Translate this page into:
Clinimetric analysis of recently applied quantitative tools in evaluation of vitiligo treatment
2 Department of Public Health, Community Medicine and General Health, Benha University, Banha, Egypt
3 Dermatologist at Ministry of Health Hospital, Cairo, Egypt
Correspondence Address:
Rehab Mohammed Salem
Benha University, Banha
Egypt
| How to cite this article: Mikhael NW, Sabry HH, El-Refaey AM, Salem RM, El-Gendy MF, Farid SA. Clinimetric analysis of recently applied quantitative tools in evaluation of vitiligo treatment. Indian J Dermatol Venereol Leprol 2019;85:466-474 |
Abstract
Background: Vitiligo affects about 1% of the world's population, however, there is currently no universally used standardized measure to assess its response to treatment.
Objective: To find the most effective technique for the quantitative assessment of therapeutic results in vitiligo patients.
Materials and Methods: The study was performed in three stages: (1) Conducting an adapted Delphi survey to check current dermatologists' attitudes regarding the topic of study. (2) Conducting a pilot study that involves testing the selected digital image analysis software in the laboratory to validate future tasks. (3) The chief clinimetric study that implicates selecting actual vitiligo lesion models and evaluating them.
Results: Regarding the surface area measuring techniques, the most accurate results were gained through the digital image analysis for surface area, followed by point-counting technique. The digital image analysis for color measurement was accurate and reliable in getting a percentage representation of color improvement within the vitiligo lesions, in response to therapy.
Limitations: Many dermatologists lack understanding of basic concepts about imaging techniques. The study does not include a traditional assessment method such as vitiligo area scoring index.
Conclusion: Our designated digital image analysis technique was able to efficiently assess the changes that occur both on surface area and the color of vitiligo lesions in response to therapy.
Introduction
Vitiligo is a chronic depigmenting disease with a prevalence of 0.5–1.0%. Various treatments have been evaluated, including topical and oral preparations, light therapy, surgical procedures, as well as psychological and complementary therapies.[1]
Many studies have reported the clinical effectiveness of various treatments for vitiligo; yet, there is only limited data available regarding the practical management of patient. One of the major challenges is the lack of uniformity in evaluation methods used to assess treatment outcomes. Most authors agree that the determination of a “change in area” is the most important parameter for assessment with regards to treatment outcome, yet despite this almost all scholarly articles use different scales to assess treatment success.[2] The assessment of vitiligo treatment relies primarily on subjective methods, such as visual assessment by the physician and/or analysis of photographs taken before and after treatment under visible or ultraviolet light.[3]
Modern trends in dermatology tend to rely more on realistic measurements for skin lesions rather than on crude scores derived from data designed to determine the efficacy of different therapeutic modalities.[4] Despite this, although skin is the largest organ of the body, there are still no standardized reproducible methods available for assessing the severity of many skin diseases. During recent years, several scoring systems have been introduced to help clinical practice and clinical research in skin diseases; these scales mainly compare interindividual differences in disease activity.[5]
Variation in the size of treated areas in some skin conditions such as wounds and leg ulcers are evaluated by area measurements, but this is not applicable to vitiligo.[6] Different techniques and scoring systems have been proposed to assess the severity of vitiligo's response to treatment and to evaluate the activity and the potential for re-pigmentation.[3] These techniques can be classified as subjective, semi-objective or objective; microscopic or macroscopic; and can be based on morphometry or colorimetry. Macroscopic morphological measurements include visual assessment, photography in natural or ultraviolet light, photography with computerized image analysis and tristimulus colorimetry or spectrophotometry. The noninvasive micromorphological methods include confocal laser microscopy. The subjective methods include clinical evaluation by a dermatologist and a vitiligo disease activity score. The semi-objective methods include the vitiligo area scoring index and point-counting methods. The objective methods include software-based image analysis, tristimulus colorimetry, spectrophotometry and confocal laser microscopy. Morphometry is the measurement of the vitiliginous surface area, whereas colorimetry provides a quantitative analysis of skin color changes caused by erythema or pigment. Most methods involve morphometry, except for the chromameter method, which assesses colorimetry. Some image analysis software programs can assess both morphometry and colorimetry. Reflectance confocal microscopy provides real-time images and has the potential to be a great option for the noninvasive assessment of pigmentary lesions.[7] Although various techniques are available, there is currently no consensus on the methods of assessment that should be used in clinical trials and daily practice. At present, it is difficult to compare the efficacy of different treatment modalities because measurement of re-pigmentation is not standardized.[3]
Aim of the work
The aim of this study was to find out the best technique for quantitative assessment of therapeutic results in vitiligo patients. The evaluation will focus on two main parameters used when evaluating vitiligo in follow-up sessions: the surface area of lesions and the color difference between normal and depigmented skin.
