Translate this page into:
A comparative study on efficacy of high and low fluence Q-switched Nd:YAG laser and glycolic acid peel in melasma
Correspondence Address:
Hemanta Kumar Kar
Department of Dermatology, STD and Leprosy, Dr. RML Hospital and PGIMER, Baba Kharak Singh Marg, New Delhi - 110 001
India
| How to cite this article: Kar HK, Gupta L, Chauhan A. A comparative study on efficacy of high and low fluence Q-switched Nd:YAG laser and glycolic acid peel in melasma. Indian J Dermatol Venereol Leprol 2012;78:165-171 |
Abstract
Background: Melasma is acquired symmetric hypermelanosis characterized by light-to-deep brown pigmentation over cheeks, forehead, upper lip, and nose. Treatment of this condition is difficult and associated with high recurrence rates. With the advent of newer therapies, there is interest in the use of glycolic acid peels and Q-switched Nd:YAG laser (QSNYL) in high and low fluence for this disorder. Aims: To compare the therapeutic efficacy of low fluence QSNYL, high fluence QSNYL, and glycolic acid peel in melasma in three study groups of 25 patients each. Methods: Seventy-five Indian patients diagnosed as melasma were included. These patients were randomly divided in three groups (Group A = 25 patients of melasma treated with low-fluence QSNYL at weekly intervals, Group B = 25 patients of melasma treated with glycolic acid peel at 2 weeks intervals, Group C = 25 patients of melasma treated with high-fluence QSNYL at 2 weeks intervals). Study period and follow-up period was of 12 weeks each. Out of the 75 patients included, 21 patients in Group A, 19 patients in Group B, and 20 patients in Group C completed the study. Response to treatment was assessed using melasma area and severity index score. Results: Significant improvement was recorded in all the three groups. The improvement was statistically highly significant in Group A as compared to Group C (P<0.005), significant in Group A as compared to Group B (P<0.05), and also in Group B when compared to Group C (P<0.05). Low-fluence QSNYL was associated with least side effects. Conclusions: This study shows the efficacy of low-fluence QSNYL and glycolic acid peel in melasma. These could be an effective treatment options compared to conventional methods for the treatment of melasma.Introduction
Melasma is an acquired symmetric hypermelanosis characterized by irregular light-to-deep brown macules on sun-exposed skin. It is commonly observed in women and is more prevalent in dark complexion individuals. The disease is far more common in Hispanics, Orientals, and people of Indo-Chinese origin who live in locations that receive high-intensity UV radiation. [1] Three clinical patterns are known: Centrofacial (most common), malar, and mandibular. [2] In today′s modern world, it is a cause of great emotional and psycho-social stress to both men and women affecting their quality of life.
Based on visible light, Wood′s light examination, and skin histology, melasma can be divided into three types. Epidermal type that has increased melanin predominantly in the basal and suprabasal epidermis with pigment accentuation on Wood′s lamp. The dermal variant has melanin-laden macrophages in the perivascular distribution in the superficial and deep dermis without Wood′s lamp accentuation. The mixed type has elements of both and appears as deep brown color on Wood′s lamp examination. There is accentuation of only the epidermal component. [2],[3]
Melasma is known to have a multifactorial etiology. Contributing factors include increased UV exposure, pregnancy, cosmetics, genetic factors, endocrine factors, and hormonal therapy. [4],[5],[6] There is an increased synthesis of melanosomes in melanocytes and increased transfer of melanosomes to keratinocytes. The common denominator thereby is increase in the number and activity of melanocytes. [7]
