Translate this page into:
An open randomized comparative study to test the efficacy and safety of oral terbinafine pulse as a monotherapy and in combination with topical ciclopirox olamine 8% or topical amorolfine hydrochloride 5% in the treatment of onychomycosis
2 Department of Microbiology, C. C. S University, Meerut, Uttar Pradesh, India
Correspondence Address:
R P Sharma
Department of Dermatology and STD, L. L. R. M. Medical College, Meerut, Uttar Pradesh - 250 005
India
| How to cite this article: Jaiswal A, Sharma R P, Garg A P. An open randomized comparative study to test the efficacy and safety of oral terbinafine pulse as a monotherapy and in combination with topical ciclopirox olamine 8% or topical amorolfine hydrochloride 5% in the treatment of onychomycosis. Indian J Dermatol Venereol Leprol 2007;73:393-396 |
Abstract
Background: Onychomycosis is a fungal infection of nails caused by dermatophytes, yeasts and molds. Aims: To study the efficacy and safety of oral terbinafine pulse as a monotherapy and in combination with topical ciclopirox olamine 8% or topical amorolfine hydrochloride 5% in onychomycosis. Methods: A clinical comparative study was undertaken on 96 Patients of onychomycosis during the period between August 2005 to July 2006. Forty-eight patients were randomly assigned in group A to receive oral terbinafine 250 mg, one tablet twice daily for seven days every month (pulse therapy); 24 patients in group B to receive oral terbinafine pulse therapy plus topical ciclopirox olamine 8% to be applied once daily at night on all affected nails; and 24 patients in group C to receive oral terbinafine pulse therapy plus topical amorolfine hydrochloride 5% to be applied once weekly at night on all the affected nails. The treatment was continued for four months. The patients were evaluated at four weekly intervals till sixteen weeks and then at 24 and 36 weeks. Results: We observed clinical cure in 71.73, 82.60 and 73.91% patients in groups A, B and C, respectively; Mycological cure rates against dematophytes were 88.9, 88.9 and 85.7 in groups A, B and C, respectively. The yeast mycological cure rates were 66.7, 100 and 50 in groups A, B and C, respectively. In the case of nondermatophytes, the overall response was poor: one out of two cases (50%) responded in group A, while one case each in group B and group C did not respond at all. Conclusion: Terbinafine pulse therapy is effective and safe alternative in treatment of onychomycosis due to dermatophytes; and combination therapy with topical ciclopirox or amorolfine do not show any significant difference in efficacy in comparison to monotherapy with oral terbinafine.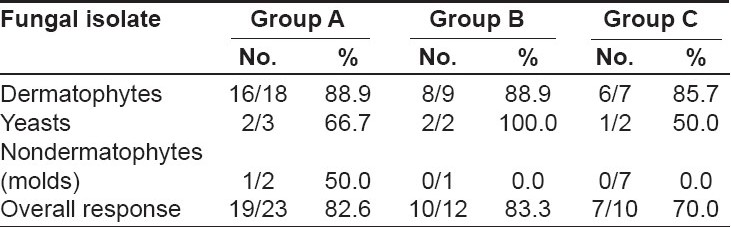
Introduction
Onychomycosis is a chronic infection of the nail predominantly caused by anthropophilic dermatophytes and to a lesser extent by yeasts ( Candida spp.) and nondermatophyte molds. The treatment of onychomycosis is far from satisfactory. However, the advent of terbinafine has revolutionized the therapy of onychomycosis because it has high clinical and mycological cure rates. [1],[2],[3] A major limitation to its widespread use is its high cost. Terbinafine is conventionally given in daily dose for 6-12 weeks. Since it persists in the nail apparatus for long durations even after the therapy is discontinued, pulse therapy is a good option as shown by different studies. [2],[4]
The recent introduction of the newer topical preparation with better drug delivery methods, low cost, low adverse effect profile, has allowed it to combine with the oral antifungal agents and this may cut short the treatment duration, achieve better results and reduce post-treatment relapse. Topical options include a nail lacquer containing either the ciclopirox olamine 8% applied once daily at night or the amorolfine hydrochloride applied once weekly as 5% lacquer; both are active against dermatophytes, yeasts and molds. [5],[6],[7] We compared their efficacy in combination with oral terbinafine vis-a-vis oral terbinafine alone.
