Translate this page into:
Asymptomatic swelling on the great toe in a 13-year-old boy
2 Postgraduate Department of Orthopaedics, Government Medical College, University of Kashmir, Srinagar, Jammu and Kashmir, India
3 Postgraduate Department of Pathology, Government Medical College, University of Kashmir, Srinagar, Jammu and Kashmir, India
Correspondence Address:
Yasmeen Jabeen Bhat
Postgraduate Department of Dermatology, STD and Leprosy, Government Medical College, University of Kashmir, Srinagar - 190010, Jammu and Kashmir
India
| How to cite this article: Bhat YJ, Baba AN, Shah FY, Wani R, Mir MA. Asymptomatic swelling on the great toe in a 13-year-old boy. Indian J Dermatol Venereol Leprol 2020;86:597-599 |
A 13-year-old boy presented with a swelling on the dorsum of distal phalanx of the great toe of the right foot, encroaching the nail bed. The swelling had been present for about 6 months and there was a history of trauma preceding the onset of the lesion. The lesion had increased in size for the first 3 months, but thereafter the size remained the same. The lesion was asymptomatic without any pain or swelling of the adjacent tissue. The mass was about 7 mm in diameter. It was non-tender and firm to hard on palpation [Figure - 1].
 |
| Figure 1: Firm yellowish swelling on right great toe |
