Translate this page into:
Facial variant of eruptive vellus hair cyst
2 Institute of Pathology, Indian Council of Medical Research, New Delhi, India
Correspondence Address:
Premanshu Bhushan
Consultant Dermatologist, Skin Institute and School of Dermatology, N- Block, Greater Kailash-1, New Delhi - 110 048
India
| How to cite this article: Bhushan P, Singh A. Facial variant of eruptive vellus hair cyst. Indian J Dermatol Venereol Leprol 2014;80:96 |
Sir,
Eruptive vellus hair cysts (EVHC) are uncommon, benign, asymptomatic, epidermal cysts histologically characterized by cystic spaces lined by undulating stratified squamous epithelium and filled with laminated keratinous debris and vellus hairs. The lesions mostly affect children and young adults mainly over chest, abdomen, and extremities; [1] while face is relatively infrequently involved. [2]
An 18-year-old male student presented with multiple, smooth, dome-shaped, asymptomatic, and skin-colored to yellowish papules of sizes 2-5 mm over forehead for last 5 years [Figure - 1]. No other site of the body was involved and rest of skin, hairs, nails, and mucosae were normal. Patient denied use of cosmetics, exposure to chemicals, excessive sun exposure, or mechanical trauma prior to the eruptions. No family members had similar lesions. He had been treated for acne with topical and systemic agents with little response. Skin biopsy revealed a cyst lined by a two to three layers of undulating stratified squamous epithelium with granular layer and filled with keratinous debris and numerous vellus hairs [Figure - 2]. No sebaceous gland was seen within or adjacent to the cyst wall. Final diagnosis of EVHC was made and patient was offered mechanical treatment which was refused, and hence patient was started on topical tretinoin 0.05% with mild improvement reported after 2 months.
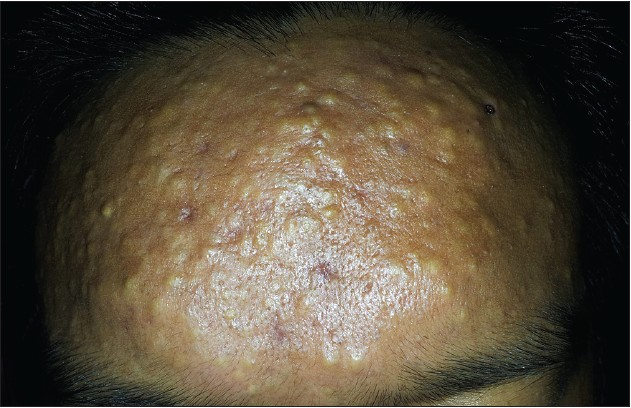 |
| Figure 1: Multiple yellowish, dome-shaped papules over forehead |
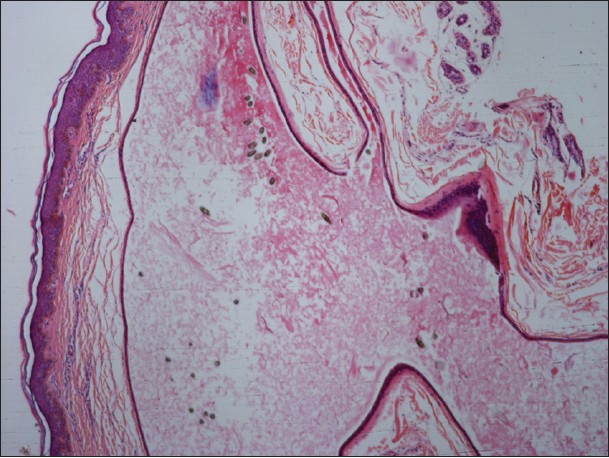 |
| Figure 2: Slightly acanthotic epidermis overlying the cyst lined by a flat and undulating lining of stratified squamous epithelium of two to three cell layers thickness with granular layer. The cyst lumen is filled with keratinous material and numerous vellus hairs (H and E, ×100) |
Since the first report in 1977, more than 200 cases of EVHC have been reported from various parts of the world. [1] Both sexes are affected equally and presentation can be acquired, familial, late onset, or associated with other diseases and syndromes like steatocystoma, pachyonychia congenita, Lowe syndrome, etc. [1] The histopathogenesis of vellus hair cyst remains controversial and its nosological position viz-a-viz steatocystoma multiplex is debated. [3] Classical steatocystoma histologically reveals stratified squamous epithelium lined cyst without a granular layer with compressed sebaceous gland within or close to the cyst wall. EVHC on the other hand is lined by stratified squamous epithelium with granular layer with keratin debris and vellus hairs in the cavity. However, the granular layer and few vellus hairs may also be present in steatocystoma, while EVHC may also have sebaceous glands in their wall. Therefore, terminologies like hybrid cyst and pilosebaceous cyst has been used. [3] Probably, EVHC originates from the infundibulum/isthmus region; steatocystoma from the sebaceous duct and mixed forms (pilosebaceous cysts) from the junction of pilosebaceous duct. However, steatocystoma expresses both keratin 10 (K10) and K17, while EVHC expresses only K17; arguing for them to be separate entities. [3] We preferred the diagnosis of EVHC over steatocystoma based on the absence of sebaceous glands in the wall, presence of granular layer and large number of vellus hairs in the lumen.
