Translate this page into:
Localized unilateral basaloid follicular hamartoma along Blaschko's lines on face
2 Consultant Dermatologist, Sakhiya Skin Clinic, Surat, Gujarat, India
Correspondence Address:
Sarina Jain
Department of Dermatology, Main Hospital Building, Ward 17-18, Ground Floor, KEM Hospital, Parel, Mumbai - 400 012, Maharashtra
India
| How to cite this article: Jain S, Khopkar U, Sakhiya J. Localized unilateral basaloid follicular hamartoma along Blaschko's lines on face. Indian J Dermatol Venereol Leprol 2019;85:60-64 |
Abstract
Basaloid follicular hamartoma (BFH) is a rare hamartoma of hair follicle. Clinical presentations may vary but are united by the same histopathological features in the form of folliculocentric basaloid or squamoid cell proliferation in the superficial dermis, which represents malformed and distorted hair follicles. It is important to recognize this entity as its simulant is basal cell carcinoma, a low-grade malignancy. Here, we report a case of localized unilateral BFH in a Blaschkoid distribution on the face of a 14-year-old female.
Introduction
Basaloid follicular hamartoma (BFH) is a rare hamartoma with hair follicle elements and characteristic histopathological features that may simulate basal cell carcinoma (BCC). It may present as solitary or multiple papules or plaques in a generalized or localized distribution. Here, we report a case of localized unilateral BFH along the lines of Blaschko on the face of a 14-year-old female.
Case Report
A 14-year-old female presented with an asymptomatic lesion on the left side of her face since early childhood. The lesion began as two small papules on the left cheek at the age of 2 years spontaneously without any prior trauma and gradually progressed over 12 years to reach the present size. There was no history of similar lesions in the family. The patient was otherwise healthy, with no relevant medical history.
