Translate this page into:
Analysis of submissions, editorial and peer-review process, and outcome of manuscripts submitted to the Indian Journal of Dermatology Venereology and Leprology over a 6-month period
2 Department of Biostatistics, All India Institute of Medical Sciences, New Delhi, India
Correspondence Address:
M Ramam
Department of Dermatology and Venereology, Teaching Block, Fourth Floor, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029
India
| How to cite this article: Gupta V, Bhatia R, Pathak M, Ramam M. Analysis of submissions, editorial and peer-review process, and outcome of manuscripts submitted to the Indian Journal of Dermatology Venereology and Leprology over a 6-month period. Indian J Dermatol Venereol Leprol 2020;86:519-525 |
Abstract
Background: Despite an interest in the editorial process at biomedical journals, not much information is available on this topic.
Aims: To study the characteristics of the submissions to the Indian Journal of Dermatology Venereology and Leprology (IJDVL) and analyze the editorial and peer-review process and factors influencing the final outcome.
Methods: Retrospective review of the manuscripts submitted to the IJDVL from January 1, 2016, to June 30, 2016.
Results: The IJDVL received 639 manuscripts during the study period, most being Case reports (35%), Research articles (30%), and Letters to editor (20%). The proportion of submissions from Indian (53%) and foreign (47%) authors was comparable. About 55% (n = 353/639) of the submissions were editorially rejected. Some of the common reasons for editorial rejection included “sub-optimal images,” “no novelty,” “incomplete information or results,” and “incorrect diagnosis or interpretation of results.” The acceptance rate during this period was 19%. The median number of days to reach the final decision was 14 days for editorial rejection, 146 days for acceptance, and 85 days for rejection after external peer-review. The acceptance rates were higher for submissions from Indian authors [odds ratio (OR) 1.96], those submitted as Letters (OR 2.06), or in the area of tropical infections (OR 2.17). Submissions as research articles (expB = 1.23), those from Indian authors (expB = 1.15), final decision being acceptance (expB = 1.56), and those requiring preliminary author revisions (expB = 3.34), external re-reviews (expB = 2.22), and repeated author re-revisions (expB = 2.34) were associated with longer times to reach final decision.
Limitations: A relatively short study period of 6 months.
Conclusion: The IJDVL attracts submissions both from India and abroad. Articles submitted in the Letters category or related to tropical infections were most likely to be accepted. There is scope for improving the time taken for editorial processing of manuscripts.
Introduction
There is an interest in the editorial processes undertaken at biomedical journals. Potential authors and some readers may wish to know how editorial decisions are taken and the usual timelines for this process. However, not much information is available in this regard. Previously, an overview of the editorial workflow in the Indian Journal of Dermatology Venereology and Leprology (IJDVL) has been published.[1] We have now looked at all submissions received by the journal over a 6-month period to provide a detailed picture of various characteristics of submissions, editorial decision-making, and timelines.
Methods
We reviewed the following data for the manuscripts submitted to the IJDVL from January 1, 2016, to June 30, 2016: place of submission, type of submitting institute, category, and subject area of submission. The number of days a submission spent in each phase of editorial cycle (triage and primary screening, external peer-review, and secondary screening) and the time to communicate the editorial decision to the author (including the time taken for first response from the journal) were recorded. For manuscripts entering the external peer-review phase, the number of invited reviewers per manuscript, the number of reviewers who responded, their recommendation (accept, accept with revision, reassess, reject), and discordance between reviewer recommendations were noted. The number of manuscripts needing more than one round of external review and revision as well as the number of re-reviews and re-revisions were noted. The final editorial decision for every manuscript and the time to reach the final decision were noted. The reasons for preliminary author revisions before external peer-review, editorial rejection, and final rejection were tabulated. For accepted manuscripts, the article category at the time of acceptance and any change in the category from the time of submission were recorded. The time to publish an accepted manuscript online and in print was also noted. The number of manuscripts which were withdrawn from the editorial cycle and the reasons thereof were listed.
Statistical analysis
Quantitative variables were compared using Wilcoxon rank-sum test, and categorical variables were compared by Chi-square test or Fisher's exact test. The factors influencing final decision were identified using univariate logistic regression [odds ratio (OR) and corresponding 95% confidence interval (CI)]. The factors influencing the time to reach final decision were evaluated using log-linear regression analysis (regression coefficient and corresponding 95% CI). A P value < 0.05 was considered statistically significant.
