Translate this page into:
Angioma serpiginosum: A case series of 4 patients
2 Department of Pathology, Institute of Pathology, Indian Council of Medical Research, New Delhi, India
Correspondence Address:
Sarvesh Sunil Thatte
Department of Dermatology, Venereology and Leprosy, Dr. P.N. Behl Skin Institute and School of Dermatology, New Delhi - 110 048
India
| How to cite this article: Bhushan P, Thatte SS, Singh A. Angioma serpiginosum: A case series of 4 patients. Indian J Dermatol Venereol Leprol 2016;82:588 |
Sir,
Angioma serpiginosum is clinically characterized by multiple copper to red-colored grouped macules that are arranged in serpiginous or gyrate patterns. Histologically, it is characterized by dilatation and proliferation of vessels in the papillary dermis.[1] The occurrence of angioma serpiginosum on the upper limb is rare while we were unable to find previous reports of its occurrence on the face and neck.
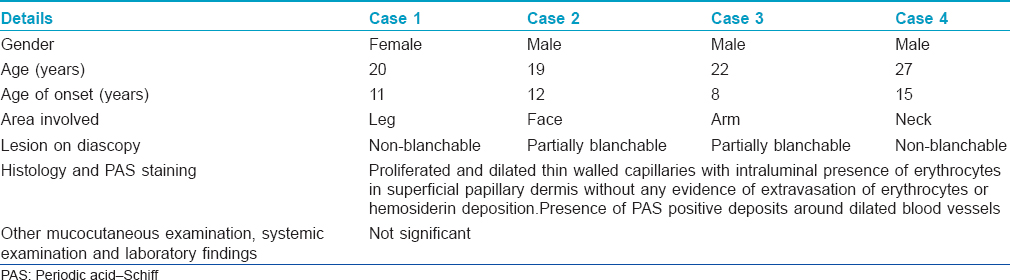
Four patients aged 20, 19, 22 and 27 years presented with complaints of multiple, well-defined, discrete to confluent, punctate, red to coppery macules and some papules on the right leg [Figure - 1], the right side of the upper lip, dorsum of nose and right cheek [Figure - 2], the right arm [Figure - 3], the left side of neck, left ear lobe and left preauricular region [Figure - 4], arranged in a nevoid pattern [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4] and [Table - 1]. On diascopy, the lesions in the first and fourth patient were non-blanchable while those in the second and third patient were partially blanchable. Ophthalmic and otorhinolaryngeal examination in patients having lesions on the face and neck did not reveal any abnormality.
 |
| Figure 1: Multiple, well defined, discrete to confluent, bright red coloured, macules having irregular margins present on the right lower limb |
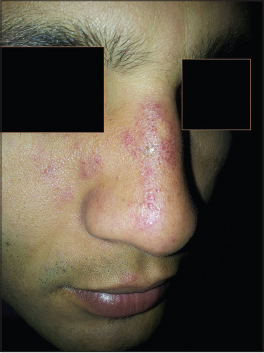 |
| Figure 2: Multiple, well-defined, discrete to confluent, punctate, red-colored to coppery, partially blanchable macules and some papules present on the right side of face |
 |
| Figure 3: Multiple, well-defined, erythematous to copper colored, partially blanchable, macules and papules having smooth surface and irregular margins present on the right arm |
 |
| Figure 4: Multiple, well-defined, punctate, smooth surfaced, reddish brown colored macules with irregular margins present on the left side of neck, left ear lobe and left preauricular area |
In all patients, the rest of the mucocutaneous examination, systemic examination and laboratory parameters were normal. Differential diagnoses of pigmented purpuric dermatosis, unilateral nevoid telangiectasia and angioma serpiginosum were considered in case 1 while unilateral nevoid telangiectasia and angioma serpiginosum were considered as differential diagnoses for cases 2, 3 and 4. Histopathological examination from an erythematous, non-blanchable macule revealed multiple proliferaing and dilated thin-walled capillaries with intraluminal presence of erythrocytes in the superficial papillary dermis without any evidence of extravasation of erythrocytes or hemosiderin deposition or perivascular inflammatory infiltrate [Figure - 5]. Periodic acid–Schiff staining revealed periodic acid–Schiff positive deposits around dilated blood vessels [Figure - 6] in all the four patients. On the basis of clinical examination and histological findings, a final diagnosis of angioma serpiginosum was made in all the four cases.
