
Translate this page into:
Clinical characteristics of 81 patients with maculopapular cutaneous mastocytosis: A 10-year experience
Corresponding author: Prof. Yue-Hua Liu, Department of Dermatology, Peking Union Medical College Hospital, Dongcheng District, Beijing, China. yuehualiu63@163.com
-
Received: ,
Accepted: ,
How to cite this article: Jia QN, Fang K, Wang T, Zhang SY, Yang L, Liu YH. Clinical characteristics of 81 patients with maculopapular cutaneous mastocytosis: A 10-year experience. Indian J Dermatol Venereol Leprol. 2024;90:372-5. doi: 10.25259/IJDVL_712_2023
Dear Editor,
Cutaneous mastocytosis (CM) is characterised by abnormal dermal accumulation of mast cells. Maculopapular CM (MPCM) is the commonest clinical type and is subdivided into pigmented variant (urticaria pigmentosa, UP) and telangiectatic variant (telangiectasia macularis eruptiva perstans, TMEP). This study reviewed all patients with histologically confirmed diagnosis of MPCM between 2009 and 2022 and characterised its detailed clinical manifestations. UP diagnosis was based on typical clinical lesions and monomorphic mast cell infiltrate. TMEP was characterised by characteristic telangiectatic macules and increased mast cells at the periphery of dilated blood vessels in the upper dermis.
In total, 81 patients were analysed, with 54 males and 27 females (2:1). The demographics and clinical characteristics of MPCM have been summarised in Table 1. There were 70 patients diagnosed with UP and 11 patients of TMEP. The mean age (± SD) of disease onset in years was 18.04 ± 15.93 in UP and 38.41 ± 14.96 in TMEP. Twelve patients with UP had congenital lesions. Most TMEP lesions developed between 31 and 50 years (8/11, 72.7%). None of our patients reported a positive family history or had any extracutaneous disease.
| All | UP | TMEP | |
|---|---|---|---|
| All | 81 | 70 | 11 |
| Male | 54 | 46 | 8 |
| Female | 27 | 24 | 3 |
| Onset/year | 28.23 | 18.04 | 38.41 |
| Location | |||
| Trunk | 72 | 65 | 7 |
| Extremities | 70 | 60 | 10 |
| Scalp & face | 23 | 23 | 0 |
| Neck | 22 | 21 | 1 |
| Patient outcome | |||
| CR | 4 | 3 | 1 |
| PR | 18 | 14 | 4 |
| NR | 21 | 18 | 3 |
| Worsen | 9 | 9 | 0 |
UP: urticaria pigmentosa, TMEP: telangiectasia macularis eruptiva perstans, CR: complete remission, PR: partial remission, NR: non-remission
TMEP presented with multiple discrete red to brown telangiectatic macules [Figure 1a]. On the contrary, UP displayed a heterogeneous appearance in the morphology and arrangement of lesions as multiple yellow-orange to red-brown papules, plaques and nodules [Figures 1b to 1g]. The trunk and extremities were commonly affected in UP, followed by the scalp and face. However, the scalp and face were spared in TMEP, which mostly affected the upper limbs.

- Telangiectasia macularis eruptiva perstans (TMEP) lesions were multiple discrete red to brown telangiectatic macules.

- Multiple red brown small macules of urticaria pigmentosa on abdomen.

- Multiple symmetrically distributed larger polygonal pigmented macules of urticaria pigmentosa on the legs.

- Multiple yellow to red brown small macules of urticaria pigmentosa on the back.
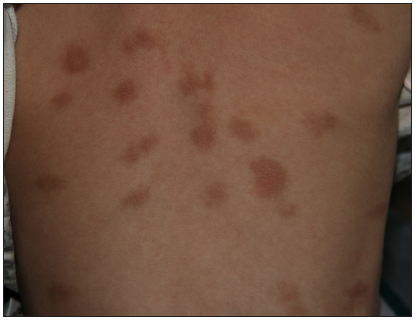
- Multiple large round to polygonal variably shaped pigmented macules of urticaria pigmentosa on the back.

- Multiple variably sized pigmented macules of urticaria pigmentosa on the back.