Results
The IJDVL received 639 manuscripts from January to June 2016. The number of submissions from Indian (n = 339, 53%) and foreign (n = 300, 47%) authors was comparable. Manuscripts were received from all regions of India: 103 (30%) from North India, 97 (29%) from South, 70 (21%) from West, 62 (18%) from East, and 7 (2%) from Central India. Outside India, submissions were predominantly from Turkey (n = 53), China (n = 53), Iran (n = 27), Spain (n = 22), Italy (n = 21), Korea (n = 17), Singapore (n = 14), and Egypt (n = 11), accounting for 73% of our foreign submissions. The majority (n = 570, 89%) of the submissions were from academic institutes. Category and subject-wise distributions of submissions from India and abroad are summarized in [Table - 1].

Editorial process
All submissions to the Journal go through various phases in the editorial cycle. [Figure - 1] shows the timelines and the proportion of manuscripts in different phases of the editorial cycle.
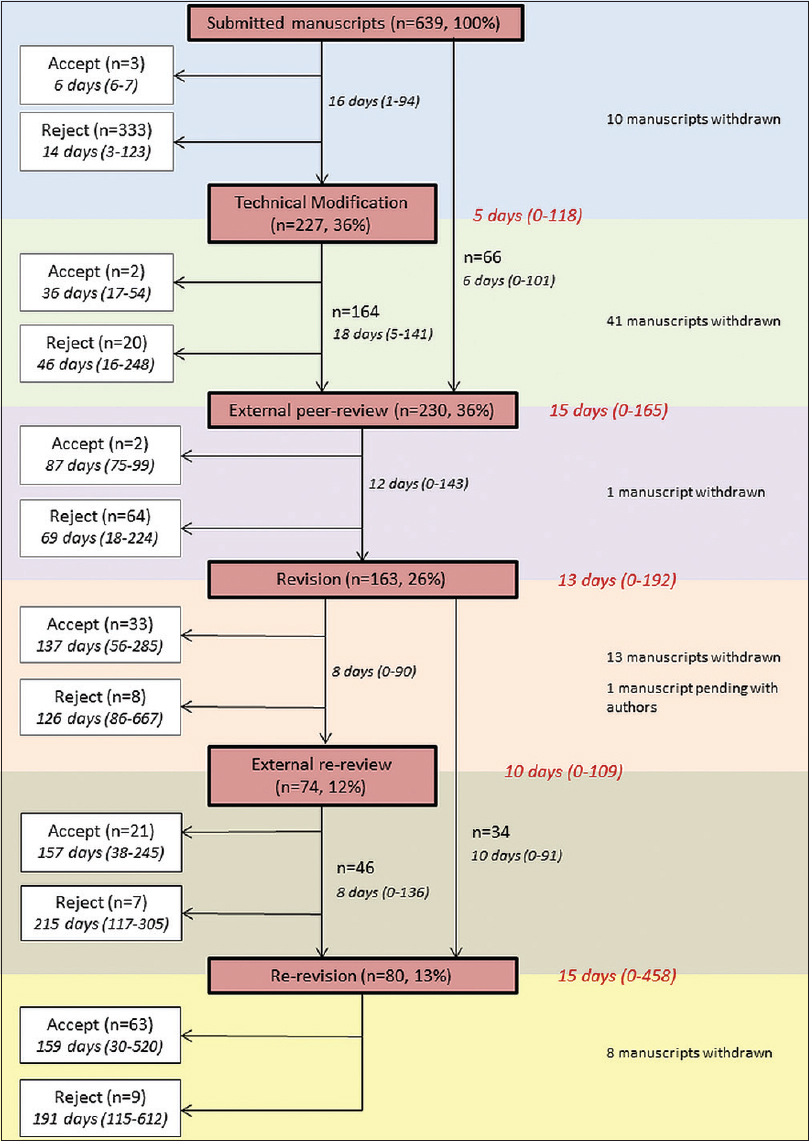 |
| Figure 1: Manuscripts in various phases of editorial cycle. The number of days are expressed as ‘median (range)’. The number of days in “red color” denotes the time spent by the manuscript in each phase |
Triage and primary screening
All submitted manuscripts were screened by a set of 10 team members, all qualified dermatologists. Following this, the manuscripts were assessed by the editor-in-chief and the associate editors.
