Translate this page into:
Adapalene pretreatment increases follicular penetration of clindamycin: In vitro and in vivo studies
Correspondence Address:
Gaurav K Jain
Department of Pharmaceutics, F/O Pharmacy, Jamia Hamdard, Hamdard Nagar, New Delhi - 110 062
India
| How to cite this article: Jain GK, Ahmed FJ. Adapalene pretreatment increases follicular penetration of clindamycin: In vitro and in vivo studies. Indian J Dermatol Venereol Leprol 2007;73:326-329 |
Abstract
Background: Topical retinoids normalize desquamation, reduce comedogenesis and may enhance the penetration of other topicals providing more effective treatment of acne. Aim: We evaluated the effect of adapalene on skin penetration of clindamycin phosphate when it is applied concomitantly or after various time durations following adapalene application. Methods: The in vitro studies were carried out using excised rat skin, whereas the in vivo studies were conducted on healthy human volunteers. Radioactive clindamycin phosphate (1%) gel was applied to rat skin sections and to the hands of human volunteers concomitantly and after the pretreatment of the skin for 3, 5 and 10 min with 10 mg of adapalene (0.1%) gel. Quantification of clindamycin phosphate was performed by liquid scintillation. Results: In vitro skin penetration and distribution of clindamycin phosphate was affected by the pretreatment time. Significantly higher skin concentration of clindamycin phosphate (15.5%) with largest proportion in viable skin layer (9.4% of applied dose) was found when clindamycin phosphate gel was applied after the pretreatment of the skin with adapalene gel for 5 min. Further increase in pretreatment time has no additive influence on the penetration of clindamycin phosphate. In vivo results were in corroboration with the in vitro results and demonstrate significantly higher concentration of clindamycin phosphate (19%) in the skin following pretreatment with adapalene gel for 5 min. Adapalene acts as a penetration enhancer and increases the penetration of topical clindamycin phosphate. Conclusion: Application of clindamycin phosphate gel after the pretreatment of skin with adapalene gel for 5 min may contribute significantly to the increased efficacy of therapy.
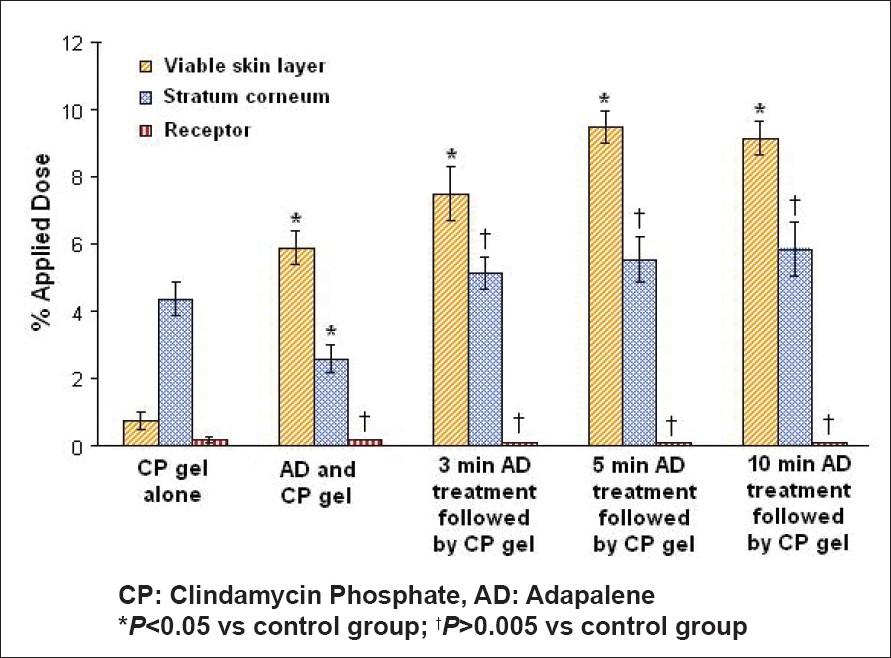 |
| Figure 2: Effect of adapalene on the skin distribution profile of clindamycin phosphate |
|