- Yellowish orange to red brown elevated papules of urticaria pigmentosa on the abdomen.
Patients underwent telephonic disease evaluation at the study endpoint. Among 46 patients with UP, 3 (6.5%) patients fully resolved over 2 years, 14 (30.4%) patients had partial remission, and 18 (39.1%) patients reported non-remission, while 9 (19.6%) patients presented with increased skin lesions. Of the 8 patients with TMEP, 1 fully regressed in 11 years, 4 partially regressed, and 3 showed unchanged disease conditions.
This study provides a detailed description of the clinical presentation of MPCM. Patients with mastocytosis have been commonly reported with systemic involvement in Caucasians.1–2 This is one of the first studies performed in the Chinese population of all ages, suggesting that Chinese patients with mastocytosis tend to have isolated cutaneous lesions without systemic involvement. Although equal gender distribution and male or female predominance have been described in the literature, this study exhibited a significant predilection for males.3–5
Among 54 patients evaluated at study endpoint, several showed increased skin lesions, and most patients had partial or non-remission, while only a small minority presented complete remission. The 10-year experience from our hospital suggested that Chinese patients tend to have persistent lesions without the tendency to regress.
TMEP is no longer considered a separate subtype in the recent World Health Organization (WHO) classification of CM and some authors suggest TMEP to be a specific form of MPCM.6 Another study described high frequency (47%) of systemic involvement in TMEP and suggested it as an individualised type of mastocytosis.7 In our study, TMEP accounted for a large proportion (13.6%) of MPCM. Compared to UP, TMEP exhibited an older age of onset, variable distribution and clinical presentation of skin lesions. Our results further validate TMEP as a distinct entity of CM.
To explore whether clinical appearance is associated with disease parameters, UP was defined as round [Figure 1b] or polygonal [Figure 1c] in shape; small (<1 cm) [Figure 1d], large (≥1 cm) [Figure 1e] or variable [Figure 1f] in size; flat [Figures 1e and 1f] or elevated [Figure 1g] lesions [Table 2]. Round lesions and polygonal lesions were distributed evenly. Compared to patients with round lesions, those with polygonal lesions exhibited earlier disease onset (P < 0.001). Concerning size, small lesions were most frequent. Compared with large and variable lesions, patients with small lesions reported later disease onset (P < 0.001). Flat lesions were more frequent than the elevated form (49 and 21 patients, respectively). The demography did not differ between flat and high lesions (P > 0.05). Our results demonstrated that polygonal lesions and large or variable sizes characterised patients with earlier disease onset.
| Shape | Size | Elevation | |||||
|---|---|---|---|---|---|---|---|
| Round | Polygonal | Small | Large | Variable | Flat | Elevated | |
| All | 39 | 31 | 40 | 22 | 8 | 49 | 21 |
| Male | 24 | 22 | 24 | 16 | 6 | 30 | 16 |
| Female | 15 | 9 | 16 | 6 | 2 | 19 | 5 |
| Onset/year | 25.67 | 8.45 | 26.13 | 6.24 | 10.01 | 17.85 | 18.48 |
| Patient outcome | |||||||
| CR | 2 | 1 | 1 | 1 | 1 | 3 | 0 |
| PR | 5 | 9 | 4 | 7 | 3 | 7 | 7 |
| NR | 11 | 7 | 11 | 4 | 3 | 10 | 8 |
| Worsen | 7 | 2 | 8 | 1 | 0 | 4 | 5 |
CR: complete remission, PR: partial remission, NR: non-remission
In conclusion, the present study found that Chinese patients with mastocytosis tend to have isolated CM without systemic involvement, significant predilection for males, and persistent lesions without significant remission. Our results suggest that TMEP is a distinct entity of CM, and it is better to maintain the concept of TMEP.
Ethical approval statement
The research/study is approved by the Ethics Committee of Peking Union Medical College Hospital.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent and ethical approval from ethics committee of Peking Union Medical College Hospital.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Frequency of isolated cutaneous involvement in adult mastocytosis: a cohort study. J Eur Acad Dermatol Venereol. 2019;33:1713-8.
- [Google Scholar]
- The data registry of the european competence network on mastocytosis (ECNM): Set up, projects, and perspectives. J Allergy Clin Immunol Pract. 2019;7:81-7.
- [Google Scholar]
- Large maculopapular cutaneous lesions are associated with favorable outcome in childhood-onset mastocytosis. J Allergy Clin Immunol. 2015;136:1581-90.
- [Google Scholar]
- Cutaneous mastocytosis in children: A clinical analysis of 71 cases. J Eur Acad Dermatol Venereol. 2004;18:285-90.
- [Google Scholar]
- Phenotypic and genotypic characteristics of mastocytosis according to the age of onset. PLoS One. 2008;3:e1906.
- [Google Scholar]
- Telangiectasia macularis eruptiva perstans or highly vascularized urticaria pigmentosa? J Allergy Clin Immunol Pract. 2014;2:813-5.
- [Google Scholar]
- Telangiectasia macularis eruptive perstans (TMEP): A form of cutaneous mastocytosis with potential systemic involvement. J Am Acad Dermatol. 2016;74:885-91.
- [Google Scholar]