A little more than half (n = 353/639, 55%) of the submitted manuscripts were rejected following this initial screening (before external peer-review). Of these, 20 (6%) were rejected by the Section Editor following preliminary author revisions. About half (51%, n = 97/192) of the submitted research articles and more than half of Case reports (n = 132/221, 60%), Quiz (n = 16/23, 70%), and Images (n = 33/45, 73%) were rejected editorially [Figure - 2]. The reasons for editorial rejection specific to the manuscript were communicated to authors in 98% (n = 346/353) of manuscripts [Table - 2]. Only five submissions (Book reviews, n = 3; Letter in response to published article, n = 2) were accepted at this stage.
 |
| Figure 2: Proportion of manuscripts being editorially rejected as per submission category |

About 45% (n = 293/639) of submissions were assigned to the Section Editors for further processing. Of these, 227 (77%) manuscripts were deemed to require preliminary author revisions before further processing. These revisions fell into three large groups: those related to author instructions, those requiring a change in the category in which the manuscript had been submitted, and those related to the content of the article [Table - 3]. Quite frequently (81.5%, n = 185/227), more than one type of problem was identified in a manuscript. Most manuscripts (70%, n = 159/227) could be processed after one author revision, but others required further revisions because all the editorial queries were not addressed in the first instance (mean number of preliminary author revisions before further processing 1.52 ± 0.98, median 1, range 1–6).

External peer-review
About a third (36%, n = 230/639) of submissions were sent for external peer-review. Most (59%, n = 136/230) of the manuscripts were sent to 2–3 reviewers, while 8 (4%) were sent to a single reviewer and 86 (37%) to more than 3 reviewers (range 4–14 reviewers). This number includes reviewers for first cycle of peer-review as well as any additional reviewers invited for subsequent peer-reviews. No reviewer could be found for one manuscript submitted on a basic science topic, which was ultimately withdrawn from the editorial cycle. The median reviewer response rate was 67%, that is, two out of three reviewers responded per manuscript. In about a quarter (24%, n = 56/230) of manuscripts, comments were received from only one reviewer. Of the manuscripts where >2 reviewer comments were available, 59% (n = 102/173) had discordance between the reviewers' recommendation.
Secondary screening
Following peer-review, a final decision could be taken for 66 (29%) manuscripts, almost all (97%, n = 64/66) being rejections. The other 163 (71%) manuscripts were sent to the authors for revision in the light of referee comments.
Following author revision, manuscripts were either sent for another round of external peer-review (45%, n = 74/163), sent back to the author for further revisions (21%, n = 34/163), or given a final decision (25%, n = 41/163): 33 were accepted and 8 were rejected.
Of the 74 manuscripts sent for re-review, 11 (15%) required repeated rounds of re-review (median 2, range 2–4 rounds). Overall, 80 (49%, n = 80/163) manuscripts required author re-revisions: 34 because the first revision was unsatisfactory and/or incomplete and 46 because the subsequent round of peer-review raised further questions. Forty-two (53%) of these manuscripts required two to six re-revisions.
Following the final author re-revisions (n = 80), a final decision could be reached in 72 manuscripts: 63 were accepted and 9 were rejected.
Final decision
Of the total 639 submissions, 124 (19%) were accepted, 441 (69%) were rejected (353 editorially rejected, 88 after external peer-review), and 74 (12%) were withdrawn. The reasons for final rejection following external peer review are summarized in [Table - 4]. Fifty-one (41%) of the 124 accepted manuscripts were accepted after a change in the article format: this was maximum for Case reports (88%, n = 29/33), followed by Original articles (37%, n = 10/27), Images (33%, n = 2/7), Brief reports (33%, n = 2/6), and Letters (24%, n = 8/34) [Figure - 3]. All other manuscripts, mainly review articles and quiz, were accepted in the format in which they had been submitted.

 |
| Figure 3: Distribution of different article categories at acceptance vis-a-vis at submission |
Of the 74 withdrawn manuscripts, 40 (54%) were withdrawn by the journal, the most common reason being “lack of response from the authors” to editorial/reviewer comments (n = 32, 80%). The other 34 (46%) manuscripts were withdrawn by the authors, the most common reason being “do not wish to change to a shorter format” (n = 13, 39%), followed by “cannot provide additional images or information” (n = 4, 12%), “wish to re-submit after corrections” (n = 3, 9%), and “lack of time” (n = 3, 9%). Other reasons included “too much time being taken by the journal” (n = 1, 3%), “manuscript accepted in another journal” (n = 1, 3%), and “manuscript uploaded by mistake” (n = 1, 3%), while no reason was given for 8 (23%) manuscripts.