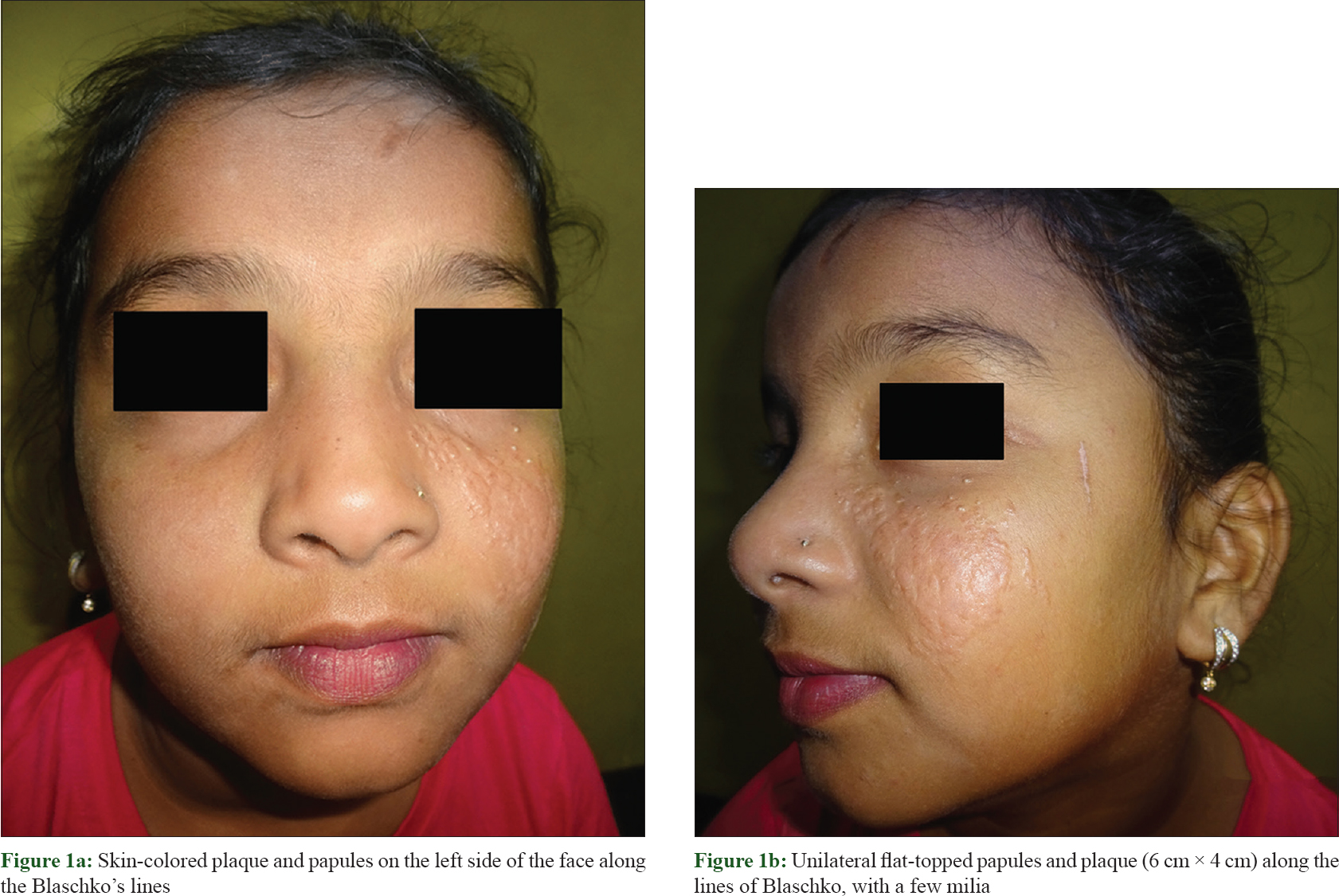
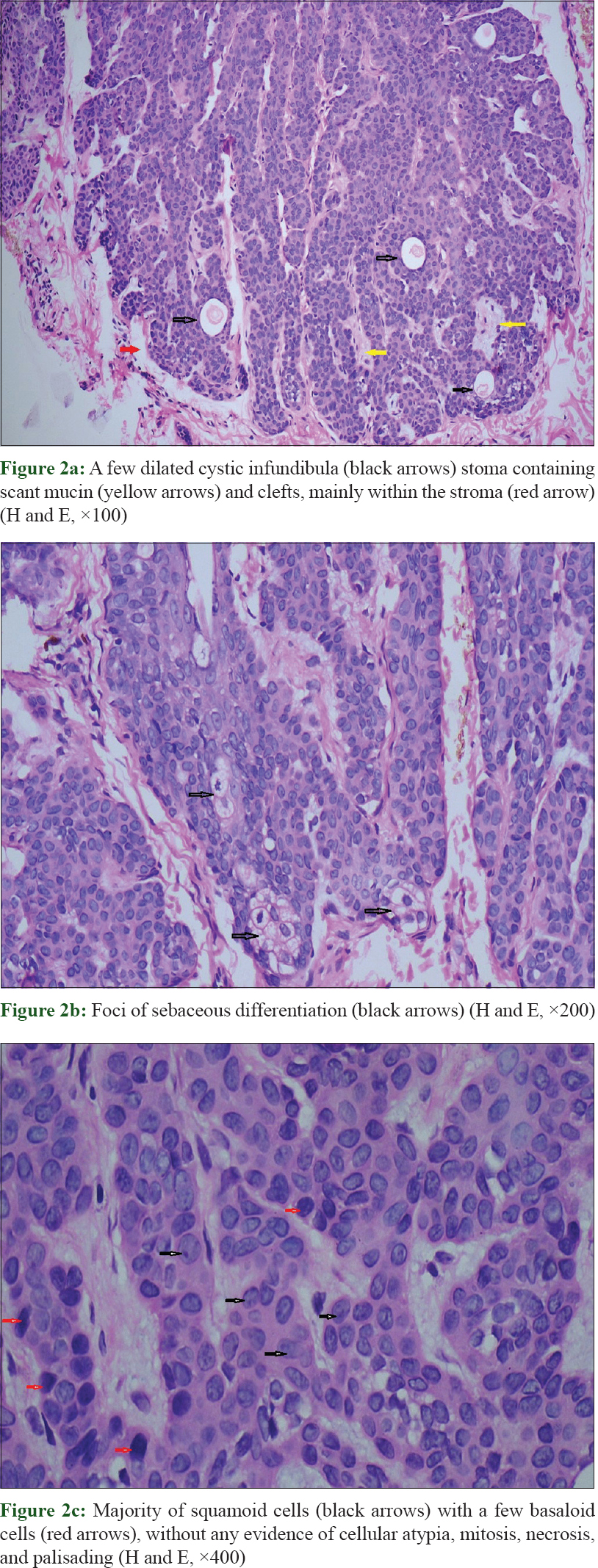
On examination, multiple skin-colored, flat-topped papules, coalescing to form an oval plaque of size 6 cm × 4 cm, along with few milia were seen on the left side of the cheek. The lesion extended from the mid of left cheek to the medial aspect of the left upper eyelid following the lines of Blaschko. The right side of her face was completely spared [Figure - 1]a and [Figure - 1]b. No other body parts were involved. Our clinical differential diagnoses were nevus sebaceous, collagen nevus, multiple trichoepitheliomas along Blaschko's lines, and unilateral nevoid BCC syndrome. Skin biopsy showed a well-demarcated epithelial proliferation in the upper dermis composed of squamoid and basaloid cells that formed branching cords and strands, most of which were seen connected with the overlying epithelium. Each tumor island was associated with a malformed vellus follicle located beneath it. A few dilated cystic infundibula and foci of sebaceous differentiation were seen inside these proliferations [Figure - 2]a and [Figure - 2]b. Majority cells were squamoid cells along with a few scattered basaloid cells at the periphery of proliferations. Peripheral palisading, mitotic figures, necrotic tumor cells, and cytological atypia were absent [Figure - 2]c. Surrounding stroma was scant, mildly fibrocellular, and contained scant mucin. There was virtually no inflammatory cell infiltrate. Clefts were seen to be present mainly within the stroma, with minimal clefting at the borders between the tumor islands and the surrounding stroma [Figure - 2]a. The overlying epidermis was atrophic but intact.