Methods
There are three main stages in this study. Two stages were related to preparation of the central work strategy and they were:
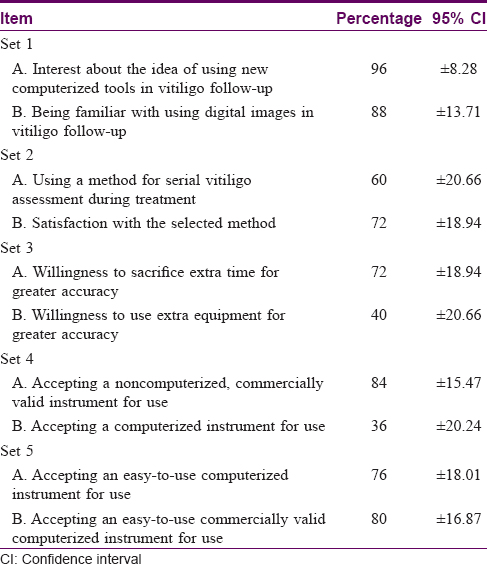
- Conducting an adapted Delphi survey: A series of five questionnaire sets were structured and then answered by a panel of 25 dermatologists with varying levels of experience. The selected dermatologists were all practicing in 25 different cities/towns across Egypt. Each answer was ranked on a grade system of four levels: 0, for no; 1, 2 and 3 for yes levels from the lowest to the highest, respectively, as depicted from each surveyor choice. The answers were collected using both a traditional paper and pencil survey and e-mail survey, and were conducted in accordance with surveyor's residence.
- Conducting a validating pilot study (aided by two computer specialists observers): It involved testing the selected digital image analysis software from the study in the laboratory concerning the following points:
- Validation of computerized planimetry regarding both scanned and photographic traces (digital image analysis for surface area): That was achieved using 10 simulated circular models with known surface areas drawn on graded sheets. These traces were scanned at a 300 DPI (pixels per inch) resolution and also photographed using the same camera for the study. Both scanned and photographic traces of the drawn circular models were separately measured using Photoshop. The drawings were done by the observers in two trials, each performed 2 weeks apart (for each trace type), to ensure minimal memory recall bias
- Validation of the color measurement procedure (digital image analysis for color measurement): Ten vitiligo lesions were photographed with two consecutive shots. Care was taken to alter the illumination conditions in the scene before capturing the second image. Each image was subjected to color sampling by the two observers using LAB color values. The color difference between normal skin and lesion/s was calculated for each shot and compared with the original image.
- The chief clinimetric study that involved selecting actual vitiligo lesions from vitiligo patients seeking medical care in the Outpatient Clinic of Benha University Hospital.
The equipment used was:
- A digital image analysis system:
- Digital photography equipment: A Kodak EasyShare Z1485 IS digital camera (2009) model (×5 optical zoom function) was selected for the work. Red, green and blue digital images were captured and retrieved in JPEG format with the s-RGB embedded color profile
- Digital image analysis software: The 2010 version of Adobe Photoshop CS® extended series; Adobe Photoshop CS5 Extended® (Photoshop) launched onto a laptop.
- Point-counting equipment:
- Transparent sheets: Semi-squeezing, crystal clear plastic sheets
- Black ball-pointed marker
- Point-counting grids: Two point-counting grids were designed and printed with the aid of a computer graphics' expert, using Corel Graphics Suite® software. One of the designs had a 1.0 cm2 representative area and the other had a 0.25 cm2 representative area.
- An image-digitizing kit: Consisting of a scanner with a scanning resolution capacity of more than 300 DPI.
The clinimetric study:
- Ethical considerations: The study was conducted in accordance with ethical rules and patients' confidentiality was respected during data collection. All procedures and the potential outcomes and benefits of the study were explained to participants taking part in the study (patients and observers) before study trial was conducted. Consent to use the enrolled patients' images in the study was obtained verbally.
- The participating observers and the number of assessments: In order to investigate the “interobserver reproducibility,” after a brief illustration of the aim of the study, two observers (a dermatologist and a computer specialists) were independently retained to follow the described methods. To evaluate the “intraobserver reproducibility” of the obtained measurements, each observer used their chosen method in two separate trials for each lesion. The two trials for each lesion were separated by 2 weeks (as in the pilot study).
- The tested techniques:
Two chief procedures were analyzed (surface area measurement and color analysis):
- Analysis of the surface area measurement techniques
- Sample selection: A total of 50 vitiligo lesions were selected. Lesions were eligible for the study if they met two inclusion criteria: localized and well-demarcated; and exhibiting total homogenous depigmentation at the time of first assessment. Vitiligo of the fair skin (phototypes I and II), vitiligo of the lips and extremities, segmental vitiligo and lesions occupying a skin fold were excluded from the study.
- Sample handling: The selected lesions were subjected to the following two processes (in two separate sessions separated by a treatment course):
-
- Tracing of lesions' boundaries on transparent sheets: These traces were cataloged with a serial number for each lesion and a patient's code in addition, in terms of the session's order. Transparency-based traces of lesions contours were also scanned at 300 DPI
- Digital photography
- The manual program of the camera was used during shooting.
