Translate this page into:
Urticaria pigmentosa in monochorionic twins
2 Department of Pathology, Faculty of Medicine, Van Yuzuncu Yil University, Van, Turkey
Correspondence Address:
Serap Gunes Bilgili
Department of Dermatology, Faculty of Medicine, Van Yuzuncu Yil University, Van
Turkey
| How to cite this article: Yavuz GO, Yavuz IH, Bilgili SG, Erten R, Savas H, Bayram I. Urticaria pigmentosa in monochorionic twins. Indian J Dermatol Venereol Leprol 2019;85:509-511 |
Sir,
Mastocytosis is a rare clonal disease of the hematopoietic stem cells characterized by accumulation and proliferation of mast cells.[1] The disease manifests itself either as cutaneous mastocytosis affecting only the skin, or as systemic mastocytosis affecting multiple organs.[2] The abnormal accumulation of mast cells is mostly seen on the skin. The World Health Organization currently recognizes three main subforms of cutaneous mastocytosis: maculopapular cutaneous mastocytosis = urticaria pigmentosa, diffuse cutaneous mastocytosis and the mastocytoma of skin.[3],[4] According to the EU/US consensus group, maculopapular cutaneous mastocytosis can be divided into two variants: monomorphic maculopapular cutaneous mastocytosis and polymorphic maculopapular cutaneous mastocytosis.[5]
Familial cutaneous mastocytosis is rare and about 100 familial cases were reported until 2018, of which, at least 10 were monozygotic twins.[6],[7]
A pair of ten-month-old female monochorionic twins were admitted to our clinic (Department of Dermatology, Van Yuzuncu Yil University, Faculty of Medicine, Van, Turkey) with skin eruptions seen predominantly on the trunk, face and extremities. Their history revealed that the skin eruptions were present at birth and were given no treatment. No itching, flushing, diarrhea or syncope was reported.
Dermatological examination of the twins revealed yellow-tan, reddish-brown plaques on the extremities and bullae overlying some of the plaques [Figure - 1]. Although Darier's sign was positive in both infants, they showed no signs of hepatosplenomegaly, lymphadenopathy or edema. Skin biopsy revealed a diffuse infiltrate of mast cells in the upper dermis with hematoxylin–eosin stain. CD117 staining was positive and toluidine blue stain confirmed the diagnosis [Figure - 2], [Figure - 3], [Figure - 4]. The patients were referred to the pediatric out-patient clinic for looking into systemic involvement.