| Figure 2: Effect of adapalene on the skin distribution profile of clindamycin phosphate |
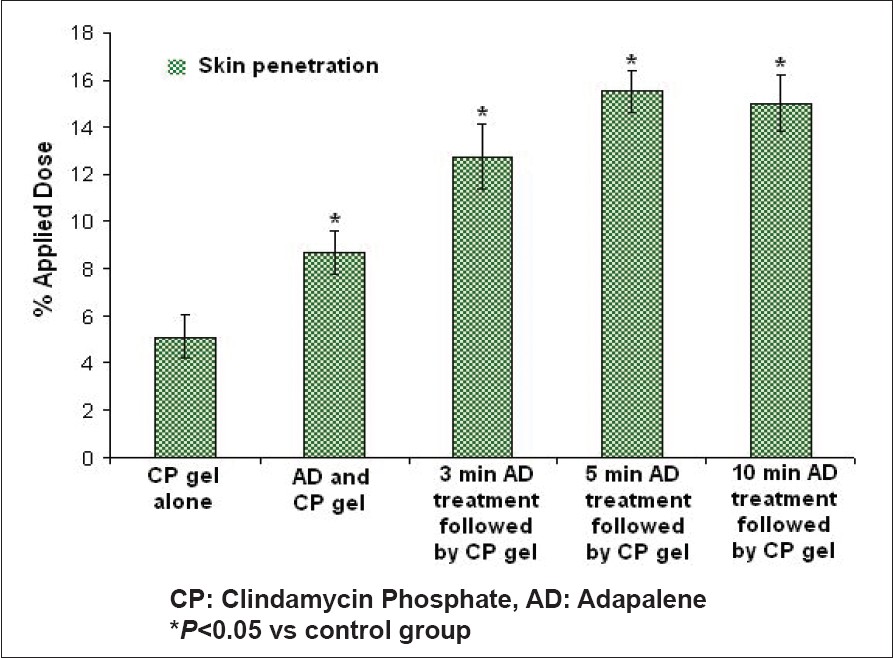 |
| Figure 1: Effect of adapalene on the skin penetration profile of clindamycin phosphate |
|
| Figure 1: Effect of adapalene on the skin penetration profile of clindamycin phosphate |
Introduction
In the clinical management of acne vulgaris, a considerable number of topical and/or systemic treatment modalities are available to the physician. The combination of a topical antibiotic with a topical retinoid is a rational choice because of their distinct, complementary and additive mechanism of action. Topical retinoids have a dual mechanism of action. They possess a strong anticomedogenic effect and are effective against inflammatory acne lesions. [1] Topically applied retinoids are an integral component of combination therapy for acne vulgaris because they promote comedonal drainage, which facilitates the penetration of other topical agents through the follicular pathway. [2],[3]
Clinical experience has shown that adapalene, a new topical retinoid, has a superior cutaneous safety profile and could be used in combination with other topical agents without any significant additive irritant effect. [4] Mechanistically, adapalene binds to specific retinoic acid nuclear receptors and normalizes the differentiation of follicular epithelial cells resulting in decreased microcomedone formation. [5],[6] Topical antibiotics such as clindamycin reduces Propionibacterium acnes count and inhibits the inflammation caused by the bacteria. [7] However, clindamycin phosphate is less effective because of its low solubility and consequent difficulty in penetrating the sebum-filled follicles. [8] Some percutaneous absorption may also occur with clindamycin phosphate, resulting in diarrhea and colitis. [9] In the present study, the effect of adapalene (when applied concomitantly or after a time duration) on the follicular penetration of clindamycin phosphate is evaluated.
Methods
The study was conducted in accordance with the ethical principles originating from the Declaration of Helsinki and Good Clinical Practice. The study protocol was reviewed and approved by the institutional review board. Research on animals (rats) for this study is approved by CPCSEA (Committee for the purpose of control and supervision of experiments on animals).
