
Translate this page into:
A rare case of scrub typhus vasculitis presenting as acute coronary syndrome diagnosed by skin manifestations
Corresponding author: Dr. Biju Vasudevan, Department of Dermatology, Base Hospital, Lucknow, Uttar Pradesh, India. bijuvasudevan1975@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Pradeesh A, Vasudevan B, Sharma N, Verma R. A rare case of scrub typhus vasculitis presenting as acute coronary syndrome diagnosed by skin manifestations. Indian J Dermatol Venereol Leprol 2022;88:184-7.
Abstract
A 48-year-old diabetic man presented with complaints of acute onset chest heaviness with palpitations, anxiety and headache. He had raised troponin-T level and electrocardiogram showed ST elevation myocardial infarction. There was a prior history of fever of 4 days duration with associated abdominal pain. He later developed skin rash and neurological symptoms following admission to the hospital. Dermatological examination revealed purpura and a livedo-like rash. Investigations revealed deranged liver and renal function tests and positive serological tests for scrub typhus. Coronary angiography revealed no evidence of atherosclerosis or any other pathology. He was therefore diagnosed as a case of scrub typhus-induced vasculitis with coronary manifestations and was managed with oral doxycycline. Scrub typhus presenting like an acute coronary syndrome has been reported very rarely previously. In addition, patient had gastrointestinal, central nervous system and hematological involvement which added to the rarity of the case.
Keywords
Myocardial infarction
rickettsia
scrub typhus
vasculitis

Introduction
Scrub typhus disease is a febrile illness caused by bacteria of the family Rickettsiaceae, with the culprit organism being Orientia tsutsugamushi. It has been found to be endemic in the subHimalayan region of India.1 The chief target of the organism is the vascular endothelium of various organs and affects skeletal muscles, skin, lungs, kidneys, brain, intestine and cardiac muscles. Based on the organ affected, patient can present with myalgia, purpuric rash, cough, seizures, altered sensorium, loose stools, vomiting or chest pain. An exceedingly rare case of scrub typhus vasculitis presenting as an acute coronary syndrome is being reported.
Case Report
A 48-year-old man presented to the hospital with complaints of acute onset chest heaviness with palpitations, anxiety and headache of about 36 h duration. His initial clinical examination revealed: blood pressure 150/90 mmHg, respiratory rate 30/min, pulse rate 100/min, normal jugular venous pressure and bilateral basal crepitations. On echocardiography, there was reduced ejection fraction (30%), regional anterior wall motion abnormality and electrocardiogram showed Q wave in V1-V4, ST elevation in V1-V4 and T inversion in aVL and V4-V5 leads [Figure 1]. Troponin-T was raised (46.44 ng/ml with reference range: <0.01 ng/ml) and creatine kinase-MB was negative. He was diagnosed with anterior wall myocardial infarction and was managed conservatively. He continued to be symptomatic with chest pain despite the above treatment.
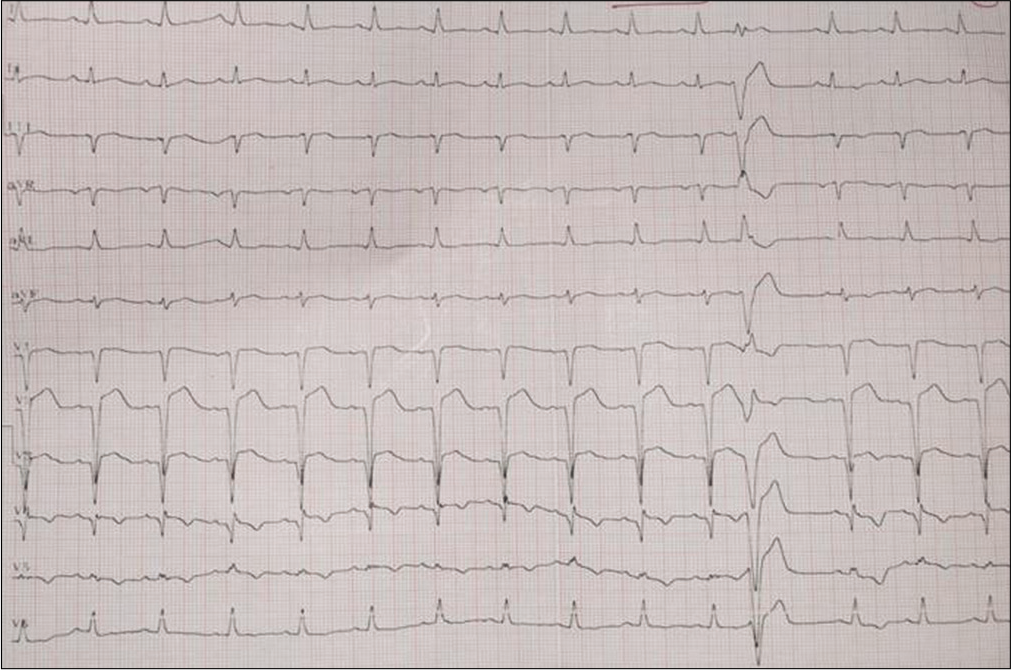
- ST elevation myocardial infarction in anterior wall
On further enquiry, he had a history of fever of acute onset, about 4 days prior to onset of chest heaviness, which was high grade, intermittent, associated with chills and myalgia. In addition, he had diffuse periumbilical pain with no bowel or bladder disturbance. After 24 h of admission, he developed painful skin rash over hands and feet which spread to the whole body with associated redness of eyes and pain in the small joints. He also developed acute onset altered sensorium, irrelevant behavior and restlessness.
Dermatological examination revealed generalized maculopapular rash [Figure 2], retiform purpura over lower limbs and forearms [Figures 3 and 4] and annular purpuric lesions over dorsum of hands and feet [Figures 5 and 6]. He also gave a history of working in the nearby forest for the last 3 months. With a suspicion of rickettsiosis based on the retiform purpura, skin biopsy was done and relevant tests were ordered.