Dermoscopy revealed non-vascular nature of the lesion and white spots were noted, indicating scarring [Figure - 2]. Laboratory investigations were normal. X-ray in the anteroposterior and lateral view of the foot revealed a sclerotic lesion with an irregular border with density similar to the adjacent bone. The sclerotic shadow could be seen as a distinct mass separate from the underlying bone [Figure - 3]. An excision biopsy was performed by the consulting orthopedician. Histopathological examination revealed hyperkeratotic and acanthotic lining epidermis and the presence of fibrous tissue among islands of osteoid tissue and osteoblasts. The underlying tissue was constituted by bony trabeculae and chondroid tissue embedded in a hyalinized fibrocollagenous stroma [Figure - 4].
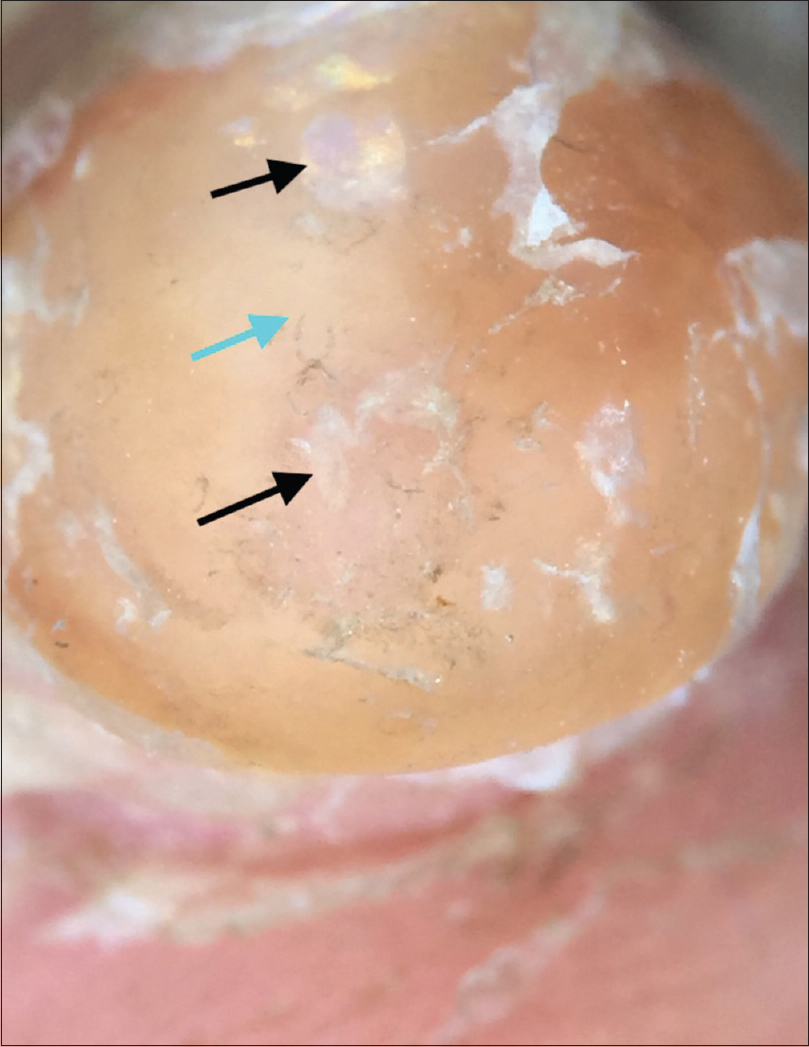 |
| Figure 2: Dermoscopy showing scales, yellowish structureless areas (blue arrow) and white (black arrows) spots [Dermlite DL3N (×10)] |
 |
| Figure 3: X-ray (lateral view) of the affected foot showing sclerotic lesion, separate from the bone (blue arrow) |
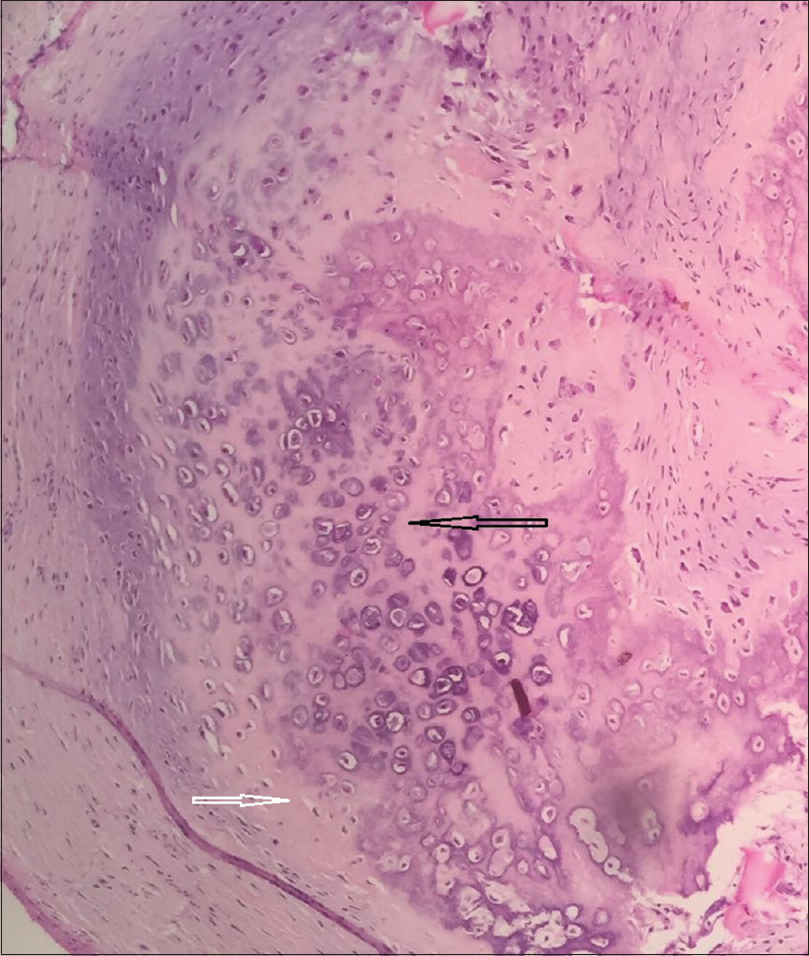 |
| Figure 4: Cellular stroma with cartilage and bone formation in the center (black arrow) and cartilaginous tissue in a mucinous matrix (white arrow) (H and E, ×400) |
What Is the Diagnosis?
Diagnosis
Fibro-osseous pseudotumor of the digit.