The treatment of melasma has been challenging. Conventional treatments include sun protection and a wide array of topical depigmentary creams available in varying combinations containing azelaic acid, glycolic acid, hydroquinone, hydrocortisone, mometasone, tretinoin, arbutin, etc. Newer treatments such as glycolic acid peels which provide an aesthetic and therapeutic benefit to the skin with quick recovery time are now widely practiced. [8],[9],[10] Continuing advances in technology have expanded the dermatologists armamentarium to use of lasers which remove the pigment selectively. Use of high-fluence Q-switched Nd:YAG laser (QSNYL) in melasma is known to be associated with risk of post inflammatory pigmentation. [11] In our study, we have compared the therapeutic efficacy of low fluence QSNYL, high-fluence QSNYL, and glycolic acid peel (35%-70%) in melasma in three study groups of 25 patients each. Outcome was assessed in relation to reduction of pigment and area of pigmentation using melasma area and severity index (MASI) score. [12]
Methods
Seventy five-Indian patients diagnosed as melasma were included in the study. These patients were randomly divided in three groups (Group A = 25 patients of melasma treated with low-fluence QSNYL, Group B = 25 patients of melasma treated with glycolic acid peel, Group C = 25 patients of melasma treated with high-fluence QSNYL). All patients were obtained from the out patients of Department of Dermatology in our hospital from 2008 to 2010 for a study period of 12 weeks. The follow-up period after treatment was 12 weeks. Patients with age group 18 years and above of either sex were included. Patients who had not received any prior treatment were included. However, those who had received any kind of topical treatment for melasma were included after a wash out period of 6 weeks. Patient′s on oral contraceptives, hormone replacement therapy, pregnant, and lactating women, patients with any systemic or endocrinological illness or hypersensitivity to the chemical peel were excluded.
In all cases, the diagnosis was made on clinical appearance, Wood′s lamp examination and was confirmed on a 2-mm skin biopsy. The protocol of the study was approved by the Institutional ethical committee of Dr. R.M.L. Hospital, New Delhi before commencing the study. Consent was obtained from the patient before inclusion. Sun protection with a broad spectrum sunscreen lotion (SPF>30) was advised at the start of therapy, during the treatment period and in the 12 weeks follow-up period. No other topical therapy was advised. Topical anesthesia with eutectic mixture of lignocaine and prilocaine was applied for 2 h under occlusion prior to laser. Treatment was performed with the hand piece held perpendicular to skin surface with minimum overlap. The entire lesion was covered in a single pass. All personnel in the laser room wore appropriate eye protection glasses during the treatment. The patient wore a silicon-coated lead shield provided by the manufacturer of laser (Med-lite C6).
In Group A, low-fluence 1064-nm QSNYL (Med-lite C6, Hoya Con Bio Inc., Fremont, CA, USA) was administered at parameters 6-8 mm SS, 10 Hz, 0.5- 1 J/ cm 2 , 10 passes at weekly intervals for a total of 12 weeks. Increment of 0.1 J/week was done till energy fluency of 1 J/cm 2 was attained and was continued at 1 J/cm 2 till 12 th week. Passes were stopped in case of immediate lightening or mild erythema of skin.
In Group B, six sessions of glycolic acid peels were done at 2 weekly intervals. Skin was primed with topical retinoic acid 0.025% once daily for two weeks before the peel was started . Graded strength of 35%-70% glycolic acid peel (Neostrata, USA) was used on incremental basis. A post auricular sensitivity test of the peel was performed to determine any hypersensitivity. First peel was done with 35% glycolic peel applied for 1 min. Contact time was 2 and 3 min in the second and third sessions, respectively. In the fourth, fifth, and sixth session 70% glycolic acid was applied for 1 min, 2 min, and 3 minutes, respectively. Skin was cleaned with spirit followed by acetone. Inner canthi of eye and nasolabial folds were protected with white vaseline. The peel was neutralized with sodium bicarbonate solution in water after the desired contact time or till erythema which ever was earlier. Sunscreen was advised after the peel.