Methods
This randomized, single-blind, longitudinal, clinical comparative study was undertaken during the period of August 2005 to July 2006. One hundred and twenty patients presenting to dermatology O.P.D. with clinical features of fingernail or toenail onychomycosis (e.g., discoloration, thickening, crumbling or destruction of nail plate, subungual debris and onycholysis) were subjected to direct microscopic examination of the nail material in potassium hydroxide (KOH) and culture on Sabouraud′s dextrose agar (SDA). Patients with nail abnormalities due to associated skin diseases such as psoriasis, lichen planus, eczema, congenital nail dystrophy or any systemic illness such as malnutrition and iron deficiency were excluded from the study.
The patients were clearly explained the nature of the study and a written consent was taken for their participation in the study. Baseline liver function tests were performed in all of them and those with hepatic dysfunction in the form of jaundice and/or elevated hepatic enzymes more than twice the normal values were excluded from the study. Other criteria for exclusion were pregnancy, lactation, mycologically negative patients (i.e., negative for KOH examination and culture on Sabouraud′s dextrose agar SDA).
A total of 96 patients (clinically suspected and KOH and/or culture positive) satisfied the abovementioned criteria and agreed to participate in the study. They were in the age group of 11-70 years (86 males, 10 females) and were included in the study. All patients were assigned individual identification number and were divided randomly into three groups (A, B and C) using a table of random numbers. Group A (48 patients) received oral terbinafine {Tab. Zimig ® 250 mg} pulse therapy 250 mg twice daily for seven consecutive days every month. Group B (24 patients) received oral terbinafine pulse therapy plus topical ciclopirox olamine 8% {Onylac ®} applied once daily at night on all the affected nails.
Group C (24 Patients) received oral terbinafine pulse therapy plus topical amorolfine hydrochloride 5% {Am-laqer ®} applied once weekly at night on all the affected nails. The total duration of treatment in all groups was four months.
The patients were evaluated at the start of therapy and thereafter at four-week (or monthly) intervals for four months followed by evaluations at 24 and 36 weeks. During these visits, they were assessed for the growth of a normal and healthy nail plate and were inquired for any adverse effects of the drugs. In addition, microscopic examination and culture of nail material were done at 16 and 36 weeks. A liver function test was done at the baseline and at one month from the start of therapy.
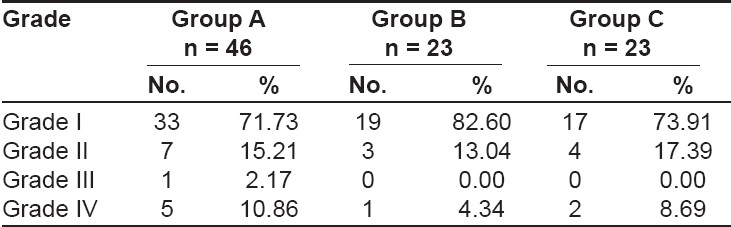
Clinical response was graded according to the changes observed in clinical signs and was divided into four categories: grade I - when the improvement was > 75% in the affected nails (very good response); grade II, - when the improvement was between 51 and 75% (good response); grade III - when the improvement was between 26 and 50% (poor response); and grade IV - when the improvement was less than or equal to 25%.
The clinical cure was defined as grade I response in improvement. Mycological cure was defined as negative microscopy under KOH examination and a negative culture in Sabouraud′s dextrose agar at the end of the follow-up period. At the end of the study, the results were compiled, and analyzed using suitable statistical tools.
Results
In group A, we observed fingernail involvement in 62.5%, toenail involvement in 20.8% and both fingernail and toenail involvement in 16.7%. In group B, the corresponding figures were 50% for fingernail, 29.2% for toenail and 20.8% for both fingernail and toenail involvement. In group C, the corresponding figures were 41.7% for fingernail, 33.3% for toenail and 25% for both fingernail and toenail involvement. In either group, the maximum number of patients belonged to the age group 11-50 years (68.7% in group A, 66.7% in group B, 58.3% in group C). We observed associated dermatophyte infection of other sites in 19 (39.6%) patients [10, Tinea manuum ; 4, Tinea pedis ; 3, Tinea cruris ; 2, Tinea corporis ] in group A and in 7 (29.2%) patients [3, Tinea mannum ; 2, Tinea pedis ; 2, Tinea cruris ] in group B and in 6 (25%) patients [2, Tinea mannum ; 1, Tinea pedis ; 2, Tinea cruris ; 1, Tinea corporis ] in group C.
During the course of the study, two patients in group A, one patient each in group B and C were lost in early follow-up period and were excluded from the analysis of results.
KOH and culture positivity was recorded in 80.0 and 37.5% cases, respectively. Dermatophytes were the commonest isolates seen in 75.56% patients, yeasts in 15.56% patients and nondermatophyte molds in 8.38% patients. Trichophyton rubrum was the commonest isolate in 60% cases, Trichophyton mentagrophytes in 13.3% and Trichophyton tonsurans in 8.38% patients. Candida albicans was the only yeast isolated in 15.6% cases. Among the molds, Aspergillus spp. was isolated in 6.7% patients and Scopulariopsis spp in 2.2% patients.