Review
Fibro-osseous pseudotumor of the digit is a rare benign soft tissue lesion which occurs as a result of focal calcification and is commonly seen in the region of proximal phalanx, metacarpal, and metatarsal regions.[1] It occurs predominantly in adolescents and young adults and consists of foci of osseous differentiation with fibroblastic proliferation.[2] The lesion is benign, and recurrence following local excision is unusual.[3] It needs to be differentiated from other disorders such as myositis ossificans, turret exostosis and extraskeletal osteosarcoma which pose a diagnostic dilemma. Fibro-osseous pseudotumor has clinical and histological semblance with myositis ossificans. However, superficial occurrence of fibro-osseous pseudotumor involving mainly the subcutaneous tissue without muscular involvement helps differentiate it from myositis ossificans which usually occurs in deeper soft tissues and also exhibits a characteristic zoning pattern on histopathology. A superficial lesion, lacking a zoning pattern, is more in line with a diagnosis of fibro-osseous pseudotumor.[4],[5] The zoning pattern refers to the characteristic zonal organization on histopathology with a peripheral zone of well-organized mature lamellar bone, intermediate osteoid region, and immature nonossified fibroblastic central zone.
Extraskeletal osteosarcoma can usually be differentiated by its late occurrence, affecting people of older age groups and development in the large proximal muscle groups of lower extremity. Fibro-osseous pseudotumor, on the other hand, is commonly found in young adults and is typically located more distally.[6]
The clinical, histological, and radiological findings in turret exostosis are similar to those of fibro-osseous pseudotumor. A distinction between the two conditions can be made on the grounds of attachment to the underlying bone and enchondral ossification in case of turret exostosis.[5],[7] Fibro-osseous pseudotumor, on the other hand, is an extraosseous lesion.
Clinically, the lesion presents as a painful, localized swelling in the soft tissue of the digits, but may be painless at times. A history of preceding trauma is frequently present, but not always. X-ray of the affected area reveals soft tissue swelling with focal calcification, which lacks the typical zoning pattern seen in myositis ossificans.[8] Wide block excision or ray amputation was recommended earlier, but recent reports suggest excellent prognosis following local excision with no tendency for recurrence (0%–0.14%).[3],[9]
Limitations
Computed tomography scan was not done in our patient. This investigation is helpful in confusing cases and can help in differentiation of fibro-osseous pseudotumor from other mimicking disorders such as myositis ossificans and osteosarcoma.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient's parents have given his consent for his images and other clinical information to be reported in the journal. The patient's parents understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Javdan M, Tahririan MA. Fibro-osseous pseudotumor of the digit. Adv Biomed Res 2012;1:31.
[Google Scholar]
|
| 2. |
Tang JB, Gu YQ, Xia RG. Fibro-osseous pseudotumor that may be mistaken for a malignant tumor in the hand: A case report and review of the literature. J Hand Surg Am 1996;21:714-6.
[Google Scholar]
|
| 3. |
Singal A, Gogoi P, Pandhi D, Bhatt S. Subungual fibro-osseous pseudotumour of the digit: A rare occurrence. Int J Dermatol 2017;56:e11-3.
[Google Scholar]
|
| 4. |
Hashmi AA, Faridi N, Edhi MM, Jafri A, Khan M. Fibro-osseous pseudotumor of the digit presenting as an ulcerated lesion: A case report. Int Arch Med 2014;7:4.
[Google Scholar]
|
| 5. |
Moosavi CA, Al-Nahar LA, Murphey MD, Fanburg-Smith JC. Fibroosseous [corrected] pseudotumor of the digit: A clinicopathologic study of 43 new cases. Ann Diagn Pathol 2008;12:21-8.
[Google Scholar]
|
| 6. |
Kwak M, Kim S, Lee S, Jun S, Lee A. Radiological features of a fibro-osseous pseudotumor in the digit: A case report. J Korean Soc Radiol 2015;73:131.
[Google Scholar]
|
| 7. |
Calisir C, Kocman AE, Oztunali C, Arik D, Uzuner M, Cetin C, et al. Imaging findings of an extradigital fibro-osseous pseudotumor. Jpn J Radiol 2014;32:613-7.
[Google Scholar]
|
| 8. |
Dupree WB, Enzinger FM. Fibro-osseous pseudotumor of the digits. Cancer 1986;58:2103-9.
[Google Scholar]
|
| 9. |
McCarthy EF, Ireland DC, Sprague BL, Bonfiglio M. Parosteal (nodular) fasciitis of the hand. A case report. J Bone Joint Surg Am 1976;58:714-6.
[Google Scholar]
|
Fulltext Views
3,308
PDF downloads
1,907





![[Figure - 1]](#fig_ijdvl_2020_86_5_597_262693_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_5_597_262693_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_5_597_262693_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2020_86_5_597_262693_f4.jpg){kind=link}