In Group C, QSNYL (Med lite C6, Hoya Con Bio Inc., Fremont, CA, USA) at high fluence was performed at 2 weekly intervals (total of six sessions) at 532 nm, 4-mm SS, 2 Hz, gradual increase in fluence from 0.5 to 1 J/cm 2 for epidermal melasma. 1064-nm QSNYL, 6-mm SS, 2 Hz, gradual increase in fluence from 2 to 2.5 J/cm 2 for dermal and combination of both for mixed melasma. Both 532 and 1064 nm QSNYL was performed in the same session for mixed melasma. Mild erythema was taken as the endpoint.
Out of the seventy-five patients included, 21 patients in Group A, 19 patients in Group B, and 20 patients in Group C completed the study. Four patients in Group A, six patients in Group B, and five in Group C were unable to complete desired number of sessions of laser/peel. The possible causes of defaulting was difficult to ascertain, it might be due to side effects of treatment like erythema and burning, unsatisfactory response to treatment or other constraints to attend laser centre regularly to complete the treatment.
Evaluation of results of the sixty patients who completed the study was made on visual inspection and by comparing serial photographs taken at inclusion and after every laser/chemical peel session. Response to treatment in terms of reduction in area of pigmentation, intensity of pigment was performed using MASI score [Table - 1]. [12] MASI I (at baseline), MASI II (after 12 weeks), and MASI III (after 12 weeks follow up) was evaluated for all patients. Patients with no improvement or worsening were documented and immediate and late complications were recorded. Patients were also observed for side effects and recurrence in the 12 weeks follow-up period after completion of treatment.

Results
Out of the 60 patients who completed the study, there were 54 females and 6 males, M:F ratio was 1:9. The mean age of the patients was 34.05 ± 6.79 years. Minimum age was 21 years and maximum age was 48 years at the time of inclusion.
Most patients were in the age group 21-40 years. There were 19 patients in age group 21-30 years, 23 in age group 31-40 years, 5 in age group 41-50 years, and 3 were more than 50 years of age. There were 20 (33.33%) patients with photo type IV and 40 (66.7%) patients with photo type V. The age distribution and the skin photo types were comparable in all three groups. All the three groups were comparable with no statistically significant difference (P>0.05) based on the type of melasma. All the three groups were comparable with no statistically significant difference in the age distribution, skin photo type, and pattern of melasma.
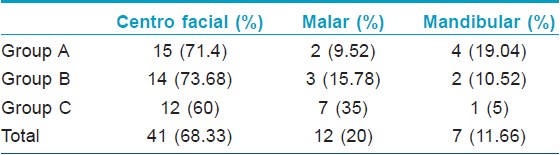
Centro facial melasma was the most common (68.33%), followed by malar (20%) and mandibular in 11.66% patients. The distribution of clinical pattern in each group is given in [Table - 2]. On Wood′s lamp examination, epidermal was most common type 28 (46.6%), closely followed by mixed in 27 (45%), and dermal in five (8.33%) patients. The distribution based on Wood′s lamp examination in each group is given in [Table - 3]. On histopathology, epidermal melasma was observed in 51.66% patients closely followed by mixed in 48.33%. The group vise distribution is given in [Table - 4]. Dermal melasma was not documented on histopathology since all dermal melasma patients on histopathology had some epidermal pigment. The positive predictive value for epidermal melasma was 90.32% and for mixed melasma was 93.1%.


Group A had a mean baseline MASI score (MASI I) 13.54 ± 7.19, Group B 10.78 ± 6.049, and Group C 10.57 ± 5.125. These were comparable with no statistically significant difference between the groups (P>0.05) using Anova test. After completion of treatment the mean MASI score (MASI II) in three groups was 7.050 ± 5.24 in Group A, 6.425 ± 5.0 in Group B, and 8.375 ± 4.177 in Group C [Table - 5]. All the three groups showed statistically significant improvement (P<0.05) at baseline and after treatment. The clinical improvement in Group A, B, C is shown in [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4], [Figure - 5] and [Figure - 6]. The improvement in the MASI score after therapy was maximum in Group A (low fluence laser) > Group B (glycolic acid peel) > Group C (high fluence laser). The improvement was statistically highly significant in Group A as compared to Group C (P<0.005), significant in Group A as compared to Group B (P<0.05), and in Group B when compared to Group C (P<0.05). Statistical analysis was done using ANOVA test.
