Translate this page into:
Handheld narrow band ultraviolet B comb as home phototherapy device for localised vitiligo: Dosimetry and calibration
Correspondence Address:
Sujay Khandpur
Room No 4071, 4th Floor Teaching Block, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029
India
| How to cite this article: Khandpur S, Bhatia R. Handheld narrow band ultraviolet B comb as home phototherapy device for localised vitiligo: Dosimetry and calibration. Indian J Dermatol Venereol Leprol 2018;84:78-80 |
Sir,
Phototherapy is an established therapeutic modality for vitiligo with high repigmentation rates and good safety profile. Narrowband-UVB (NB-UVB) involves the use of UV-lamps with peak emission at 311 nm. The efficacy of NB-UVB in vitiligo was first demonstrated by Westerhof and Nieuwboer-Krobotova in 1997, and since then, several clinical studies have demonstrated its effectiveness in both generalized and localized vitiligo.[1],[2] NB-UVB therapy is currently being administered in whole body chambers which are usually available in tertiary care hospitals. This is an expensive equipment, requires regular hospital visits, and is inconvenient for patients travelling long distance for therapy, in addition to resulting in loss of wages for the patients and their attendants. To overcome these significant disadvantages of whole body cabinets, home-based NB-UVB therapy is the need of the hour; such devices are being used in both vitiligo and psoriasis with encouraging results.[3],[4] In addition, unnecessary exposure to uninvolved body sites in whole body cabinets would be circumvented by targeted home phototherapy devices. A home-based phototherapy unit that has been found as effective in psoriasis as the outpatient NB-UVB chamber, in a comparative trial, consists of 2 Philips TL-9 W/01 lamps and delivers NB-UVB at irradiance of 10 mW/cm2, over a 9 × 7 cm area for the treatment of localized lesions.[4] Several other studies have also documented the safety of home phototherapy.[5]
Numerous portable and lightweight handheld NB-UVB devices are now available in the market. NB-UVB comb is marketed in India primarily for the treatment of scalp psoriasis. It consists of two Philips TL-9W/01 NB-UVB lamps placed in a plastic casing that emit wavelength of 310–315 nm (peak 311 nm) over an 11 × 4 cm area, on which parallel arrays of toothed structures of approximately 2 cm length (comb) are attached [Figure - 1]. The comb is for removing thick scales present on the psoriatic plaques to adequately expose the lesions to NB-UVB radiation. We intend to use this equipment for delivering NB-UVB to localized patches of vitiligo on domiciliary basis. This equipment has been chosen because it is lightweight, handheld, easily available, easy to maintain and store, and inexpensive. The toothed structures or comb would maintain a uniform distance between the NB-UVB lamps and vitiligo patches. However, there is no data on irradiance measurements from these devices. Irradiance is defined as radiant power incident on a surface from all forward angles, per unit area, expressed as W/m2 or mW/cm2 nm in a specified wavelength range. Fluence or dose is the energy incident on the skin during a treatment session calculated as follows: UVR dose = irradiance × treatment time. To use this equipment effectively, irradiance measurements should be made to assess the output from this device so that appropriate treatment protocol for vitiligo in terms of initial exposure time and increments of exposure to NB-UVB can be formulated. The present study was undertaken to determine the irradiance of handheld NB-UVB comb as a preliminary step to adopt it as a home phototherapy device in limited vitiligo.
 |
| Figure 1: Hand-held narrow band ultraviolet B comb (V-Care Meditech Pvt. Ltd., Bengaluru, India) |
A total of 22 handheld NB-UVB combs (V-Care Meditech Pvt. Ltd., Bangalore, India) were tested for irradiance measurement using an integrated UV meter (Herbert Waldmann GmbH and Co. KG Villingen-Schwenningen, Germany). The sensor of the UV meter was kept at a distance of approximately 2 cm from the lamp (length of the teeth of the NB-UVB comb) [Figure - 2]. The comb was switched on for 45 seconds to warm up the device and the irradiance was measured at 45 seconds, 1 minute, 2 minutes, 3 minutes, 4 minutes, and 5 minutes. This measurement was undertaken for all the devices.