Clinical cure was observed in 71.73, 82.60, and 73.91% patients in groups A, B and C, respectively [Table - 1].
Mycological cure rates were 82.6, 83.3, and 70% in groups A, B and C, respectively [Table - 2]. Mycological cure rates in case of dermatophytes were 88.9% in groups A and B and 85.7% in group C. In the case of yeast, the mycological cure rates were 66.7, 100 and 50% in groups A, B and C, respectively. In the case of nondermatophytes, the overall response was poor; one out of two cases (50%) responded in group A, while one case each in group B and group C did not respond at all. The difference in clinical cure rates between group A and group B (Chi square =0.48, P=0.49) and between group A and group C (Chi-square =0.04, p=0.85) were not statistically significant ( P> 0.05). Similarly, mycological cure rates among the dermatophytes between group A and group B (Yates corrected Chi square =0.42, P=0.52) and group A and group C (Yates corrected Chi square = 0.22, P=0.64) did not show any significant difference ( P>0.05). In the case of yeast and nondermatophytes, the groups could not be compared (did not satisfy the requirements for Chi-square test). Adverse effects due to terbinafine were observed in 12 (13%) patients (diarrhea, 3; headache, 3; dyspepsia, 2; taste disturbance, 2; pruritus, 1; liver enzyme abnormality 1). All the side effects disappeared with time. Adverse effects due to topical ciclopirox were observed in 2 (8.7%) patients (burning, 1; rash, 1). No adverse effects were observed on the application of amorolfine hydrochloride. None of these effects was sufficiently significant to discontinue therapy except for one patient with liver enzyme abnormality; the level returned to normal in four weeks time.
Cost
The costs of four-pulse regimen of terbinafine, ciclopirox olamine 8%, amorolfine hydrochloride were approximately Rs. 1600, Rs. 850, and Rs. 500, respectively.
Discussion
Onychomycosis is known to be difficult to treat and often exerts a significant negative impact on the quality of life. The agents most commonly used for treatment of onychomycosis are fluconazole, itraconazole, terbinafine as oral agents and ciclopirox, and amorolifine as topical agents. These newer antifungal agents have better pharmacokinetic profiles, such as prompt penetration of the nail and nail bed, persistence in the nail for several months even after the discontinuation therapy and fewer adverse reactions. [1],[5],[7],[8],[9] Ciclopirox olamine is a synthetic antifungal agent, which is a hydroxy pyridone derivative; its mechanism of action is diverse, targeting different metabolic processes in the microbial cell. It has a broad spectrum of antifungal activity against dermatophytes, yeasts and some molds, e.g., Scopulariopsis brevicollis . After the application of ciclopirox nail lacquer 8% to the nail, the solvent evaporates and the concentration in the remaining film increases to 34.87 percent, thereby resulting in a high concentration gradient of the antifungal agent in the nail plate.
Amorolfine hydrochloride is a morpholine derivative. It acts primarily by inhibiting the biosynthesis of ergosterol, [10] a component of fungal cell membrane, and possesses both fungistatic and fungicidal activity. Its spectrum of in vitro activity includes dermatophytes, dimorphic, some dematiaceous and filamentous fungi and yeasts. After a single application of nail lacquer (formulated with methylene chloride), the permeation of amorolfine 5% through the thumb nail ranged from 20 to 100 µg/4 h. [11]
No previous study could be found that compared terbinafine in pulse form and in combination with topical ciclopirox/amorolfine in the treatment of onychomycosis. Pavlotsky et al, [12] studied the pulsed vs continuous terbinafine dosing in the treatment of dermatophyte onychomycosis and concluded that the pulsed regimen is at least as effective as continuous dosing. Moreover, it involves 50% less cost and it is more convenient; hence, it is preferable to the continuous regimen. Avner et al, [13] studied the effectiveness of the combination of oral terbinafine and topical ciclopirox in comparison to oral terbinafine for the treatment of onychomycosis and concluded that combination therapy of oral terbinafine and ciclopirox nail lacquer is a safer and more effective treatment for onychomycosis than terbinafine alone, particularly in younger patients and for a shorter duration of onychomycosis. Baran et al , [14] studied the efficacy of a combination therapy with amorolfine nail lacquer and oral terbinafine in comparison to oral terbinafine alone for the treatment of onychomycosis with matrix involvement and concluded that in the treatment of dermatophytic toenail onychomycosis with matrix involvement, amorolfine nail lacquer in combination with oral terbinafine enhances clinical efficacy and is more cost-effective than terbinafine alone.