 |
| Figure 1: Pre- (MASI=23) and post-treatment (MASI=9) clinical photograph after 12 sessions of low fluence QSNYL in melasma |
 |
| Figure 2: Pre- (MASI=9) and post-treatment (MASI=2.4) clinical photograph after 12 sessions of low fluence QSNYL in melasma |
 |
| Figure 3: Pre- (MASI=7.2) and post-treatment (MASI=2.4) clinical photograph after six sessions of glycolic acid peel in melasma |
 |
| Figure 4: Pre- (MASI=13.6) and post-treatment (MASI=3.6) clinical photograph after six sessions of glycolic acid peel in melasma |
 |
| Figure 5: Pre- (MASI=9.6) and post-treatment (MASI=4.2) clinical photograph after six sessions of high fluence QSNYL in melasma |
 |
| Figure 6: Pre- (MASI-6) and post-treatment (MASI=4.6) clinical photograph after six sessions of high fluence QSNYL in melasma |
 |
| Figure 7: Adverse effect: Clinical photograph at baseline, confetti like hypo-pigmentation followed by post-inflammatory hyperpigmentation in a patient after high-fluence QSNYL in melasma |

Immediate complications such as erythema, transient burning, and slight edema of the face after treatment, all of which were mild and disappeared within 1 h were seen in four (19.04%) patients administered high-fluence QSNYL. No immediate complications were observed in patients who received low fluence QSNYL. Transient erythema and burning was seen in 4 (21.05%) patients which disappeared within an hour in the glycolic acid peel group. In the follow up period of 12 weeks, mottled confetti like hypo pigmentation was seen in 5 (23.8%) patients in high fluence group and 1 patient in low fluence group. Two of the five patients who had mottled hypo pigmentation earlier after high fluence laser developed postinflammatory hyper pigmentation [Figure - 7]. Postinflammatory pigmentation was seen in only one (5.2%) patient in the glycolic peel group and six (28.5%) in high-fluence group. The adverse effects in each study group are given in [Table - 6]. No patient in the low-fluence group developed postinflammatory hyper pigmentation. Overall, fewer side effects were observed after low-fluence QSNYL treatment compared to high-fluence QSNYL.

However, at the end of the 12 weeks follow-up period, the mean MASI score increased in all the three groups. The mean MASI score in Group 1, Group 2, and Group 3 was 7.97 + 023, 7.24 + 36, and 9.4 + 76, respectively. When compared to MASI II, the percentage worsening in all groups was 13.04%, 13.125%, and 13.25%, respectively. This was almost similar in all the three groups with no statistical difference (P<0.05).
Discussion
Melasma is the most common hyperpigmentation disorder in Asians which is difficult to treat. Treatment of this condition accounts for a large fraction of aesthetic consultations. Even though total clearing may occur in up to 50% of cases with topical preparations such as Kligman′s formula, there are high rates of recurrence. [8] In the recent past, glycolic acid peels have been tried in various pigmentary disorders including melasma. Lasers have been evaluated only recently for the treatment of this condition. Most of the early studies have reported poor results and complications. [9],[10],[11]
QSNYL follow the principle of selective photo thermolysis and in doing so, limit the damage to the melanosome containing cell. However, there is existing lacunae in our knowledge regarding efficacy of glycolic acid and QSNYL (both high and low fluence) in melasma in Indian patients.
