chest and left shoulder [Figure - 1]a. Multiple hyperpigmented to violaceous papules and plaques with central erosions and crusting were noted on the trunk and limbs [Figure - 1]b. We also observed fleshy growths from both upper eyelids without any bleeding, discharge or matting. Brownish discoloration of teeth was observed along with few dystrophic nails [Figure - 1]c and [Figure - 1]d. Ear, nose and throat referral was made and laryngoscopy revealed multiple tense bullae in the larynx [Figure - 1]e. There was no history of breathing difficulty. Parents denied any history of recurrent skin or respiratory infections or similar complaints in any family member. Developmental milestones were adequate for her age. Routine blood investigations and serum immunoglobulin levels were normal. Absence of hair or sweating abnormalities, icthyosis, palmoplantar keratoderma, photosensitivity and acantholysis on skin histopathology ruled out ectodermal dysplasias and other genodermatoses associated with blistering. Ultrasonogram of the abdomen revealed a fatty liver with borderline splenomegaly.
 |
We identified three different mutations in different exons of the LAMA3A gene on chromosome 18 by molecular analysis of the child's blood sample. A heterozygous two base pair deletion in exon 47 of the LAMA3 gene resulted in a frame shift and premature truncation of the protein, 5 amino acids downstream to codon 1967 (p. Ser1967GlnfsTer5; ENST00000313654) was detected [Figure - 2]. A heterozygous missense mutation was detected in exon 13 of the LAMA3 gene (chr18:21390398C>T; depth: 164×), which led to substitution of amino acid tryptophan for arginine at codon 558 (p. Arg558Trp; ENST00000313654). This observed variation lies in the lamin in epidermal growth factor domain of the LAMA3 protein. Another heterozygous missense variation in exon 28 of the LAMA3 gene (chr18:21422480G>A; depth: 74×) was found which resulted in amino acid substitution of glutamine for arginine at codon 1153 (p. Arg1153Gln; ENST00000313654).
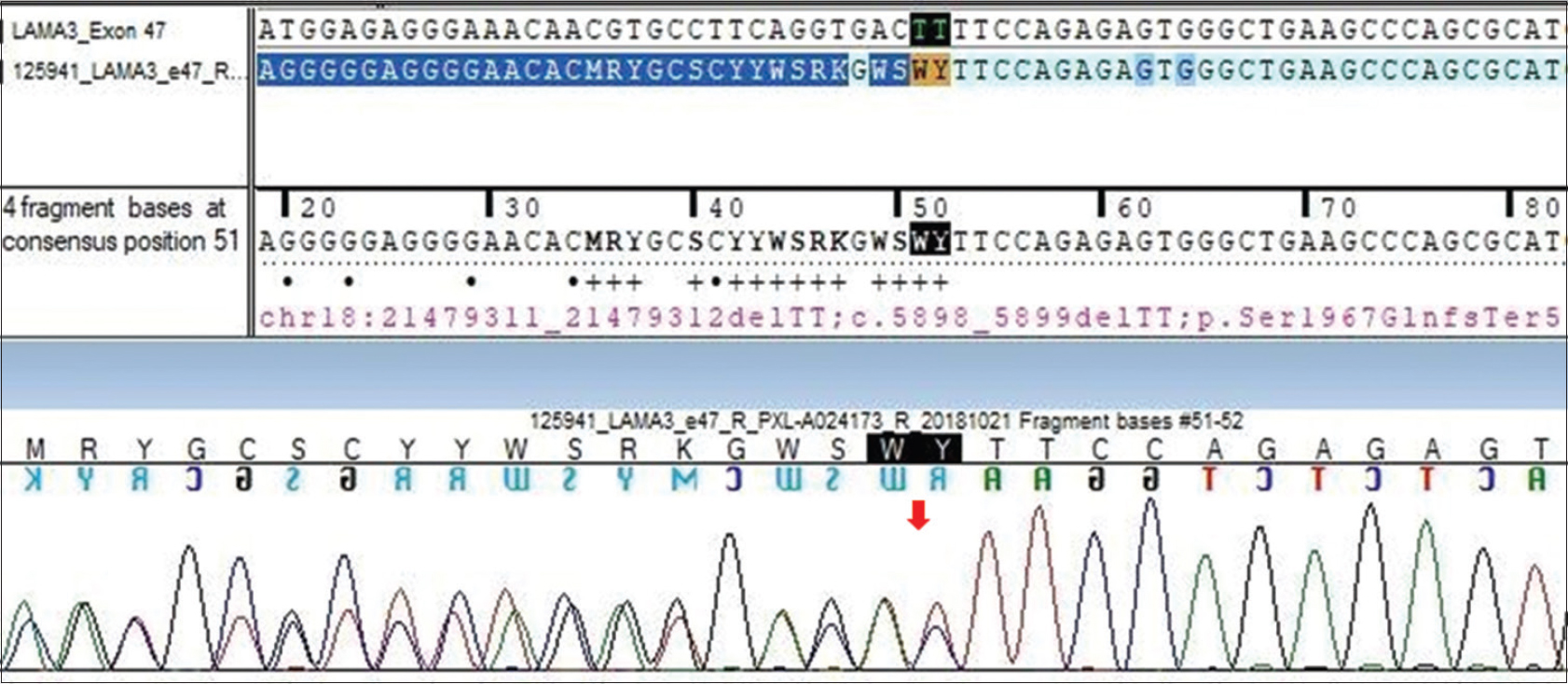 |
| Figure 2: Sequence chromatogram and alignment to the reference sequence showing the variation in exon 47 of the LAMA3 gene (chr18:21479311_21479312delTT; c.5898_5899delTT; p. Ser1967GlnfsTer5) detected in heterozygous condition |
Based on clinical findings and mutations in the LAMA3A gene, we made a diagnosis of laryngo-onycho-cutaneous syndrome. We advised daily dressing of the wounds, topical steroids and antihistamines. Parents were taught about wound care and ophthalmologic intervention was sought for excision of conjunctival granulation tissue and amniotic membrane transplant. The child expired after 6 months following respiratory distress.