 |
| Figure 1 |
 |
| Figure 2 |
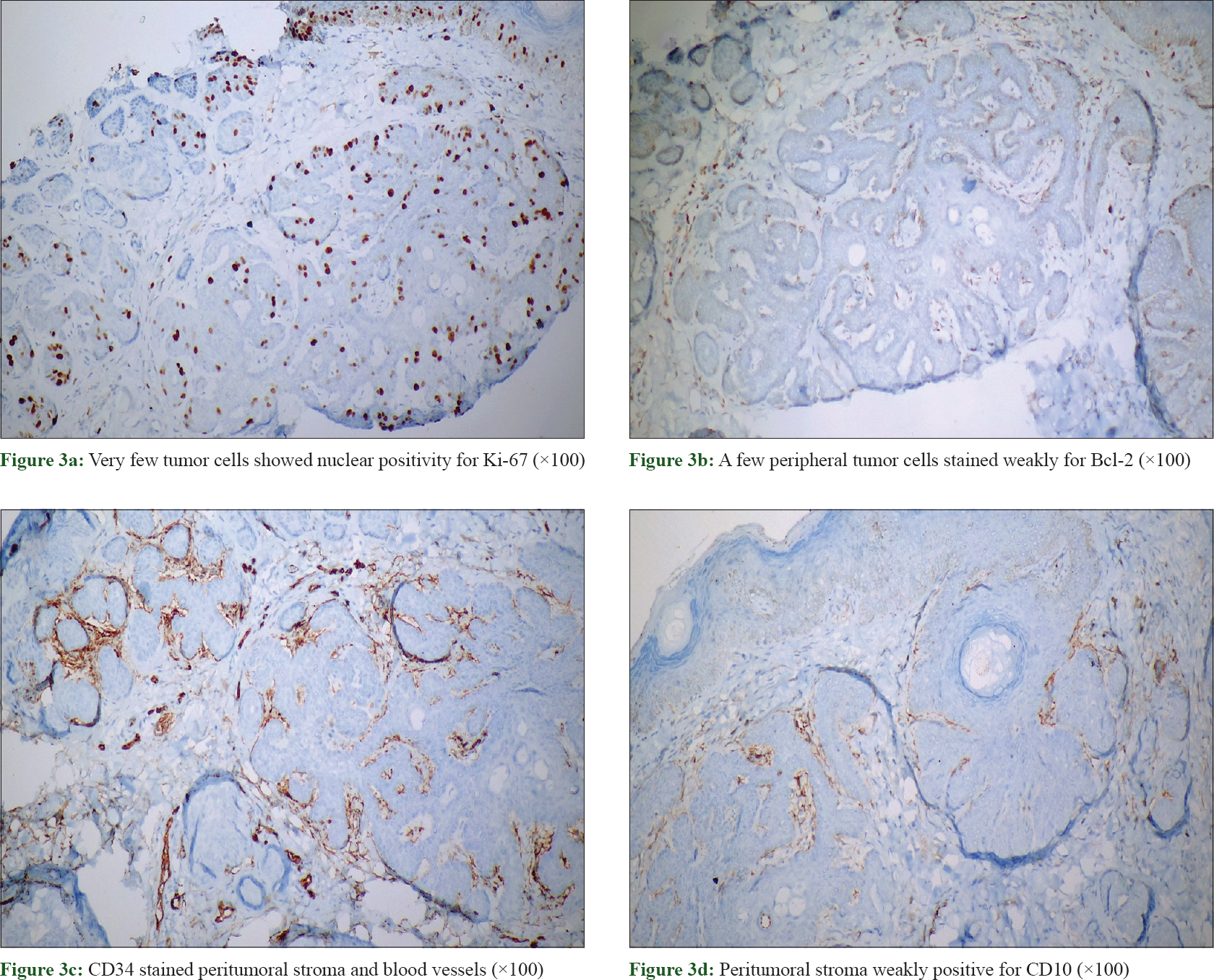
Upon immunohistochemical staining, tumor cells expressed AE1/AE3 (keratin). Ki-67 index was only 10% [Figure - 3]a. A few peripheral tumor cells bordering the stroma stained weakly for Bcl-2 [Figure - 3]b. The stroma showed strong CD34 positivity and weak CD10 positivity [Figure - 3]c and [Figure - 3]d.