Most patients were in the age of 21-40 years which corroborated with the study by Javaheri et al., [13] which had a mean age of onset at 27.4 years. An earlier study in Caucasians reported the age of onset at 30 years. [14] Centrofacial melasma was the most common clinical type followed by malar and mandibular and this corroborates with other Indian studies. [13] On Wood′s lamp examination, accentuation of pigment was observed in 46.6% patients indicating its epidermal nature. However, on histopathology 51.66% patients had epidermal and 48.33% had mixed melasma. No dermal melasma was observed on histopathology. This is in partial agreement to a recent Indian study in which epidermal melasma was seen in 50% and mixed in 45% patients. [15]
The effectiveness of lasers in pigmented lesion is based on the principle of selective photothermolysis introduced by Anderson and Parish. When a specific wavelength of energy is delivered in a period of time shorter than the thermal relaxation time (TRT) of the target chromophore, heat energy is restricted to the target with less damage to the surrounding tissue. [16] Melanosomes of approximate size 0.5 to 1 micrometer in size have TRT of 50-500 ns whereas, melanocytes of approximate size 7 mm have TRT of several ms. Lasers with a wavelength well absorbed by melanin and pulse duration <1 ms effectively treat pigmented lesions with microscopic selectivity based on melanosome rupture. Immediate lightening of skin color after the laser pulses which fades gradually is consistent with formation and dissolution of gas bubbles due to laser induced cavitation. [16],[17] At the conventional parameters used to treat melasma, 532 nm for epidermal, and 532 nm and 1064 nm for dermal and mixed, the wavelength is absorbed not only by melanin but also by hemoglobin which may lead to formation of purpuric macules when the immediate white fades away. Purpuric macules on histology correlate with changes of erythrocyte coagulation (photo mechanical effect) within the superficial blood vessels. This damage leads to inflammation resulting in post inflammatory hyper pigmentation common in Asian skin and which also explains the non response and the rebound pigmentation seen after treatment with 532 nm QSNYL. [18] 1064 nm QSNYL has a longer wavelength (>600 nm), with added benefit of deeper skin penetration, is well absorbed by melanin and to a lesser extent by hemoglobin, making it safer in darker skin types because it spares injury to the epidermis to a greater degree than shorter wavelengths. However, in Asian skin, postinflammatory hyper pigmentation is common after 1,064-nm QSNDYL treatments. [16] Efficacy of 532 nm QSNYL is low due to purpuric effects (erythrocyte coagulation) resulting in inflammation and post inflammatory hyperpigmentation.
In a study by Polnikorn et al., two cases of long standing refractory dermal melasma responded to treatment with the Medlite C6 using once weekly treatment for 10 weeks with 1064-nm QSNYL at sub photothermolytic fluence (<5 J/cm 2), resulting in reduction of epidermal and dermal pigment with no recurrences at 1 year and 6 month follow-up, respectively. [19] In 2009, Cho et al., demonstrated that use of 1064 nm QSNYL with low pulse energy in 25 patients at 2 weekly intervals (2.5 J/cm 2 , 6-mm spot size, two passes with appropriate overlapping) as an effective treatment for melasma. [20] In 2010, Suh et al., in their study using 1064 nm QSNYL at 1-week interval for 10 weeks showed that it is a safe and effective modality for treating melasma in Asian patients. [21] By delivering repetitive energy with 1064 nm QSNYL at sub photothermolytic fluence using 6-8 mm spot size, melanin granules are fragmented and dispersed into cytoplasm. The total accumulative dose should be lower than the total toxic accumulative energy that will destroy cells which will lead to pigment lightening. Subsequent treatments at weekly intervals will lead to reduction of pigment. This reaction can be classified as biostimulation effect of QSNYL at subcellular level, without cell damage or death. On average, about 8-10 weekly treatments are required to reduce the hyperpigmentation so that it appears close to normal skin color. [22]
Glycolic acid interferes with the enzymes responsible for keratinocyte adhesion leading to its dysadhesion and exfoliation. [23] It causes thinning of stratum corneum, increase in epidermal hyaluronic acid, thickening of dermis associated with increase in glycosaminoglycans and collagen, dispersion of melanin and reversal of basal cell atypia. [24]
In our study, we observed both immediate complications and late onset hyper pigmentation with high fluence QSNDL, probably as a result of erythrocyte damage. Glycolic acid peels give good result with fewer complications. However, the best results with least adverse effects were observed with low fluence QSNYL.