 |
| Figure 2: Calibration of irradiance of narrow band ultraviolet B comb using an integrated ultraviolet meter (Herbert Waldmann GmbH and Co. KG Villingen-Schwenningen, Germany) |
There was a progressive decay in the irradiance of NB-UVB combs with time. The mean irradiance from 22 combs at 45 seconds was 6.84 mW/cm2 (range 5.64–7.87), 6.5 (range 5.56–7.82) at 1 minute, 6.4 (range 5.26–7.22) at 2 minutes, 5.9 (range 4.94–6.71) at 3 minutes, 5.5 (range 4.62–6.25) at 4 minutes and 5.1 mW/cm2 (range 4.29–5.83) at 5 minutes. The output was again measured from 6 combs after 3 months of use. The mean irradiance was 5 mW/cm2 (4.32–5.99) at 45 seconds, 5.0 (4.33–6.11) at 1 minute, 4.9 (4.07–6.01) at 2 minutes, 3.8 (3.77–5.67) at 3 minutes, 4.3 (3.51–5.28) at 4 minutes and 4.1 (3.30–4.91) at 5 minutes. There was decay in irradiance after 3 months. The decay was 26.9%, 23.1%, 23.4%, 35.6%, 21.8% and 19.6% at each time interval measured [Figure - 3] and [Figure - 4]. In terms of the exposure time required to irradiate vitiligo patches with a starting dose of 350mJ/cm2, it would be 54 seconds, 55, 59, 64, 69 seconds for the first 5 vitiligo patches and the exposure time would increase to 70 seconds, 71, 92, 81 and 85 seconds after 3 months of use, as a result of decay in irradiance of lamps.
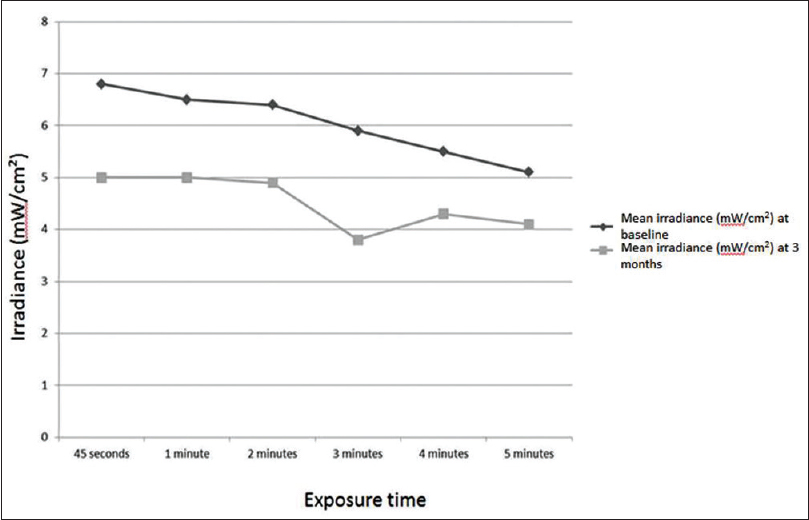 |
| Figure 3: Mean irradiance of narrow band ultraviolet B combs at baseline and after 3 months |
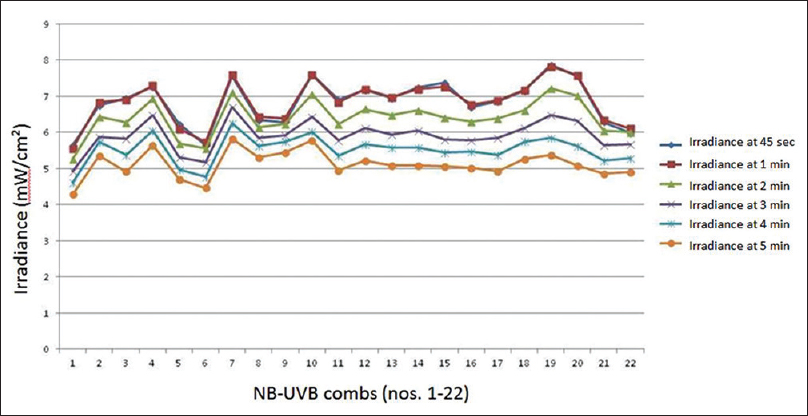 |
| Figure 4: Change in irradiance of narrow band ultraviolet B combs with time |
In our irradiance- measurement study, the mean irradiance from hand-held NB-UVB device was found to be 6.84 mw/cm2 after a warm-up time of 45 seconds, which decreased to 5.1 mW/cm2 after 5 minutes. The irradiance of Philips type TL-01 100 W fluorescent tubes used in whole body chambers is known to decline rapidly over the first 200 operating hours, dropping to 60–70% of the initial intensity, and then a relatively constant output is maintained until lamp failure.[6] Due to lamp failure, cold spots or localized low irradiance areas are formed leading to low overall irradiance. In lamps used for whole body chambers, single lamp failure leads to fall in irradiance by 7–12% while a new lamp gives hot spots of 3–6%. In smaller devices, each lamp contributes higher to overall irradiance, hence the fall of irradiance with a single lamp failure is higher, up to 30%.[7] However, the rate of decay of irradiance with handheld NB-UVB device is not clear. In a trial involving 29 vitiligo cases, patients were randomized to receive hand-held phototherapy (2 groups receiving Waldmann and Dermfix devices) and placebo handheld phototherapy for 16 weeks.[8] In 12% of the active group, there was significant repigmentation (>75%) at the end of 16 weeks. Overall, there was little impact on the quality of life (measured by Dermatology life quality index scores). The mean output was found to be approximately 4.5 and 3.8 mW/cm2 for Waldmann and Dermfix, respectively. Similar to our study, there was an increase in the output for first 60 seconds followed by a gradual decay over time. Furthermore, at the end of 16 weeks there was a fall in the output of Waldmann and Dermfix devices by 38.5% and 28.5%, respectively.[8]