Laryngo-onycho-cutaneous syndrome is a localized variant of junctional epidermolysis bullosa. It starts in infancy with chronic erosions affecting the face (predominantly perinasal and perioral). The nails are involved with marked periungual and subungual inflammation. Hoarseness is a universal feature characterized by altered cry at birth. The teeth may be notched. Exuberant skin and mucosal granulation tissue formation can impair wound healing and result in laryngeal obstruction and blindness.[2] Although these findings are common to all types of junctional epidermolysis bullosa, the erosions and bullae are much extensive in generalized junctional epidermolysis bullosa whereas minimal blistering with excessive granulation tissue formation is characteristic of laryngo-onycho-cutaneous syndrome. Conjunctival eye lesions, characteristic of laryngo-onycho-cutaneous syndrome, are rare in other subtypes of junctional epidermolysis bullosa.[1]
The laminins are a family of heterotrimeric molecules, responsible for structural and functional integrity of basement membrane. Through the study of blistering skin diseases, it is now well-established that the a3 subunit of laminins-332, -321 and -311 plays an important role in mediating epidermal-dermal integrity and is essential for the skin to withstand mechanical stress.[3] Most mutations in both Herlitz and non-Herlitz forms of junctional epidermolysis bullosa disease are restricted to three genes, LAMA3, LAMB3 and LAMC2, that encode the α, β and γ subunits of laminin 332, respectively.[4]
The human LAMA3 gene encodes 76 exons from 318 kb of genomic DNA at chromosomal location 18q11.2 and has two transcripts LAMA3A and LAMA3B (B1 and B2).[3]In most laryngo-onycho-cutaneous cases of Punjabi origin, a homozygous recessive mutation has been detected in exon 39 of LAMA3A which encodes laminin 3A leading to the fore-shortening of a critical portion of the N terminus of the a3 chain of laminin-5 trimer.[3] Studies suggest altered homeostasis of extracellular matrix due to secretion of abbreviated a3 chain by the basal keratinocytes.[5],[6]
In our patient, we detected a novel heterozygous 2-base pair deletion in exon 47, not reported till date, leading to premature truncation of protein, which could be the possible pathogenic mutation. Absence of the N-terminal region of laminin alpha 3a in laryngo-onchyo-cutaneous syndrome results in excessive granulation tissue production at wound sites.[5]