There was a rise in the mean MASI score in all the three groups in the 12 weeks follow up period. Recurrence is expected in all groups, since treatment is not targeted to the cause, but for the lightening of the pigmentation in melasma as shown by the rise in MASI. This clearly shows that all the patients need maintenance therapy along with the use sunscreens to avoid recurrence.
Conclusion
This study shows the efficacy of low fluence QSNYL as well as glycolic acid peel in melasma with minimal side effects in type IV and V skin. Comparing the parameters of QSNYL used, 1064 nm QSNYL at low fluence at 0.5-1 J/cm2 with multiple passes repeated weekly is superior to QSNYL (at 532 and 1064 nm) at high fluence. This new technique of repetitive sub-threshold pulsed laser treatments at low fluence with the Med-Lite C6 laser is an effective modality for treating melasma.
However, in the absence of any maintenance therapy all the treatments had equal recurrence as shown by rise in MASI score. Thereby, treatment for melasma can only be effective when it is followed with a strict maintenance regimen in the absence of which recurrence is likely to occur.
| 1. |
Grimes PE. Melasma: Etiologic and therapeutic considerations. Arch Dermatol 1995;131:1453-7.
[Google Scholar]
|
| 2. |
Sanchez NP, Pathak MA, Sato S, Fitzpatrick TB, Sanchez JL, Mihm MC Jr. Melasma: A clinical, light microscopic, ultra structural, and immunofluorescence study. J Am Acad Dermatol 1981;4:698-710.
[Google Scholar]
|
| 3. |
Kang WH, Yoon KH, Lee ES, Kim J, Lee KB, Yim H, et al. Melasma: Histopathological characteristics in 56 Korean patients. Br J Dermatol 2002;146:228-37.
[Google Scholar]
|
| 4. |
Pasricha JS, Khaitan BK, Dash S. Pigmentary disorders in India. Dermatol Clin 2007;25:343-52.
[Google Scholar]
|
| 5. |
Vázquez M, Maldonado H, Benmamán C, Sánchez JL. Melasma in men: A clinical and histological study. Int J Dermatol 1988;27:25-7.
[Google Scholar]
|
| 6. |
Pérez M, Sánchez JL, Aguiló F. Endocrinologic profile of patients with idiopathic melasma. J Invest Dermatol 1983;81:543-5.
[Google Scholar]
|
| 7. |
Grimes PE, Yamada N, Bhawan J. Light microscopic, immunohistochemical and ultrastructural alteration in patients with melasma. Am J Dermatopath 2005;27:96-101.
[Google Scholar]
|
| 8. |
Gupta AK, Gover MD, Nouri K, Taylor S. The treatment of melasma: A review of clinical trials. J Am Acad Dermatol 2006;55:1048-65.
[Google Scholar]
|
| 9. |
Palumbo A, d'Ischia M, Misuraca G, Prota G. Mechanism of inhibition of melanogenesis by hydroquinone. Biochim Biophys Acta 1991;1073:85-90.
[Google Scholar]
|
| 10. |
Ferreira Cestari T, Hassun K, Sittart A, de Lourdes Viegas M. A comparison of triple combination cream and hydroquinone 4% cream for the treatment of moderate severe facial melasma. J Cosmet Dermatol 2007;6:36-9.
[Google Scholar]
|
| 11. |
Lipper GM, Anderson RR. Lasers in dermatology. In. Freedburg IM, Eisen AZ, Wolf Ketal, editors. Fitzpatrick dermatology in general medicine. 7 th ed. New York: McGraw Hill; 2007. p. 2508.
[Google Scholar]
|
| 12. |
Pandya A, Berneburg M, Ortonne JP, Picardo M. Guidelines for clinical trials in melasma: Pigmentation disorders academy. Br J Dermatol 2006;156:21-8.