Adapalene gel and clindamycin phosphate (CP) were obtained from Galderma India Pvt. Ltd. Pertechnetate was obtained from Bhabha Atomic Research Centre, India.
Preparation of radioactive clindamycin phosphate (1%) gel
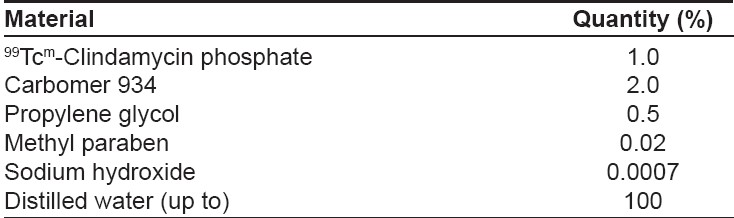
Carbopol 934 was added in small amounts to approximately 90% of the water phase used in the final product. While stirring, 99 Tc m -pertechnetate labeled clindamycin phosphate and a 10% solution of methyl paraben in ethanol was added along with triethanolamine. The final volume of the gel (clindamycin phosphate, 1%) was adjusted using water. The composition of clindamycin phosphate (1%) gel is shown in [Table - 1].
Preparation of rat skin
Six (6) male albino rats were used for the preparation of skin. Care of the rats was in accordance with institutional guidelines. The rats were killed by cervical dislocation. Dorsal hair was removed with an electrical clipper and full-thickness skin was surgically removed from each rat. To assure the integrity of each skin section, its permeability to tritiated water was determined before the application of sample.
In vitro skin penetration and distribution studies
The in vitro skin penetration and distribution profile was assessed using modified Franz diffusion cell. After removal of subcutaneous fat, circular specimens of full-thickness skin were placed in static diffusion cells. The dermal side of the skin was in contact with aqueous receptor phase (phosphate buffered saline; pH 6.4). The receptor phase was stirred constantly with a spinning bar magnet to ensure proper mixing. To separate the skin sections, radiolabeled clindamycin phosphate gel at a target dose of 5mg/dose/cm 2 was applied concomitantly and after pre-treatment of skin sections for 3, 5 and 10min with 10mg of adapalene gel per cm 2 . Radiolabeled clindamycin phosphate gel was also applied alone to serve as control. The procedure was carried out at 37°C with thermostatically controlled water circulating in the external water jacket of the diffusion cell. At the end of the application period (12h), the entire dosing area of skin was collected, washed and wiped properly and clindamycin was quantified in the skin compartments and in the receptor fluid by using a liquid scintillation counter.
In vivo scintigraphic studies in human volunteers
A total of 30 healthy male volunteers (age: 25 ± 5 years), were enrolled in the study. Subjects with abnormal skin hyperpigmentation, a history of skin disease or known sensitivity to skin care products were excluded from the study. Use of any systemic drug and/or topical drug on the application area within one week before beginning the protocol was not permitted. Radiolabeled clindamycin phosphate gel at a target dose of 5mg/dose/cm 2 was applied concomitantly to the hand of healthy human volunteers and after pre-treatment of the skin for 3, 5 and 10 min with 10 mg of adapalene gel per cm 2 . In each case, the control was the other hand applied with radiolabeled clindamycin phosphate gel alone. Two hours later, hands were covered with protective dressings. At the end of the application period (12h), all the residual nonabsorbed radioactive material on the skin surface was carefully washed and recovered. Unabsorbed clindamycin phosphate was quantified using liquid scintillation and clindamycin phosphate that was retained in the skin and permeating to the systemic circulation was determined by using a gamma camera. After completion of the study, subjects were monitored up to one week for skin irritation, adverse effects or any systemic effects.
Statistical analysis
The results were analyzed by student′s t-test using Sigma Stat software (version 3.5). A difference below the probability level of 0.05 ( P < 0.05) was considered to be statistically significant.