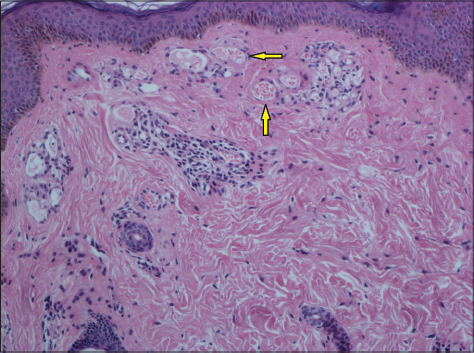 |
| Figure 5: Multiple proliferated and dilated thin walled capillaries with intraluminal presence of erythrocytes in superficial papillary dermis (arrow) without any evidence of extravasation of erythrocytes or hemosiderin deposition (H and E, ×100) |
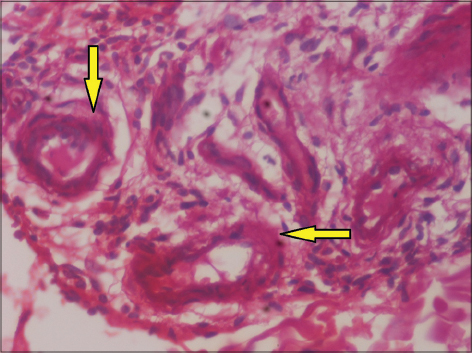 |
| Figure 6: Periodic acid–Schiff positive deposits around dilated blood vessels (arrow) (H and E, ×400) |
Angioma serpiginosum, a rare, benign, acquired, vascular nevoid condition was first described by Hutchinson in 1889.[2] The condition is usually sporadic, has a female preponderance and mainly affects lower extremities and buttocks. The condition is an asymptomatic, yet progressive anomaly that usually starts in early childhood and stabilizes in adults. It is rare for angioma serpiginosum to undergo complete spontaneous involution; however it may undergo partial involution. Clinically, lesions are copper to bright red, punctate, non-blanchable or partially blanchable, grouped macules that may develop into papules with a background of erythema. Lesions enlarge by developing new lesions at the periphery with clearing of lesions in the center and this leads to a serpiginous or gyrate or ring-like morphology.[1]
Angioma serpiginosum is a mosaic condition of unknown etiology. Estrogen was considered to be an important hormone in the development of angioma serpiginosum owing to its proliferative effects on vascular endothelial cells supporting the role of hormones for the cause of increased incidence of angioma serpiginosum in women.[3] However, recently, the role of hormones in its pathogenesis was disproved due to the absence of estrogen and progesterone receptors on the involved blood vessels.[4] Another proposed etiology is an abnormal vascular response to cold that manifests as formation and aggregation of newly formed capillaries that leads to large ectatic vessels in the papillary dermis.[2]
Though angioma serpiginosum is more common in women, it may also occur in men, as in our case series.[5] Angioma serpiginosum predominantly affects the lower extremities and buttocks though the upper extremity as in our case, the sole, and other body sites can rarely be involved.[2],[4],[5] However, we were unable to find any previous reports of the involvement of the face and neck. Dermoscopy with the characteristic presence of round to oval red lagoons and histopathology showing proliferating and dilated capillaries in the superficial papillary dermis, periodic acid–Schiff positive deposits around involved vessels and absence of erythrocyte extravasation or hemosiderin deposits or inflammatory cells helps to differentiate angioma serpiginosum from its closest mimics, pigmented purpuric dermatoses and unilateral nevoid telangiectesia.[5] All four patients had periodic acid–Schiff positive deposits around dilated blood vessels. However, this finding needs further corroboration in larger studies before being considered a diagnostic marker of the condition.[5] Argon laser, pulsed dye laser and intense pulsed light may give promising results in terms of clearance of lesions.[1],[2],[5]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form. The patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Namazi MR, Handjani F. Angioma serpiginosum. Dermatol Online J2003;9:19.
[Google Scholar]
|
| 2. |
Chen JH, Wang KH, Hu CH, Chiu JS. Atypical angioma serpiginosum. Yonsei Med J2008;49:509-13.
[Google Scholar]
|
| 3. |
Xiao X, Hong L, Sheng M. Promoting effect of estrogen on the proliferation of hemangioma vascular endothelial cells in vitro. J Pediatr Surg1999;34:1603-5.
[Google Scholar]
|
| 4. |
Bayramgurler D, Filinte D, Kiran R. Angioma serpiginosum with sole involvement. Eur J Dermatol2008;18:708-9.
[Google Scholar]
|
| 5. |
Ilknur T, Fetil E, Akarsu S, Altiner DD, Ulukus C, Günes AT. Angioma serpiginosum: Dermoscopy for diagnosis, pulsed dye laser for treatment. J Dermatol 2006;33:252-5.
[Google Scholar]
|
Fulltext Views
10,941
PDF downloads
2,027





![[Figure - 1]](#fig_ijdvl_2016_82_5_588_182972_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_5_588_182972_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_5_588_182972_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2016_82_5_588_182972_f4.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2016_82_5_588_182972_t7.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2016_82_5_588_182972_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2016_82_5_588_182972_f6.jpg){kind=link}