 |
| Figure 3 |
Based on the clinical, histopathological, and immunohistochemical findings, we diagnosed our patient as a case of localized unilateral BFH present along the Blashcko's lines on the face. We counseled her regarding the benign nature of the disease and advised her for periodic follow-up.
Discussion
BFH is a rare cutaneous hamartoma showing follicular elements first described by Brown et al. in 1969. The term “basaloid follicular hamartoma” was coined by Mehregan and Baker in 1985 who described localized and solitary types of lesions without associated systemic involvement.[1]
Five clinical variants of BFH include solitary or multiple papules; a localized plaque with alopecia; a localized linear or unilateral papule or plaque; a generalized variant dominantly inherited familial type without associated disorders; and generalized papules associated with alopecia and myasthenia gravis.[2] Individual lesions are small, skin-colored to brown papules, nodules or plaques, with or without associated milia and/or comedones, commonly present over the face, scalp, and occasionally, the trunk.[1]
The localized linear or unilateral type may present at birth or may appear later in childhood or second decade of life. It commonly follows lines of Blaschko. Early lesions may show hypopigmented, smooth or striae-like areas, with or without comedones. Later, small skin-colored, pale or brown-colored papules and plaques may develop.[3] This type has been described with different names such as “linear unilateral basal cell nevus with comedones,” “linear unilateral basal cell nevus,” “linear unilateral basaloid follicular hamartoma,” and “basal-cell and linear unilateral adnexal hamartoma.”[4]
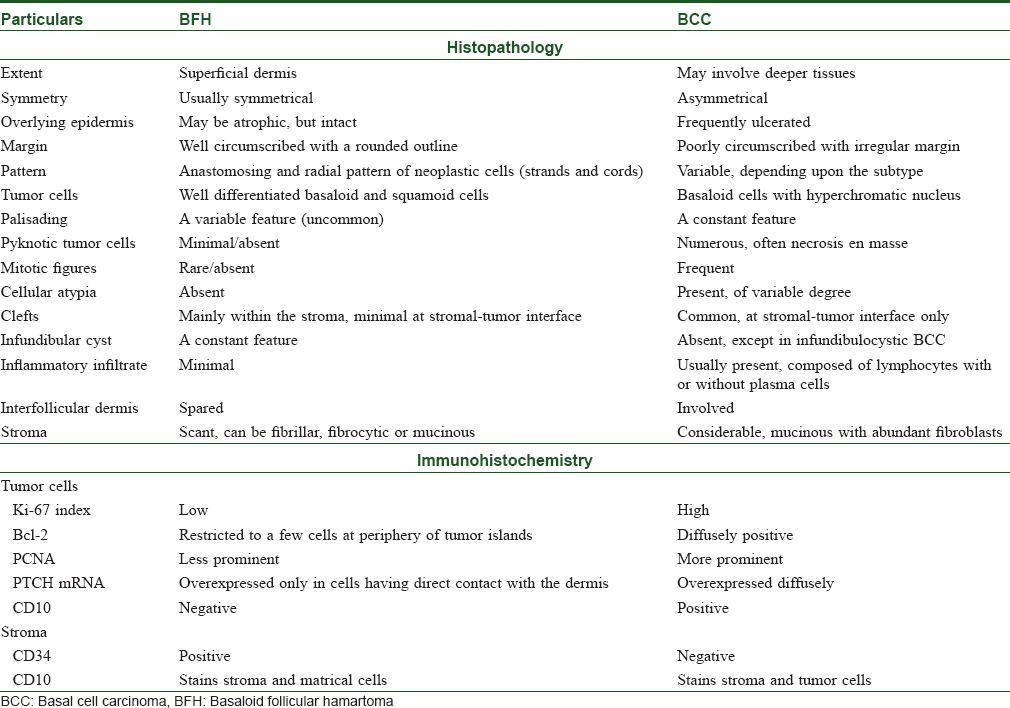
Histopathological differential diagnosis of BFH includes BCC and trichoepithelioma. The key histopathological and immunohistochemical differences between BFH and BCC are summarized in [Table - 1].[1],[2] Trichoepithelioma is a benign neoplasm of germinative follicular cells. It is differentiated from BFH by the presence of follicular differentiation in the form of germs and papillae; abundant and highly fibrocytic stroma; palisading; and predominance of basaloid cells.[2]
Infundibulocystic BCC (ICBCC) is a rare variant of BCC that was described by Walsch and Ackerman in 1990 that is histopathologically similar to BFH.[2] In contrast to the BFH, ICBCC is a low-grade malignancy composed of neoplastic cell proliferation that involve and destroy pre-existing follicles as well as the interfollicular dermis.[1] Though it is usually confined to the upper dermis, it may sometimes involve deeper tissues. It can also be differentiated from BFH by the presence of palisading, mitotic figures, necrotic neoplastic cells arranged as solitary units or in clusters and possible continuity with the nodular BCC.