Facial EVHC is uncommon and Lew et al., recounted only eight patients. [2] Facial EVHC have been described as macular, papular, skin-colored, pink, slate hyperpigmented, nevus of Ota like, and even unilateral. [2],[3] Sites of involvement include forehead, cheeks, and periorbital areas. Furthermore, there is scarcity of reports from India and we could locate only three reports of EVHC from India on the PubMed. [3],[4],[5] Singh et al., presented the first case of EVHC over chest in a 10-year-old child in 1993. [5] Rao et al., reported a patient with skin-colored papules and comedo-like openings on anterior chest and abdomen; [3] while Saha et al., described one case of multiple dome-shaped cysts over the forehead. [4]
The treatment of EVHC remains problematic. Mechanical treatments with needle evacuation, dermabrasion, lasers, or surgery [3] are complicated by scarring and recurrences. This is even more important in facial variant. Spontaneous resolution by transepidermal elimination occurs in 25% of cases, but has not been reported in facial EVHC. [2] Topical therapies like urea, retinoids, and lactic acid are minimally effective, but offer a safer alternative for facial lesions. Our patient showed minimal improvement with tretinoin 0.05% after 2 months.
It is believed that EVHC are commoner than it appears from the scarcity of literature. [1] Moreover, the paucity of reports from India indicates that EVHC indeed is underdiagnosed and/or underreported. Facial involvement is especially apt to be misdiagnosed as milia, acne, steatocytoma, molluscum, and epidermal cysts. [3] Our report is aimed at generating awareness about this uncommon diagnosis amongst dermatologists in general and Indian dermatologists in particular.
| 1. |
Torchia D, Vega J, Schachner LA. Eruptive vellus hair cysts: A systematic review. Am J Clin Dermatol 2012;13:19-28.
[Google Scholar]
|
| 2. |
Lew BL, Lee MH, Haw CR. Unilateral eruptive vellus hair cysts occurring on the face. J Eur Acad Dermatol Venereol 2006;20:1314-6.
[Google Scholar]
|
| 3. |
Rao R, Balachandran C. Asymptomatic papular lesions on the trunk. Indian J Dermatol Venereol Leprol 2009;75:217-9.
[Google Scholar]
|
| 4. |
Saha A, Das NK, Gharami RC, Chowdhury SN, Datta PK. A clinico-histopathological study of appendageal skin tumors, affecting head and neck region in patients attending the dermatology opd of a tertiary care centre in eastern India. Indian J Dermatol 2011;56:33-6.
[Google Scholar]
|
| 5. |
Singh A, Ponnaiya J. Eruptive vellus hair cysts: A case report. Indian J Pathol Microbiol 1993;36:289-91.
[Google Scholar]
|
Fulltext Views
9,231
PDF downloads
1,399





![[Figure - 1]](#fig_ijdvl_2014_80_1_96_125513_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_1_96_125513_u2.jpg){kind=link}