[Google Scholar]
|
| 13. |
Javaheri SM, Handa S, Kaur I, Kumar B. Safety and efficacy of glycolic acid facial peel in Indian women with melasma. Int J Dermatol 2001;40:354-7.
[Google Scholar]
|
| 14. |
Griffiths CE, Finkel LJ, Ditre CM, Hamilton TA, Ellis CN, Voorhees JJ. Topical tretinoin (retinoic acid) improves melasma: A vehicle-controlled, clinical trial. Br J Dermatol 1993;129:415-21.
[Google Scholar]
|
| 15. |
Sarkar R, Puri P, Jain RK, Singh A, Desai A. Melasma in men: A clinical, aetiological and histological study. J Eur Acad Dermatol Venereol 2010;24:768-72.
[Google Scholar]
|
| 16. |
Anderson RR, Margolis RJ, Watenabe S, Flotte T, Hruza GJ, Dover JS. Selective photothermolysis of cutaneous pigmentation by Q-switched Nd:YAG laser pulses at 1064, 532, and 355 nm. J Invest Dermatol 1989;93:28-32.
[Google Scholar]
|
| 17. |
Kurban AK, Morrison PR, Trainor SW, Tan OT. Pulse duration effects on cutaneous pigment. Lasers Surg Med 1992;12:282-7.
[Google Scholar]
|
| 18. |
Polnikorn N, Tanrattanakorn S, Goldberg DJ. Treatment of Hori's nevus with the Q-switched Nd:YAG laser. Dermatol Surg 2000;26:477-80.
[Google Scholar]
|
| 19. |
Polnikorn N. Treatment of refractory dermal melasma with the MedLite C6 Q-switched Nd:YAG laser: Two case reports. J Cosmet Laser Ther 2008;10:167-73.
[Google Scholar]
|
| 20. |
Cho SB, Kim JS, Kim MJ. Melasma treatment in Korean women using a 1064-nm Q-switched Nd:YAG laser with low pulse energy. Clin Exp Dermatol 2009;34:e847-50.
[Google Scholar]
|
| 21. |
Suh KS, Sung JY, Roh HJ, Jeon YS, Kim YC, Kim ST. Efficacy of 1064 nm Q switched Nd:YAG Laser in melasma. J Dermatolog Treat;2011;22:233-8.
[Google Scholar]
|
| 22. |
Wattanakrai P, Mornchan R, Eimpunth S. Low-fluence Q-switched neodymium-doped yttrium aluminum garnet (1,064 nm) laser for the treatment of facial melasma in Asians. Dermatol Surg 2010;36:76-87.
[Google Scholar]
|
| 23. |
Khunger N. Glycolic acid peels. In: Khunger N, editor. Step by step chemical peels. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2009. p. 70-87.
[Google Scholar]
|
| 24. |
Behl DS, Tung R. Chemical peels. In: Alam M, Gladstone HB, Tung RC, editors. Requisites in dermatology: Cosmetic dermatology (Vol. 1). Edinburgh: Elsevier Limited; 2009. p. 81-101.
[Google Scholar]
|
Fulltext Views
7,232
PDF downloads
2,595





![[Table - 1]](#tbl_ijdvl_2012_78_2_165_93633_t1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2012_78_2_165_93633_t2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2012_78_2_165_93633_t3.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2012_78_2_165_93633_t4.jpg){kind=link}
![[Table - 5]](#tbl_ijdvl_2012_78_2_165_93633_t5.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2012_78_2_165_93633_f7.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_2_165_93633_f8.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_2_165_93633_f9.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2012_78_2_165_93633_f10.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2012_78_2_165_93633_f11.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2012_78_2_165_93633_f12.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2012_78_2_165_93633_f13.jpg){kind=link}
![[Table - 6]](#tbl_ijdvl_2012_78_2_165_93633_t6.jpg){kind=link}