Translate this page into:
A rare case of metastatic skin tumors originating from the sarcomatous component of lung carcinosarcoma
Correspondence Address:
Yuka Takashima
Department of Dermatology, Sapporo City General Hospital, North 11 West 3, Sapporo 060-8604
Japan
| How to cite this article: Takashima Y, Moriuchi R, Shirato T, Shimizu S. A rare case of metastatic skin tumors originating from the sarcomatous component of lung carcinosarcoma. Indian J Dermatol Venereol Leprol 2019;85:201-203 |
Sir,
Carcinosarcomas are rare malignancies that are defined as biphasic tumors composed of two intimately intermingled carcinomatous and sarcomatous components. Carcinosarcomas can arise in various parts of the body, including the uterus, ovaries, bladder, breasts, lungs and larynx. They are highly aggressive tumors with an average 5-year survival rate of 26–34%. Skin metastases of carcinosarcomas are extremely rare;[1] with the metastatic lesions most commonly occurring in the peritoneum, lung and bone.[2],[3] Here, we report a rare case of cutaneous metastases arising from lung carcinosarcoma.
An 80-year-old Japanese man was referred to our hospital with hard nodules on the second to fourth fingers of the right hand, noted since 1-month. Physical examination revealed hard skin coloured to reddish nodules on the right second to fourth fingers of the right hand and on the left side of the forehead [Figure - 1]a and [Figure - 1]b. The nodules on the right fingers were up to 5 mm in diameter and the nodule on the left side of the forehead measured 15 × 5 mm. The differential diagnoses included primary extraskeletal chondrosarcoma, fibro-osseous pseudotumor of the digit