Results
In vitro skin penetration and distribution studies
In vitro skin retention measurements and skin distribution profile of radiolabeled clindamycin phosphate were performed to investigate the role of topical adapalene on transdermal uptake of clindamycin phosphate. [Figure - 1] clearly demonstrates that adapalene acts as a penetration enhancer and increases the penetration of clindamycin phosphate into the rat skin. When clindamycin phosphate gel was applied alone, only 5.13% of radioactive clindamycin phosphate penetrated into the skin. The highest proportion of the total amount recovered in the whole skin (4.3% of the applied dose) was found in stratum corneum [Figure - 2]. The concomitant application of adapalene gel increases the penetration of clindamycin phosphate to 8.7%. Moreover, a significantly higher concentration of clindamycin phosphate (5.9% of the applied dose, P< 0.05) was observed in the viable skin layers. [Figure - 1],[Figure - 2] also demonstrate that both the amount and depth of penetration of clindamycin phosphate appeared to be related to the pretreatment time of skin with adapalene gel. The pretreatment of skin with adapalene gel for 3 and 5 min prior to application of clindamycin gel significantly increases the penetration of clindamycin phosphate to 12.75 and 15.5% respectively ( P< 0.05). A higher proportion of clindamycin phosphate (7.5 and 9.4% of the applied dose) was found in the viable skin layers after the pretreatment of the skin with adapalene gel for 3 and 5 min respectively. Furthermore, despite the numerical differences, no statistically significant difference on skin penetration of clindamycin phosphate was observed with an increase in the pretreatment time from 5 to 10 min. Only modest amounts of radioactive clindamycin phosphate permeated to the receptor phase from all the formulations [Figure - 2].
In vivo scintigraphic studies in human volunteers
As shown in [Table - 2], adapalene increases the penetration of clindamycin phosphate. Significantly higher concentrations of clindamycin phosphate (19%) in skin were achieved following the pretreatment of skin with adapalene for 5 min as compared to the control (7.2%, P< 0.05). No radioactivity was detected in urine and feces albeit the detection limits were high, indicating a minimal systemic exposure. On visualizing the skin scans it appears that pretreatment of skin with adapalene gives higher clindamycin concentration at the intended site of action, thereby enhancing the localized effects. None of the volunteers in either treatment group experienced any local and systemic adverse reactions (pseudomembranous colitis and diarrhea).
Discussion
The stratum corneum is a major barrier for penetration of topical antibiotics such as clindamycin into and through the skin. Generally, sebaceous glands release sebum into follicular canal creating lipoidal environment and restricting the follicular penetration of clindamycin phosphate. [10] Application of clindamycin phosphate gel alone (control) shows the low penetration of clindamycin phosphate in skin because of the presence of stratum corneum and the restricted follicular penetration. Owing to higher lipophilicity (log P : 7.884) and its desirable particle size (3-10 mm), from its gel formulation, adapalene selectively penetrates into the follicular ducts and pilosebaceous units. [4] In addition, adapalene modulates keratinization and draws out sebum from the follicular shunts. [11] The concomitant application or the pretreatment of skin with adapalene gel promotes comedonal drainage that allows the follicle to function as rapid transport shunts and permit high concentrations of clindamycin phosphate to bypass the continuous stratum corneum and readily reach the deeper viable skin layers. The microcrystals of adapalene rapidly distributes in the upper part of follicular duct within 3-5 min of topical application of the adapalene 0.1% gel; therefore, the pretreatment of skin with adapalene gel for 5 min prior to application of clindamycin gel significantly increases the penetration of clindamycin phosphate. [4] Moreover, when adapalene gel is applied concomitantly with clindamycin phosphate gel, its effect may get diluted as the whole of adapalene does not come in contact with skin.