 |
| Figure 1: Patients aged 10 months showing lesions of cutaneous mastocytosis |
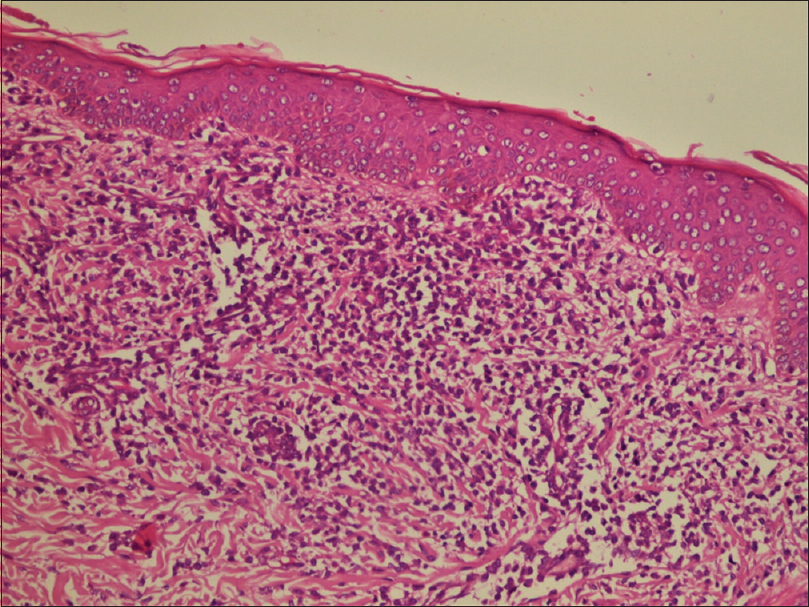 |
| Figure 2: Dense mast cell infiltration in the upper dermis (hematoxylin and eosin, ×200) |
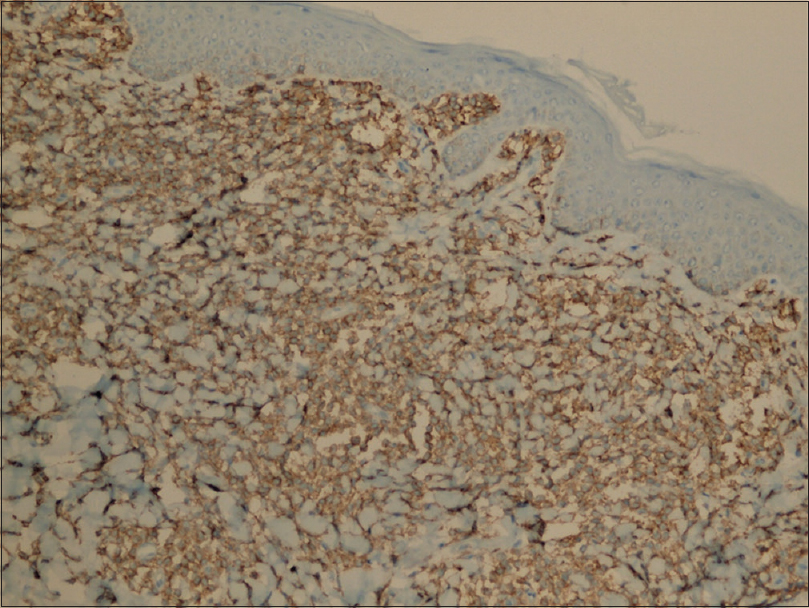 |
| Figure 3: Mast cells were stained with CD117 (CD117 × 200) |
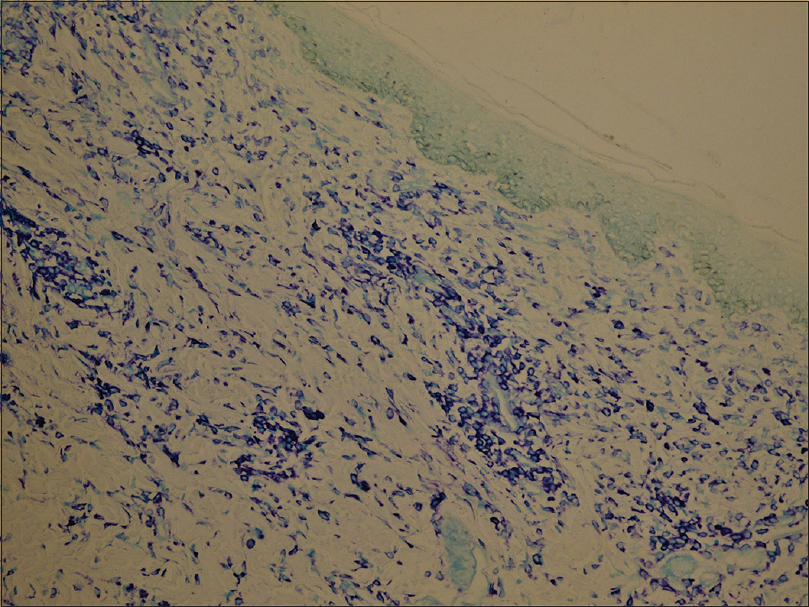 |
| Figure 4: Mast cells were stained with toluidine blue (toluidine blue × 200) |
A complete blood cell count and biochemical profiles were within normal limits. For systemic involvement, abdominopelvic ultrasonography, trans-fontanel ultrasonography, chest radiography and cerebral magnetic resonance imaging were performed; all revealed normal findings. Patients were diagnosed as urticaria pigmentosa based on the clinical and histopathological findings. The patients were not started on any medications as they had only skin findings; however, they were placed on regular follow-up.
Mastocytosis, a disease characterized by clonal proliferation of mast cells in one or multiple organs, may lead to various clinical manifestations. Mastocytosis is defined in two main forms: cutaneous mastocytosis (involvement of skin alone) and systemic mastocytosis with involvement of the organs such as the liver, spleen and/or bone marrow.[2],[3],[6]
Cutaneous mastocytosis is a very rare disease that usually occurs sporadically. The prevalence of the cutaneous form has been reported with variations. Kiszewski et al. reported a prevalence of 1 in 500.[1] Familial cutaneous mastocytosis is rare and about 100 familial cases were reported until 2018, at least 10 of these cases were monozygotic twins.[4],[7] Urticaria pigmentosa, the most common form of cutaneous mastocytosis, also known as maculopapular cutaneous mastocytosis, is mainly seen in children. The lesions may be present at birth and often develop from early infancy to the age of two. Ben-Amitai et al. have demonstrated that the lesions of urticaria pigmentosa are present at birth in 20% of the pediatric cases of cutaneous mastocytosis and the majority of the lesions usually develop during the first year of life.[2] In our case, the lesions were congenital.