and ossifying fibromyxoid tumor. A skin biopsy specimen from the digit showed dermal nodular proliferation of atypical chondrocyte-like cells, which was consistent with the findings of chondrosarcoma [Figure - 2]a and [Figure - 2]b. Detailed medical history revealed that the patient had undergone video-assisted thoracoscopic surgery for a right upper lobe lung tumor, 4 months before the digital lesions appeared. The lung tumor specimen showed a biphasic pattern consisting of atypical squamoid cells which were positive for CK5/6 and atypical chondrocyte-like cells [Figure - 2]c, [Figure - 2]d, [Figure - 2]e, [Figure - 2]f. The morphological features of the chondrocyte-like cells in the lung lesion were identical to those of the digital tumor cells and intravascular invasion by atypical chondrocyte-like cells was seen in the lung lesion. In addition, more than one tumor appeared in the fingers at the same time. Taking into account these factors, we made the final diagnosis of metastatic cutaneous deposits originating from the sarcomatous component of lung carcinosarcoma.
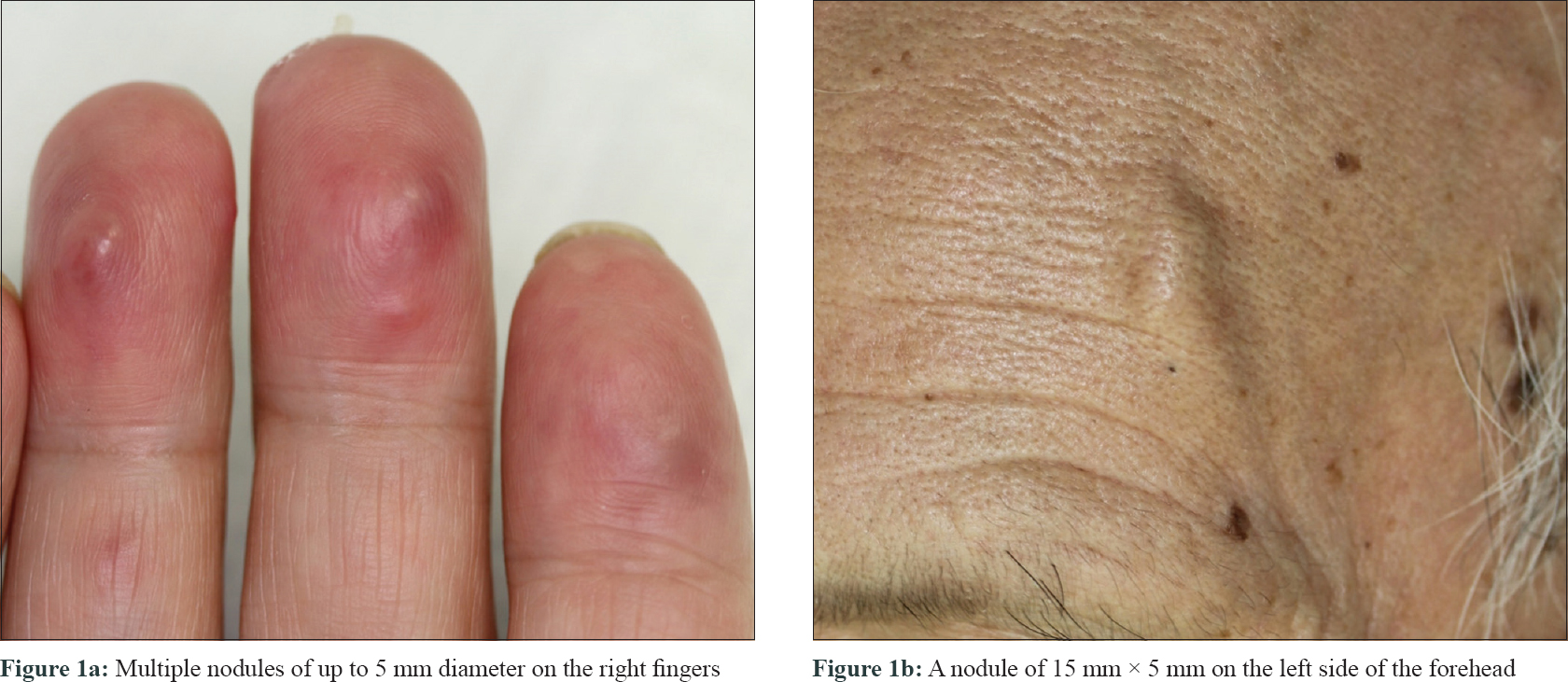 |
| Figure 1: |
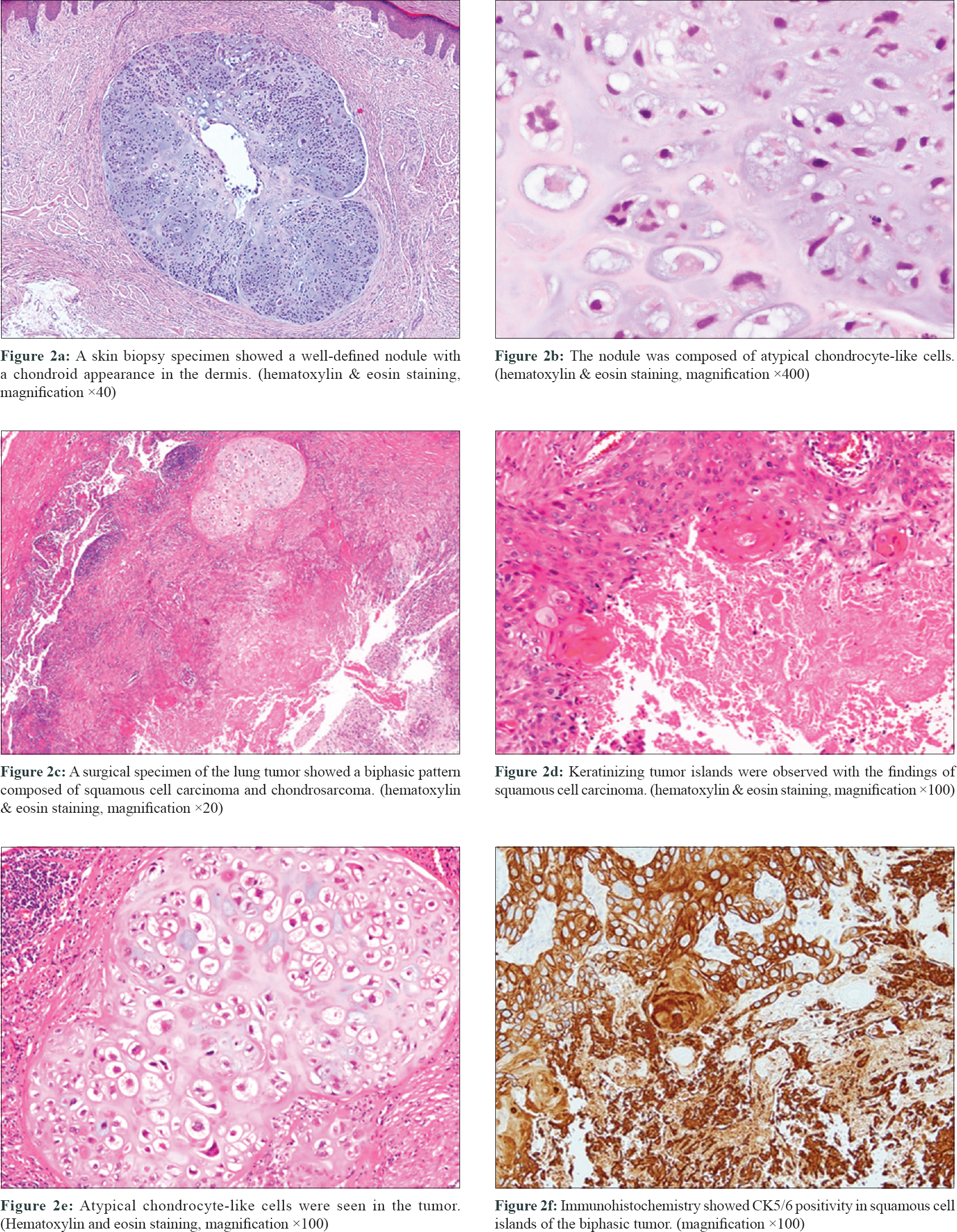 |
| Figure 2: |
Cutaneous metastases of carcinosarcoma are extremely rare. A PubMed search identified only 42 cases of metastatic carcinosarcoma. Of these, only three of the cases with pathological proof of both metastatic lesions and primary lesions had metastatic skin lesions. The primary lesions of these three cases were in the uterus, lung and rectum.[4] We were unable to find any previous reports of multiple metastases to the distal extremities and this is the striking feature in this case.
