Translate this page into:
Nevoid sebaceous hyperplasia mistaken as nevus sebaceous: Report of four cases
2 Department of Dermatology, KPC Medical College and Hospital, Kolkata, West Bengal, India
3 Department of Pathology, North Bengal Medical College and Hospital, Darjeeling, West Bengal, India
Correspondence Address:
Anupam Das
Department of Dermatology, KPC Medical College and Hospital, Kolkata, West Bengal
India
| How to cite this article: Mandal RK, Das A, Chakrabarti I, Agarwal P. Nevoid sebaceous hyperplasia mistaken as nevus sebaceous: Report of four cases. Indian J Dermatol Venereol Leprol 2017;83:213-216 |
Sir,
Sebaceous gland hyperplasia is a benign hamartoma composed of epidermal appendages with sebaceous differentiation. This condition is mostly seen in adults and is characterized by multiple asymptomatic yellowish to skin-colored papules on the face. Rare variants include linear, diffuse, familial and giant forms. Here, we report a case series of four children with nevoid (linear) sebaceous hyperplasia since birth. The extreme rarity of this entity and its clinical resemblance to nevus sebaceous prompted the present report.
The first patient was a 6-year-old girl who presented with multiple yellowish bumps on the right side of the face since birth. Cutaneous examination revealed multiple skin-colored papules coalescing to plaques in a linear distribution on the zygomatic arch of the right side [Figure 1a]. The lesions were growing in proportion to the size of the face.
 |
| Figure 1a: Multiple yellowish papules and plaques distributed on the cheeks |
The second patient was a 7-year-old girl with multiple yellowish papules and plaques, with a central dell-like depression in some lesions, since birth. The lesions were present on the zygomatic arch of the left side [Figure 1b].
 |
| Figure 1b: Multiple yellowish papules and plaques distributed on the cheeks |
The third patient was a 10-year-old girl with similar papules and plaques distributed on the right side of the face. Her parents were unable to pinpoint the age of onset. Examination revealed dell-like depressions on the top of the papules [Figure 1c].
 |
| Figure 1c: Multiple yellowish papules and plaques distributed on the cheeks |
The fourth patient was an 8-year-old girl with identical papules coalescing to form plaques, located on the retroauricular region of the right side, since birth [Figure 1d].
 |
| Figure 1d: Multiple yellowish papules and plaques distributed on the retroauricular region |
All the cases presented to us at the Dermatology Outpatients' Department of North Bengal Medical College and Hospital, Darjeeling, except the third case who consulted us at a private clinic in Barrackpore, West Bengal. Past history and family history were noncontributory in all the cases. In each case, a clinical provisional diagnosis of nevus sebaceous was thought of; however, the clinical picture [Figure - 2] (papules with central dell-like depression) and the lack of any morphological change in the lesions since birth, made us consider nevoid sebaceous hyperplasia as a differential diagnosis. Hence, a biopsy was done for confirmation. Histologically, there was increased number of sebaceous glands close to the epidermis. The glands were mostly composed of mature sebaceous lobules with independent ducts that opened up directly to the surface of the skin [Figure - 3]. Although most of the lobules were composed of mature sebocytes, some lobules showed the presence of undifferentiated, generative cells with scant cytoplasm in the periphery [Figure - 4]. There was the absence of any rudimentary hair follicle.
 |
| Figure 2: Dell-like depression on the top of the papules |
 |
| Figure 3: Increased number of sebaceous glands near the epidermis. The ducts opening directly to the skin surface (H and E, ×10) |
 |
| Figure 4: Most of the lobules composed of mature sebocytes, some showing undifferentiated, generative cells with scant cytoplasm in the periphery of the lobules (H and E, ×100) |
Differentiation of linear sebaceous hyperplasia from nevus sebaceous is important. There are a few clinical and histological pointers which can differentiate these two entities [Table - 1]. Clinically, nevus sebaceous presents as a flat, smooth-surfaced, solitary plaque, mostly on the scalp since birth. Slowly, the surface becomes irregular and verrucous at puberty. Nevoid sebaceous hyperplasia, on the other hand, presents as multiple skin colored to yellowish papules with central depression. Here, the face is the most common site and there is no surface change that occurs with age.