- Maculopapular rash with a reticular pattern on trunk

- Retiform purpura on thighs

- Reticular pattern of purpura on forearms

- Annular purpuric lesions on dorsum of hands

- Annular morphology better seen on anterior aspect of ankle
Investigations revealed normal blood counts except for thrombocytopenia (68,000/µl). Serum bilirubin was 1.5 mg%, serum glutamic-oxaloacetic transaminase: 446 IU/L, serum glutamic-pyruvic transaminase: 510 IU/L, gamma glutamyl transferase: 132 IU/L and alkaline phosphatase: 247 IU/L. He also had raised blood urea (55 mg/dL) and serum creatinine (1.5 mg/dL) levels. Computed tomography scan of the abdomen revealed hepatomegaly and mild stenosis of superior mesenteric artery. Noncontrast computerized tomography of brain and cerebrospinal fluid analysis was normal. Antibodies to rickettsial OXK antigen were significantly positive at 1:320 titers and he was positive for IgM against scrub typhus. He was given oral doxycycline 100 mg twice daily with which his rash, cardiac and neurological symptoms and liver and kidney functions improved drastically. The histopathology of skin biopsy done from purpura was suggestive of small vessel vasculitis [Figure 7]. Coronary angiography revealed no evidence of atherosclerosis or any other underlying pathology. The titers of antibodies against rickettsial antigens also fell after treatment and became negative later.
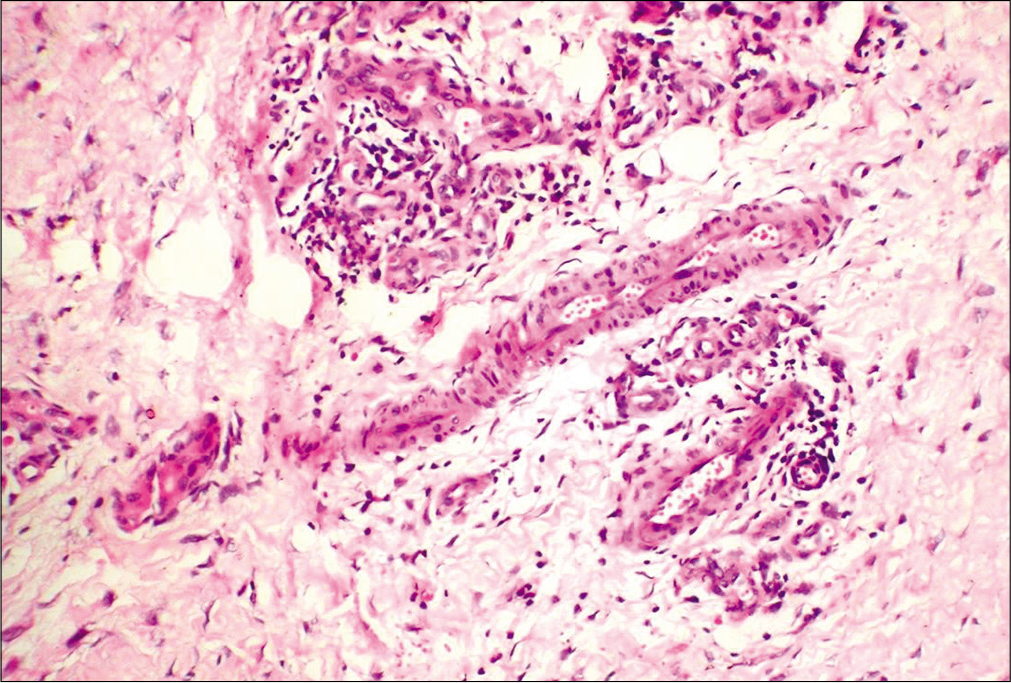
- Features of vasculitis: fibrinoid necrosis and leukocytoclasis (H and E,×40)
Discussion
In scrub typhus infections, the primary reservoir is a trombiculid mite, while the secondary reservoirs are mainly rodents and humans. Man is an accidental host and incubation period is 5–20 days with a mean of 10–12 days. Orientia tsutsugamushi, the causative agent, is transmitted to humans through bite of the trombiculid mites.
Scrub typhus produces a vasculitis response and can affect any system of the body. In a study by Griffith et al., 85.2% scrub typhus patients had dysfunction of 3 or more organ systems.2 Our patient had skin, cardiac, central nervous system, liver, kidney, gastrointestinal and hematological involvement.
Cardiac involvement is rarely reported in rickettsial infections. R. conorii related cardiac involvement is reported in about 6 cases previously.3 Acute coronary syndrome has been also described as a sequela to rickettsial infection.4,5 Chronic cardiac involvements like relative bradycardia, electrocardiographic changes, cardiomegaly, myocarditis, pericarditis, cardiogenic shock and heart failure are also reported in a few cases.6 We could find one previous report of scrub typhus manifesting as myocardial infarction.7