Our study shows that pulse therapy with terbinafine (250 mg twice daily for seven days a month) is cost effective and safe in treating onychomycosis due to dermatophytes. How ever, terbinafine was not found to be effective in curing molds infection even when it was combined with topical therapies.
Combination therapy with ciclopirox olamine 8% or amorolfine hydrochloride 5% do not show a statistically significant difference ( P > 0.05) in clinical cure rates than terbinafine monotherapy. The combination of ciclopirox/amorolfine with terbinafine in conventional dosages was found to be less cost effective than terbinafine monotherapy.
Terbinafine pulse therapy is effective and safe in treating onychomycosis (due to dermatophytes) and it is cost effective, ensuring that the patients are likely to complete the therapy. Combination of terbinafine pulse with ciclopirox olamine 8% or amorolfine hydrochloride 5% does not have a significant difference in efficacy than that of terbinafine monotherapy.
| 1. |
Gupta AK, Lynde CW, Konnikov N. Single-blind, randomized, prospective study of sequential itraconazole and terbinafine pulse compared with terbinafine pulse for the treatment of toenail onychomycosis. J Am Acad Dermatol 2001;44:485-91.
[Google Scholar]
|
| 2. |
Tosti A, Piraccini BM, Stinchi C, Venturo N, Bardazzi F, Colombo MD. Treatment of dermatophyte nail infections: An open randomized study comparing intermittent terbinafine therapy with continuous terbinafine treatment and intermittent itraconazole therapy. J Am Acad Dermatol 1996;34:595-600.
[Google Scholar]
|
| 3. |
Nolting S, Brautigam M, Weidinger G. Terbinafine in onychomycosis with involvement by non-dermatophytic fungi. Br J Dermatol 1994;130:16-21.
[Google Scholar]
|
| 4. |
Mishra M, Panda P, Tripathy S, Sengupta S, Mishra K. An open randomized comparative study of oral itraconazole pulse and terbinafine pulse in the treatment of onychomycosis. Indian J Dermatol Venereol Leprol 2005;71:262-6.
[Google Scholar]
|
| 5. |
Gupta AK, Flerkman P, Barean R. Ciclopirox nail lacquer topical solution 8% in the treatment of toenail onychomycosis. J Am Acad Dermatol 2000;43:70-80.
[Google Scholar]
|
| 6. |
Ulbricht H, Worz K. Therapy of onychomycosis due to molds with ciclopirox nail lacquer. Mycoses 1994;37:97-100.
[Google Scholar]
|
| 7. |
Zaug M. Amorolfine nail lacquer: Once-weekly application in onychomycosis. JAMA South East Asia 1993;9:19-22.
[Google Scholar]
|
| 8. |
Gupta AK, Scher RK, De Doncker P. Current management of onychomycosis: An overview. Dermatol Clin 1997;15:121-35.
[Google Scholar]
|
| 9. |
Scher RK. Diseases of the nails. In : Conn H, editor. Current therapy. Philadelphia: WB Saunders Co; 1990. p. 736-42.
[Google Scholar]
|
| 10. |
Polak AM. Preclinical data and mode of action of amorolfine. Clin Exp Dermatol 1992;17:8-12.
[Google Scholar]
|
| 11. |
Franz TJ. Absorption of amorolfine through human nail. Dermatology 1982;184:18-20.
[Google Scholar]
|
| 12. |
Pavlotsky F, Armoni G, Shemer A, Trau H. Pulsed versus continuous terbinafine dosing in the treatment of dermatophyte onychomycosis. J Dermatolog Treat 2004;15:315-20.
[Google Scholar]
|
| 13. |
Avner S, Nir N, Henri T. Pulsed versus continuous terbinafine dosing in the treatment of dermatophyte onychomycosis. J Dermatolog Treat 2005;16:327-30.
[Google Scholar]
|
| 14. |
Baran R, Sigurgeirsson B, Berker D, Kaufmann R, Lecha M, Faergemann J, et al . A multicentre, randomized, controlled study of the efficacy, safety and cost-effectiveness of a combination therapy with amorolfine nail lacquer and oral terbinafine compared with oral terbinafine alone for the treatment of onychomycosis with matrix involvement. Br J Dermatol 2007;157:149-57.
[Google Scholar]
|
Fulltext Views
3,650
PDF downloads
2,357





![[Table - 1]](#tbl_ijdvl_2007_73_6_393_37056_1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2007_73_6_393_37056_2.jpg){kind=link}