The typical presentation of urticaria pigmentosa is with yellow-tan to reddish-brown macules or slightly raised papules scattered mainly on the trunk and legs with generally less involvement of the sun-exposed areas. The disease generally spreads to palms, soles, face and scalp, especially in adults. Dermatologic symptoms are pruritus, “flushing” and “bullae.” Bullae formation is almost uniquely seen in children.[2],[6] In our case, yellow-tan to reddish-brown plaques on face, trunk and extremities and some bullae were noted in both of the twins. Erythema and urticarial wheals induced by physical trauma (e.g., rubbing, friction) is known as Darier's sign,[8] which was positive in our case.
Since the course of the disease is benign, the main objective of the therapy is to reduce the release of mast cell mediators and to inhibit their effects, thereby controlling signs and symptoms. Patients with urticaria pigmentosa and the families should be informed that they should avoid hot baths, sudden temperature changes, physical stimulants, vigorous rubbing of the skin, anxiety and drugs including aspirin, codeine, opiates, alcohol and radiocontrast substances containing iodide, to prevent exacerbations.[4],[8]
Childhood cases of urticaria pigmentosa have a good prognosis; systemic involvement is rare and usually spontaneously resolves until puberty.[4] In our case, physical examination, laboratory and radiological examinations showed no evidence of systemic involvement.
Finally, although familial cases of urticaria pigmentosa, diffuse cutaneous mastocytosis and mastocytomas have been reported, to our knowledge, this is the first report of urticaria pigmentosa seen in twins at the same time, which suggests that this form of mastocytosis is also genetically determined.[6],[9],[10],[11]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the legal guardian has given his consent for images and other clinical information to be reported in the journal. The guardian understands that names and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Kiszewski AE, Durán-Mckinster C, Orozco-Covarrubias L, Gutiérrez-Castrellón P, Ruiz-Maldonado R. Cutaneous mastocytosis in children: A clinical analysis of 71 cases. J Eur Acad Dermatol Venereol 2004;18:285-90.
[Google Scholar]
|
| 2. |
Ben-Amitai D, Metzker A, Cohen HA. Pediatric cutaneous mastocytosis: A review of 180 patients. Isr Med Assoc J 2005;7:320-2.
[Google Scholar]
|
| 3. |
Valent P, Akin C, Metcalfe DD. Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts. Blood 2017;129:1420-7.
[Google Scholar]
|
| 4. |
Valent P, Akin C, Hartmann K, Nilsson G, Reiter A, Hermine O, et al. Advances in the classification and treatment of mastocytosis: Current status and outlook toward the future. Cancer Res 2017;77:1261-70.
[Google Scholar]
|
| 5. |
Hartmann K, Escribano L, Grattan C, Brockow K, Carter MC, Alvarez-Twose I, et al. Cutaneous manifestations in patients with mastocytosis: Consensus report of the European Competence Network on Mastocytosis; the American Academy of Allergy, Asthma and Immunology; and the European Academy of Allergology and Clinical Immunology. J Allergy Clin Immunol 2016;137:35-45.
[Google Scholar]
|
| 6. |
de la Sotta P, Romero WA, Kramer D, Cárdenas C, González S. Cutaneous mastocytosis in twins: Multiple mastocytomas and urticaria pigmentosa in two pairs of monozygotic twins. Pediatr Dermatol 2011;28:585-7.
[Google Scholar]
|
| 7. |
Pollard WL, Beachkofsky TM, Kobayashi TT. Novel R634W c-kit mutation identified in familial mastocytosis. Pediatr Dermatol 2015;32:267-70.
[Google Scholar]
|
| 8. |
Güneş Bilgili S, Karadaǧ AS, Takci Z, Çalka Ö, Kösem M. Comparison of cutaneous mastocytosis with onset in children and adults. Turk J Med Sci 2014;44:504-10.
[Google Scholar]
|
| 9. |
Cainelli T, Marchesi L, Pasquali F, Rozzoni M. Monozygotic twins discordant for cutaneous mastocytosis. Arch Dermatol 1983;119:1021-2.
[Google Scholar]
|
| 10. |
Duckworth AK, Bhatti A, Barnes C. Diffuse cutaneous mastocytosis in fraternal twins. Int J Dermatol 2009;48:170-2.
[Google Scholar]
|
| 11. |
Rockoff AS. Urticaria pigmentosa in identical twins. Arch Dermatol 1978;114:1227-8.
[Google Scholar]
|
Fulltext Views
4,165
PDF downloads
1,473





![[Figure - 1]](#fig_ijdvl_2019_85_5_509_264007_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_5_509_264007_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2019_85_5_509_264007_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2019_85_5_509_264007_f4.jpg){kind=link}