A study involving 93 Chinese vitiligo patients treated with handheld NB-UVB device with 2 Philips TL-9W/01 lamps showed good re-pigmentation (75%) in 22.6% (21/93) at 6 months, the exposure time was roughly determined by the patient based on the development of erythema.[3] This method of calculation of exposure time may put the patient at risk of both over and under exposure to radiation. Moreover, in this study, re-pigmentation was rapid only in the initial 3 months, stabilizing thereafter. This might support our finding of a decay in the irradiance after 3 months of use and the need to adjust the duration of exposure for each patch after recalculating the irradiance.
Home-based handheld NB-UVB therapy could be an important addition to the treatment options available to patients with localized vitiligo and may in fact completely substitute hospital-based phototherapy. At present, the disadvantage of hand-held NB-UVB device seems to be its output, nearly half of that of the whole-body cabinets with a faster rate of decay in irradiance, necessitating greater exposure time to the lesion to achieve a therapeutic fluence. Given the decay in irradiance with time, the equipment should be periodically calibrated and the correct duration of exposure determined for optimum results.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Westerhof W, Nieuweboer-Krobotova L. Treatment of vitiligo with UV-B radiation vs. topical psoralen plus UV-A. Arch Dermatol 1997;133:1525-8.
[Google Scholar]
|
| 2. |
Njoo MD, Spuls PI, Bos JD, Westerhof W, Bossuyt PM. Nonsurgical repigmentation therapies in vitiligo. Meta-analysis of the literature. Arch Dermatol 1998;134:1532-40.
[Google Scholar]
|
| 3. |
Shan X, Wang C, Tian H, Yang B, Zhang F. Narrow-band ultraviolet B home phototherapy in vitiligo. Indian J Dermatol Venereol Leprol 2014;80:336-8.
[Google Scholar]
|
| 4. |
Koek MB, Buskens E, van Weelden H, Steegmans PH, Bruijnzeel-Koomen CA, Sigurdsson V. Home versus outpatient ultraviolet B phototherapy for mild to severe psoriasis: Pragmatic multicentre randomised controlled non-inferiority trial (PLUTO study). BMJ 2009;338:b1542.
[Google Scholar]
|
| 5. |
Cameron H, Yule S, Dawe RS, Ibbotson SH, Moseley H, Ferguson J. Review of an established UK home phototherapy service 1998-2011: Improving access to a cost-effective treatment for chronic skin disease. Public Health 2014;128:317-24.
[Google Scholar]
|
| 6. |
Amatiello H, Martin CJ. Ultraviolet phototherapy: Review of options for cabin dosimetry and operation. Phys Med Biol 2006;51:299-309.
[Google Scholar]
|
| 7. |
Moseley H, Allan D, Amatiello H, Coleman A, du Peloux Menagé H, Edwards C, et al. Guidelines on the measurement of ultraviolet radiation levels in ultraviolet phototherapy: Report issued by the British Association of Dermatologists and British Photodermatology Group 2015. Br J Dermatol 2015;173:333-50.
[Google Scholar]
|
| 8. |
Eleftheriadou V. Setting Priorities and Reducing Uncertainties for the Treatment of Vitiligo. PhD Thesis; University of Nottingham; 2013. Available from: https://www.core.ac.uk/download/pdf/17208415.pdf. [Last accessed on 2017 Feb 12].
[Google Scholar]
|
Fulltext Views
8,022
PDF downloads
2,255





![[Figure - 1]](#fig_ijdvl_2018_84_1_78_220783_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_1_78_220783_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_1_78_220783_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_1_78_220783_f4.jpg){kind=link}