Our case in addition to manifesting as acute coronary syndrome had the following additional features: (i) multisystem involvement (skin, liver, kidney, gastrointestinal, central nervous system and hematological) which is more common with Indian tick typhus infection than in scrub typhus, (ii) diagnosis suspected due to the type of retiform purpura, (iii) presentation of scrub typhus without an eschar and (iv) clinical improvement in all organs and laboratory parameters with doxycycline. Raised troponin-T and normal creatine kinase-MB levels with normal coronaries helped us confirm the diagnosis of rickettsial cardiac involvement.8 Liver involvement in the form of raised bilirubin and enzymes, raised blood urea and creatinine pointing to kidney involvement, superior mesenteric artery block as abdominal involvement, altered sensorium in central nervous system and thrombocytopenia made it a truly global systemic involvement which is rarely seen. Raised bilirubin has been reported as a marker for severe systemic involvement previously.9
Hence, in a case of retiform purpura manifesting as acute coronary syndrome and multisystem involvement, we need to keep scrub typhus as a possible diagnosis and doxycycline needs to be administered at the earliest to prevent complications and mortality.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Emerging and re-emerging bacterial diseases in India. J Biosci. 2008;33:549-55.
- [CrossRef] [PubMed] [Google Scholar]
- Profile of organ dysfunction and predictors of mortality in severe scrub typhus infection requiring intensive care admission. Indian Soc Crit Care Med. 2014;18:497-502.
- [CrossRef] [PubMed] [Google Scholar]
- Myocarditis in mediterranean spotted fever: A case report and a review of the literature. JMM Case Rep. 2016;3:e005039.
- [CrossRef] [PubMed] [Google Scholar]
- Scrub typhus increases the risk of developing acute coronary syndrome: A nationwide cohort study. Heart. 2014;100:1844-50.
- [CrossRef] [PubMed] [Google Scholar]
- Acute myocardial infarction following scrub typhus infection. Int J Cardiol. 2007;114:e18-20.
- [CrossRef] [PubMed] [Google Scholar]
- Scrub typhus presenting as acute myocardial infarction. Online J Health Allied Sci. 2012;11:11.
- [Google Scholar]
- Pericarditis due to Tsutsugamushi disease. Scand J Infect Dis. 2000;32:101-2.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiac troponin T in patients with clinically suspected myocarditis. J Am Coll Cardiol. 1997;30:1354-9.
- [CrossRef] [Google Scholar]
- Predictors of acute myocarditis in complicated scrub typhus: An endemic province in the Republic of Korea. Korean J Intern Med. 2018;33:323-30.
- [CrossRef] [PubMed] [Google Scholar]