The premalignant potential of BFH is currently uncertain, although BCC arising within BFH has been documented. Out of the 100 cases of BFH reported till date, 10 cases showing transition to BCC have been documented.[1],[2],[3],[4],[5],[6],[7],[8],[9],[10] Out of these 10 cases, 8 cases were of localized linear or unilateral variant of BFH.[3],[4],[5],[6],[7],[8],[9],[10] Rapid change in size or appearance of lesions of BFH may indicate development of BCC.
BFH per se is a benign condition which needs to be distinguished from BCC to avoid any aggressive surgical treatment. It remains stable for years and thus immediate surgical treatment is not required, and it can be periodically monitored to detect any malignant transformation. Treatment of BFH is opted by patients for cosmetic reasons. Treatment options include surgical excision, cryosurgery, laser surgery, and photodynamic therapy for diffuse or extensive lesions.[1]
Here, we report a case of localized unilateral BFH along the Blashcko's lines on the face of a young female child. Though BFH is a benign condition in itself, since instances of development of BCC in BFH are known, our patient requires long-term follow-up.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Gumaste P, Ortiz AE, Patel A, Baron J, Harris R, Barr R, et al. Generalized basaloid follicular hamartoma syndrome: A case report and review of the literature. Am J Dermatopathol 2015;37:e37-40.
[Google Scholar]
|
| 2. |
Saxena A, Shapiro M, Kasper DA, Fitzpatrick JE, Mellette JR Jr. Basaloid follicular hamartoma: A cautionary tale and review of the literature. Dermatol Surg 2007;33:1130-5.
[Google Scholar]
|
| 3. |
Jiménez-Acosta FJ, Redondo E, Baez O, Hernandez B. Linear unilateral basaloid follicular hamartoma. J Am Acad Dermatol 1992;27:316-9.
[Google Scholar]
|
| 4. |
Yébenes M, Toll A, Vélez M, Barranco C, Alonso-López NA, Gonzalez-Sarmiento R, et al. Linear unilateral hamartomatous basal cell naevus with glandular and follicular differentiation. Clin Exp Dermatol 2008;33:429-32.
[Google Scholar]
|
| 5. |
Yoshida Y, Urabe K, Mashino T, Duan H, Kiryu H, Masuda T, et al. Basal cell carcinomas in association with basaloid follicular hamartoma. Dermatology 2003;207:57-60.
[Google Scholar]
|
| 6. |
Nelson BR, Johnson TM, Waldinger T, Gillard M, Lowe L. Basaloid follicular hamartoma: A histologic diagnosis with diverse clinical presentations. Arch Dermatol 1993;129:915-7.
[Google Scholar]
|
| 7. |
Carney RG. Linear unilateral basal-cell nevus with comedones; report of a case. AMA Arch Derm Syphilol 1952;65:471-6.
[Google Scholar]
|
| 8. |
Bleiberg J, Brodkin RH. Linear unilateral basal cell nevus with comedones. Arch Dermatol 1969;100:187-90.
[Google Scholar]
|
| 9. |
Anderson TE, Best PV. Linear basal-cell naevus. Br J Dermatol 1962;74:20-3.
[Google Scholar]
|
| 10. |
Choi SW, Ryu YS, Kim HO, Kim CW. A case of basaloid follicular hamartoma combined with basal cell epithelioma. Korean J Dermatol 1998;36:148-51.
[Google Scholar]
|
Fulltext Views
3,996
PDF downloads
2,611





![[Figure - 1]](#fig_ijdvl_2019_85_1_60_226512_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_1_60_226512_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2019_85_1_60_226512_f3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2019_85_1_60_226512_t4.jpg){kind=link}