The overall median number of days to reach the final decision varied considerably depending on the final decision: 14 [interquartile range (IQR) 10–26, range 3–248] days for editorial rejection, 146 (IQR 99–194, range 17–520) days for acceptance, 85 (IQR 59–132, range 17–612) days for rejection after external peer-review, and 121.5 (IQR 53–195, range 1–1083) days to withdraw a manuscript.
Publication: Online and in print
Of the 124 accepted manuscripts, 120 have been published online and in print (114 manuscripts were online ahead of print), so far. The median time to publish the manuscript online after acceptance was 194 (IQR 158–255, range 22–518) days, while it was 267 (IQR 209–361, range 22–662) days for publishing in print.
Time for first response from the Indian Journal of Dermatology Venereology and Leprology
Overall, the median time for first response to authors varied depending on the response: 14 (IQR 10–26, range 3–248) days for editorial rejection, 16 (IQR 11–21, range 1–93) days for preliminary author revision, 64 (IQR 35–118, range 19–224) days for rejection after external peer-review, and 70 (IQR 33–95, range 11–160) days for author revision after external peer-review.
Factors influencing final decision
Place of submission
The acceptance rate for Indian authors (24%, n = 82/339) was statistically significantly higher than for foreign authors (14%, n = 42/300), translating into an OR of acceptance of 1.96 (95% CI 1.30–2.95, P = 0.001) for Indian authors. The acceptance rate was 32% (n = 20/62) for manuscripts from Eastern states of India, 29% (n = 30/103) from North India, 20% (n = 14/70) from West India, and 19% (n = 18/97) from South India, while none of the seven submissions from Central India was accepted (P = 0.09). The acceptance rate for manuscripts submitted from teaching and non-teaching institutes was similar (19.5%, n = 111/570 vs 18.8%, n = 13/69; P = 0.9).
Category of submission
Of the major categories, the acceptance rate was highest for Letters (30%, n = 37/125), followed by Reviews, (24%, n = 4/17), Research articles (17%, n = 33/192), Images, (16%, n = 7/45), Case Reports (15%, n = 33/221), and Quiz (13%, n = 3/23) (P = 0.022). This translates to an OR of acceptance of 2.06 (95% CI 1.31–3.23, P = 0.001) for Letters when compared with other categories combined. This statistic was not significant for any other category of submission.
Subject area of submission
Manuscripts in the area of tropical infections had the highest acceptance rate of 33% (n = 17/52). The acceptance rates for manuscripts on general dermatology (20%, n = 81/407), pediatric dermatology (17%, n = 8/48), sexually transmitted infections and HIV (22%, n = 6/27), leprosy (15%, n = 3/20), dermatoscopy (21%, n = 3/14), and basic science (18%, n = 4/22) were comparable, while it was quite low for dermatopathology (7%, n = 1/14) and other sub-specialities (3%, n = 1/34) (P = 0.08). Manuscripts related to tropical infections had an OR of acceptance of 2.17 (95% CI 1.18–4.03, P = 0.013), while it was not statistically significant for manuscripts submitted in any other field.
Factors influencing the time to final decision
On univariate analysis, longer time to reach a final decision was associated with submissions in the category of research article or letter, manuscripts that were finally accepted, submissions from Indian authors, and manuscripts requiring preliminary author revision, external re-review or author re-revision. Multivariate regression analysis revealed longer time to reach a final decision was associated with submissions in the category of research articles, manuscripts that were finally accepted, submissions from Indian authors, and manuscripts requiring preliminary author revision, external re-review or repeated author re-revisions [Table - 5].

Discussion
The IJDVL received articles from both Indian and international authors in comparable numbers. The majority of the submissions were from academic institutions. Case reports, Research articles, and Letters formed the bulk (85%) of submissions. The journal's acceptance rate during this period was 19%, which compares favorably with most other dermatology journals. Most rejections occurred during the initial in-house triage process (80%) or after the first round of peer-review (an additional 18%). However, once the manuscript passes this stage, the chances of acceptance increase and continue to increase as it makes its way further into the editorial cycle: twenty percent (n = 33/163) were accepted after first author revision, twenty eight percent (n = 21/74) after external re-reviews, and seventy nine percent (n = 63/80) after author re-revisions.