Several theories have been proposed regarding the histogenesis of carcinosarcoma. Recent studies support the “combination theory,” as molecular genetic testing has shown carcinomatous and sarcomatous components to share the same features.[2] The combination theory suggests that both components originate from a common pluripotent stem cell that undergoes divergent differentiation.
It has been reported that the carcinomatous component of the primary carcinosarcoma most commonly has features of squamous cell carcinoma or adenocarcinoma,[5] whereas the sarcomatous component is usually chondrosarcoma.[4] The majority of the metastases in the 42 cases of metastatic carcinosarcoma were found to be composed of a single component: 30 of the 42 cases were composed of a purely carcinomatous component and five were composed of a purely sarcomatous component.[3],[4],[6] Only seven were composed of a mixture of carcinoma and sarcoma. In our case, the primary lesion in the lung was composed of squamous cell carcinoma and chondrosarcoma, and the metastatic skin lesion on the finger was composed of pure chondrosarcoma.
The primary treatment of carcinosarcoma is surgery. Some adjuvant treatment modalities have been reported, including radiation therapy and/or chemotherapy with cisplatin and epirubicin. However, no regimen of adjuvant treatment has been established.[7] Considering this situation and the patient's advanced age, we did not add adjuvant treatment for the present case.
To conclude, we describe a case of skin metastases from lung carcinosarcoma. As the metastatic lesions of carcinosarcoma can show a carcinomatous component, a sarcomatous component, or a mixture of those, it is often difficult to make an accurate diagnosis. When dermatologists encounter metastatic chondrosarcoma as in the present case, they should consider the possibility of the existence of primary carcinosarcoma.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that the name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Terada T. Sarcomatoid carcinoma of the lung presenting as a cutaneous metastasis. J Cutan Pathol 2010;37:482-5.
[Google Scholar]
|
| 2. |
Loh TL, Tomlinson J, Chin R, Eslick GD. Cutaneous carcinosarcoma with metastasis to the parotid gland. Case Rep Otolaryngol 2014;2014:173235.
[Google Scholar]
|
| 3. |
Clairwood M, Yasuda M, Belazarian L, Deng A. Unusual cutaneous metastasis of uterine carcinosarcoma: A case report and review of the literature. Am J Dermatopathol 2016;38:366-9.
[Google Scholar]
|
| 4. |
Kiuru M, McDermott G, Coit DC, Berger MF, Busam KJ. Basal cell carcinosarcoma with PTCH1 mutations in both epithelial and sarcomatoid primary tumor components and in the sarcomatoid metastasis. Am J Surg Pathol 2014;38:138-42.
[Google Scholar]
|
| 5. |
Gao S, Huang L, Dai S, Chen D, Dai R, Shan Y. Carcinosarcoma of the gallbladder: A case report and review of the literature. Int J Clin Exp Pathol 2015;8:7464-9.
[Google Scholar]
|
| 6. |
Lau PP, Ting SH, Ip YT, Tsang WY, Chan JK. Merkel cell carcinosarcoma: Merkel cell carcinoma with embryonal rhabdomyosarcoma-like component. Ann Diagn Pathol 2012;16:388-91.
[Google Scholar]
|
| 7. |
Singh R. Review literature on uterine carcinosarcoma. J Cancer Res Ther 2014;10:461-8.
[Google Scholar]
|
Fulltext Views
3,185
PDF downloads
2,595





![[Figure - 1]](#fig_ijdvl_2019_85_2_201_251383_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_2_201_251383_f2.jpg){kind=link}