Data also suggest that the systemic exposure to clindamycin following the topical application of adapalene is negligible and comparable to or less than that observed after the topical application of the clindamycin phosphate gel alone. Interestingly, the pretreatment of skin with adapalene gel significantly increases the skin penetration of clindamycin phosphate without appreciable increase in its permeation. With the abovementioned understanding, it could be theorized that adapalene pretreatment delivers higher concentrations of clindamycin phosphate to the follicular ducts and pilosebaceous units. It is possible that the localization of the drug in viable skin layers prevents the active drug from permeating into the systemic circulation. It may be conjectured that once within the pilosebaceous unit, it is likely that clindamycin will dissolve into the sebum resulting in low systemic permeation. Furthermore, the in vivo and in vitro results are in corroboration with each other. The small variations are attributed to difference in skin type, site of application and difference in follicular density.
As shown in this study, the characteristic property of adapalene to enhance the penetration of clindamycin phosphate into skin makes it a good choice as a therapy in combination with clindamycin phosphate for the treatment of acne. Adapalene increases the follicular penetration of clindamycin phosphate, thereby enhancing its localization in the skin. The application of clindamycin phosphate gel after the pretreatment of skin with adapalene gel for 5 min may contribute significantly to the increased efficacy of therapy.
Acknowledgement
We would like to thank Galderma India Pvt. Ltd. for providing financial support for this work. We would also like to thank Dr. A. Bhatnagar, Department of Nuclear Medicine, INMAAS, Delhi, for his helpful comments and advice during the gamma scintigraphic studies.
| 1. |
Cunliffe WJ, Caputo R, Dreno B, Forstrom L, Heenen M, Orfanos CE, et al . Efficacy and safety comparisons of adapalene (CD271) gel and tretinoin gel in the topical treatment of acne vulgaris. A European multicentre trial. J Dermatol Treat 1997;8:173-8.
[Google Scholar]
|
| 2. |
Thiboutot D. New treatments and therapeutic strategies for acne. Arch Fam Med 2000;9:179-87.
[Google Scholar]
|
| 3. |
Dreno B. Topical antibacterial therapy for acne vulgaris. Drugs 2004;64:2389-97.
[Google Scholar]
|
| 4. |
Ellis CN, Gammon WR, Stone DZ, Heezen-Wehner JL. A comparison of Cleocin T Solution, Cleocin T Gel, and placebo in the treatment of acne vulgaris. Cutis 1998;42:245-7.
[Google Scholar]
|
| 5. |
Gollnick HP, Krautheim A. Topical treatment in acne: Current status and future aspects. Dermatology 2003;206:29-36.
[Google Scholar]
|
| 6. |
Waugh J, Noble S, Scott LJ. Adapalene: A review of its use in the treatment of acne vulgaris. Drugs 2004;64:1465-78.
[Google Scholar]
|
| 7. |
Toyoda M, Morohashi M. An overview of topical antibiotics for acne treatment. Dermatology 1998;196:130-4.
[Google Scholar]
|
| 8. |
Akhavan A, Bershad S. Topical acne drugs: Review of clinical properties, systemic exposure and safety. Am J Clin Dermatol 2003;4:473-92.
[Google Scholar]
|
| 9. |
van Hoogdalem EJ. Transdermal absorption of topical anti-acne agents in man: Review of clinical pharmacokinetic data. J Eur Acad Dermatol Venereol 1998;11:S13-9.
[Google Scholar]
|
| 10. |
Meidan VM, Bonner MC, Michniak BB. Transfollicular drug delivery-is it a reality? Int J Pharm 2005;306:1-14.
[Google Scholar]
|
| 11. |
Shroot B, Michel S. Pharmacology and chemistry of adapalene. J Am Acad Dermatol 1997;36:S96-103.
[Google Scholar]
|
Fulltext Views
3,020
PDF downloads
1,125





![[Table - 1]](#tbl_ijdvl_2007_73_5_326_34010_1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2007_73_5_326_34010_2.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_5_326_34010_3.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2007_73_5_326_34010_4.jpg){kind=link}