The acceptance rate for submissions from Indian authors was higher than from foreign authors, probably reflecting the quality of articles the journal attracts from Indian authors. Apart from reasons such as a lack of novelty, incomplete or incorrect results, and flawed methodology,[2],[3] sub-optimal quality of submitted images emerged as an important reason for editorial rejection. As dermatology is largely a visual science, the quality of image is often one of the deciding factors. The journal is making every effort to improve the quality of published photographs: there are three dedicated image editors who carefully scrutinize the submitted images and even suggest ways to the authors on how to improve them. An editorial discussing some common pitfalls of clinical photography has been published previously.[4]
Of the manuscripts which were not rejected straight away, a large majority (77%) were sent back to the authors for preliminary revisions before further processing. The most common reasons for this were not following author instructions correctly, followed by sub-optimal quality of images. A change in article category, usually conversion to a shorter format, was requested in about 41% of manuscripts before acceptance, mostly for Case Reports and Original articles. Like most other journals, IJDVL is also consciously shifting away from Case reports, with only well worked-up novel cases or case series which can potentially impact the clinical practice being considered for this format.
The median editorial rejection time of the IJDVL was 14 days, a bit longer than what one might expect. However unlike most other journals, IJDVL provides fairly detailed and specific feedback for manuscripts that are editorially rejected. This slows the triage process, but it is likely that authors appreciate the effort made to explain the editorial decision and suggestions for improving the manuscript. Although there are no accepted standard editorial turnover times, it has been suggested that the results of a peer-review should be available in 1–2 months for research articles and review papers, and the authors are expected to submit the revision within a month. For Letters to editor and Commentaries, the suggested time to reach a final decision is 2 weeks. 5 The journal has some way to go to meet these benchmarks, and a part of the reason may be that the entire editorial team works on a purely voluntary basis and nearly all members are clinical dermatologists, with additional academic and other responsibilities. Some measures are being considered and implemented to improve the editorial workflow. A recently implemented change was assigning an editorial team member the task of keeping manuscripts moving rather than depending on system-generated reminders. In addition, there is an attempt to reduce the number of manuscripts sent back to referees for re-review. Currently, this figure stands at 45% (n = 74/163). Reserving re-reviews only for those articles where outside expertise is imperative is likely to speed-up the workflow. There is a clear need for the IJDVL to improve its manuscript processing time. One of the major challenges is finding reviewers who can provide constructive criticism in a timely manner. On an average, about a third of the reviewers did not respond, which often necessitated sending the manuscript to additional reviewer (s). Other problems included too much time taken by the reviewers and unsatisfactory quality of reviewers' comments (sometimes just one word!). Holding workshops for reviewers may improve the external peer-review process.[6] Sending the manuscripts back to the authors for revisions repeatedly also led to a delay in the final decision. One of the main reasons behind this was the failure of the authors to address all queries at one go. A continuous process of self-appraisal followed by improvements in workflow will serve the journal well in its goal of meeting the expectations of IADVL and the larger bio-medical community.
Limitations
This study was limited to IJDVL over a 6-month period. A study covering a longer period and comparison of data with other journals of dermatology could have given us better insight.
Acknowledgement
The authors would like to acknowledge Ms. Alexy Babu for her assistance in gathering the data for statistical analysis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Ramam M. The manuscript review process: What do editors do? Indian J Dermatol Venereol Leprol 2016;82:599-602.
[Google Scholar]
|
| 2. |
Pierson DJ. The top 10 reasons why manuscripts are not accepted for publication. Respir Care 2004;49:1246-52.
[Google Scholar]
|
| 3. |
Gupta P, Kaur G, Sharma B, Shah D, Choudhury P. What is submitted and what gets accepted in Indian pediatrics: Analysis of submissions, review process, decision making, and criteria for rejection. Indian Pediatr 2006;43:479-89.
[Google Scholar]
|
| 4. |
Kaliyadan F. Image quality for publication. Indian J Dermatol Venereol Leprol 2016;82:367-70.
[Google Scholar]
|
| 5. |
da Silva JA, Dobranszki J. Excessively long editorial decisions and excessively long publication times by journals: Causes, risks, consequences, and proposed solutions. Publ Res Q 2017;33:101-8.
[Google Scholar]
|
| 6. |
Schroter S, Black N, Evans S, Godlee F, Osorio L, Smith R. What errors do peer reviewers detect, and does training improve their ability to detect them? J R Soc Med 2008;101:507-14.
[Google Scholar]
|
Fulltext Views
5,119
PDF downloads
2,425





![[Table - 1]](#tbl_ijdvl_2020_86_5_519_280118_t4.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2020_86_5_519_280118_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_5_519_280118_f2.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2020_86_5_519_280118_t5.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2020_86_5_519_280118_t6.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2020_86_5_519_280118_t7.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_5_519_280118_f3.jpg){kind=link}
![[Table - 5]](#tbl_ijdvl_2020_86_5_519_280118_t8.jpg){kind=link}