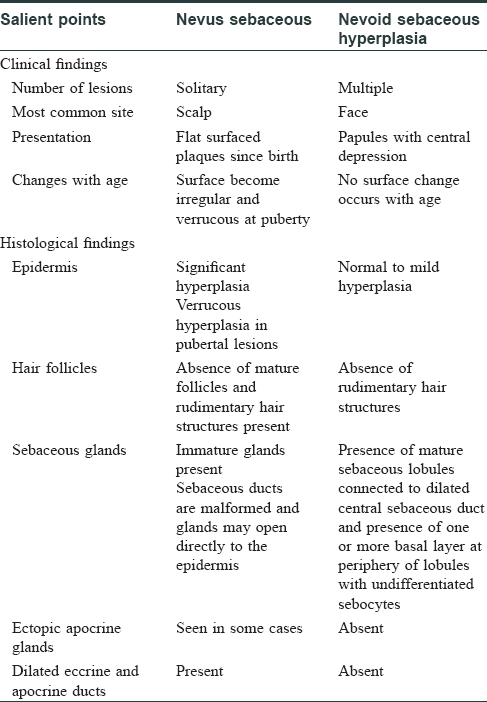
Histopathologically, in the latter, in childhood, there is mild epidermal hyperplasia, abrupt absence of mature hair follicles, vestigial hair structures, immature sebaceous glands and vertically arranged ectopic apocrine ducts in some cases. In the verrucous or nodular stage that occurs in puberty, numerous irregularly arranged sebaceous glands can be seen in the histopathology, which are usually superficially located, often with ectatic ducts opening directly into the epidermis. The epidermis frequently shows verrucous hyperplasia.[1],[2]
On the other hand, sebaceous hyperplasia shows increased number of sebaceous glands close to the epidermis, composed of mature sebaceous lobules with independent ducts that open up directly to the surface of the skin. Although most of the lobules are composed of mature sebocytes, some lobules show the presence of a single layer of undifferentiated, generative cells with scant cytoplasm in the periphery. There is the absence of any rudimentary hair follicle.
In our cases, the clinical as well as the histopathological pictures were compatible with sebaceous hyperplasia. Therefore, on the basis of clinicopathological correlation, a diagnosis of “nevoid sebaceous hyperplasia” was rendered. The parents were counseled regarding the benign nature of the disease and advised periodic follow-up.
Atypical proliferations of sebaceous glands include linear (nevoid) sebaceous hyperplasia, senile sebaceous hyperplasia, nevus sebaceous of Jadassohn, linear papular ectodermal-mesodermal hamartoma and juxtaclavicular beaded lines.[3]
Sebaceous hyperplasia usually develops in a background of actinic damage, mostly in the elderly population. Clinically, it is characterized by multiple yellowish papules (1–3 mm diameter) distributed on the forehead, cheeks, neck, lips, rarely oral mucosa, vulva, thorax, areola, penile shaft, etc.[4] A central comedone may be present in some lesions. Rare presentation includes papules and plaques distributed in a linear configuration. Clinical differentials include nevus comedonicus, nevus sebaceous, sebaceous epithelioma, follicular sebaceous cystic hamartoma, sebaceous adenoma and trichofolliculoma.
The differentiation of sebocytes in sebaceous gland hyperplasia is different from that found in normal sebaceous glands. The cells are smaller, but the nuclei are larger and rich in glycogen. The sebum production is also quite low in comparison to a normal sebaceous gland.
In 1984, Fernandez and Torres were the first to report cases of linear hyperplasia of the sebaceous glands on the preauricular and retroauricular areas, neck and cheeks.[5] Some cases of linear sebaceous gland hyperplasia on the chest, penis and ear have been reported.[6],[7],[8],[9]
Treatment is usually not required. However, options include cryotherapy, electrocautery, topical retinoids and surgical excision.
Nevoid sebaceous hyperplasia is a rare entity and quite often, it is diagnosed as nevus sebaceous, due to close clinical resemblance. Here, we report four cases of nevoid sebaceous hyperplasia, which were clinically diagnosed as nevus sebaceous, thus highlighting the importance of detailed histopathological importance of such cases.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Bhawan J, Calhoun J. Premature sebaceous gland hyperplasia. J Am Acad Dermatol 1983;8:136.
[Google Scholar]
|
| 2. |
De Villez RL, Roberts LC. Premature sebaceous gland hyperplasia. J Am Acad Dermatol 1982;6:933-5.
[Google Scholar]
|
| 3. |
Finan MC, Apgar JT. Juxta-clavicular beaded lines: A subepidermal proliferation of sebaceous gland elements. J Cutan Pathol 1991;18:464-8.
[Google Scholar]
|
| 4. |
Bakaris S, Kiran H, Kiran G. Sebaceous gland hyperplasia of the vulva. Aust N Z J Obstet Gynaecol 2004;44:75-6.
[Google Scholar]
|
| 5. |
Fernandez N, Torres A. Hyperplasia of sebaceous glands in a linear pattern of papules. Report of four cases. Am J Dermatopathol 1984;6:237-43.
[Google Scholar]
|
| 6. |
Sato T, Tanaka M. Linear sebaceous hyperplasia on the chest. Dermatol Pract Concept 2014;4:93-5.
[Google Scholar]
|
| 7. |
Kumar A, Kossard S. Band-like sebaceous hyperplasia over the penis. Australas J Dermatol 1999;40:47-8.
[Google Scholar]
|
| 8. |
Vergara G, Belinchón I, Silvestre JF, Albares MP, Pascual JC. Linear sebaceous gland hyperplasia of the penis: A case report. J Am Acad Dermatol 2003;48:149-50.
[Google Scholar]
|
| 9. |
Nair PA, Diwan NG. Sebaceous hyperplasia mimicking linear wart over ear. Int J Trichology 2015;7:170-2.
[Google Scholar]
|
Fulltext Views
18,095
PDF downloads
4,404





![[Figure - 2]](#fig_ijdvl_2017_83_2_213_199424_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_2_213_199424_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2017_83_2_213_199424_f4.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_2_213_199424_t8.jpg){kind=link}