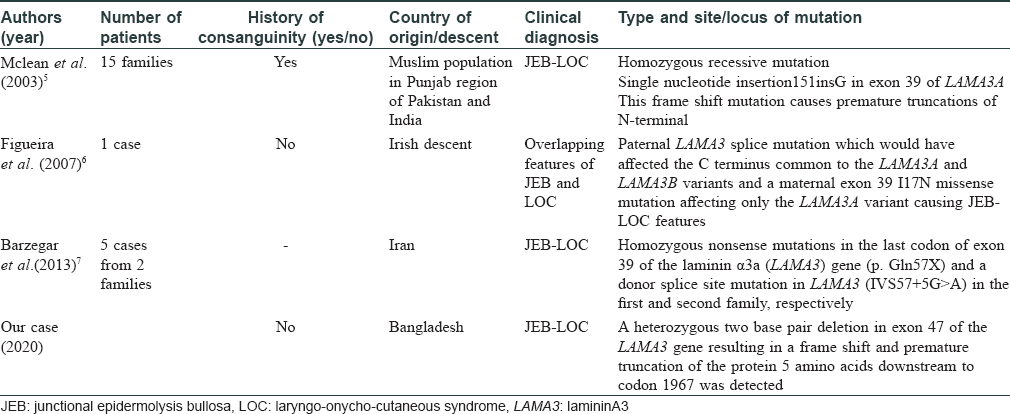
We also found heterozygous missense mutations in exon 13 and exon 28, however, further studies are needed to highlight its significance. The different mutations reported in laryngo-onycho-cutaneous syndrome till date are described in [Table - 1].[5],[6],[7]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the legal guardian has given his consent for images and other clinical information to be reported in the journal. The guardian understands that names and initials will not be published and due efforts will be made to conceal the identity but anonymity cannot be guaranteed.
Acknowledgments
We would like to thank Dr. Ravi N. Hiremagalore for helping us with the evaluation of the case.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Cohn HI, Murrell DF. Laryngo-onycho-cutaneous syndrome. Dermatol Clin 2010;28:89-92.
[Google Scholar]
|
| 2. |
McGrath JA. Genetic blistering diseases. In: Chalmers R, Barker J, Griffiths C, Bleiker T, Creamer D, editors. ROOK's Textbook of Dermatology. 9th ed. West Sussex, UK: John Wiley and Sons, Ltd.; 2016. p. 71.14.
[Google Scholar]
|
| 3. |
Hamill KJ, Paller AS, Jones JC. Adhesion and migration, the diverse functions of the laminin alpha3 subunit. Dermatol Clin 2010;28:79-87.
[Google Scholar]
|
| 4. |
Varki R, Sadowski S, Pfendner E, Uitto J. Epidermolysis bullosa. I. Molecular genetics of the junctional and hemidesmosomal variants.J Med Genet 2006;43:641-52.
[Google Scholar]
|
| 5. |
McLean WH, Irvine AD, Hamill KJ, Whittock NV, Coleman-Campbell CM, Mellerio JE, et al. An unusual N-terminal deletion of the laminin alpha3a isoform leads to the chronic granulation tissue disorder laryngo-onycho-cutaneous syndrome. Hum Mol Genet 2003;12:2395-409.
[Google Scholar]
|
| 6. |
Figueira EC, Crotty A, Challinor CJ, Coroneo MT, Murrell DF. Granulation tissue in the eyelid margin and conjunctiva in junctional epidermolysis bullosa with features oflaryngo-onycho-cutaneous syndrome. Clin Exp Ophthalmol 2007;35:163-6.
[Google Scholar]
|
| 7. |
Barzegar M, Mozafari N, Kariminejad A, Asadikani Z, Ozoemena L, McGrath JA. A new homozygous nonsense mutation in LAMA3A underlying laryngo-onycho-cutaneous syndrome. Br J Dermatol. 2013 Dec;169(6):1353-6.
[Google Scholar]
|
Fulltext Views
3,138
PDF downloads
1,607





![[Figure - 1]](#fig_ijdvl_2020_86_5_555_290498_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_5_555_290498_f2.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2020_86_5_555_290498_t3.jpg){kind=link}