- The field was adjusted via the optical zoom. The chosen resolution was the maximum one offered by the camera (480 pixels/inch).
- Special care was taken during taking the photographs in order to keep the camera lens perpendicular to the photographic field to avoid exposure bias.
- A ruler was placed within the photographic field, at a place not obscuring the photographed lesion.
- Using Photoshop tools, the obtained images were subjected to a process of restoration (i.e. correction of minor technical faults, removal of noises, construction of a scale marker of 1 cm and documentation).
- The measuring procedure:
-
- Establishing a gold standard to assess accuracy: Photoshop was used to measure all of the scanned transparency-based traces of the lesions all at once (as the procedure was not vulnerable to memory recall bias). These measurements were recorded and considered the gold standard in terms of accuracy. Measurements obtained by the tested techniques were compared with these control samples.
- Application of the three designated methods:
-
- Simple visual observation: Using the scale marker constructed within the photographic traces as a reference, simple visual estimations of the length and width (in cm) of each lesion were made by each observer. This was done via visual examination of the lesion image (using the laptop monitor). Multiplying length by width would finally give an estimate of surface area of that lesion (in cm2).
- Point-counting technique: Observers were instructed to place the transparent sheets (on which the lesion contours were copied) arbitrarily over the selected point-counting grid, and then count the points in the area within the drawn boundaries. Finally, the surface area of the lesion was calculated by multiplication of the number of counted points, by the representative area of the used grid.
- Digital image analysis for surface area of photographic traces: This method was performed using the “Analysis” menu of Adobe Photoshop CS5 Extended. The observers were instructed to invert the color information of the images to enhance the contrast between lesional and nonlesional skin. Perifollicular re-pigmentation areas that appeared in some lesions in the second session were excluded during the measurement procedure. Exclusion eliminated potential error that might result. Alternatively, the areas that joined the borders of the lesions were automatically added to the normal skin areas with the resultant shrinkage of the overall lesional area.
- Analysis of the planned digital image analysis technique for color measurement
- Sample selection: Another sample of 20 vitiligo lesions was selected from 10 patients (two lesions per patient). As there was no gold standard for accuracy, every two lesions were selected bilaterally from the symmetrical body portions in each patient. This was done to detect the reliability of results by standardizing the expected response to treatment of the two lesions (to virtually assess the accuracy).
- Sample handling: Each lesion was photographed on two occasions (before and 12 weeks after treatment) without standardizing the illumination source in the two shots
- Obtaining measurements: Using LAB color values (as directly computed by Adobe Photoshop CS5 Extended), the calculated color differences were used to obtain a percentage of treatment results from every two shots, taken for each lesion.
Statistical methodology
Raw data were deposited onto the Microsoft® Excel (2010) spreadsheets and subsequently exported to MedCalc software for Windows (version 11.6.1© 1993-2011, MedCalc Software® bvba) for analysis.
Results
Analysis of our Delphi set results showed that 96% of our observers were interested in the idea of using new computerized tools in vitiligo's follow-up. Although 72% of the observers were satisfied with methods they were already using, 80% were also accepting of an easy-to-use, commercially valid, computerized instrument. They would also be willing to sacrifice extra time for greater accuracy [Table - 1].
With regards to the surface area measurement, the pilot study did not show differences between the measurements obtained by both observers using both methods of digital planimetry and the actual surface areas (gold standard) (P > 0.05). There were significant levels of agreement regarding the interobserver reproducibility (r = 1.00, P < 0.001) and the intraobserver reproducibility (r = 1.00, P < 0.001). Similar results found for the color difference measurement (P < 0.001) for both photographs in both inter- and intraobserver reproducibility, in the pilot study.
After a treatment period ranging from 4 to 12 weeks, the actual reductions in the surface area of lesions ranged from 0.11 to 10.2 cm2 (i.e. reduction in surface area ± standard deviation = 1.8 ± 2.2 cm2). There were statistically nonsignificant differences between surface area measurements obtained by each observer, when the three designated methods were used. Statistically significant levels of agreement were revealed between measurements obtained by the two observers. Agreement could be seen by interobserver and by each observer in the two (intraobserver) trials performed in terms of tested methods for surface area measurement. Although no significant differences were revealed between the visual estimations of both observers and the pre-set gold standard for each lesion area, simple visual observation was revealed to have the highest possibility of bias [Table - 2].

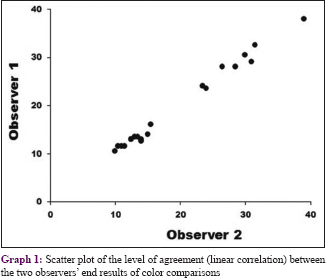
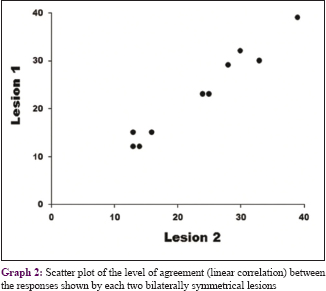
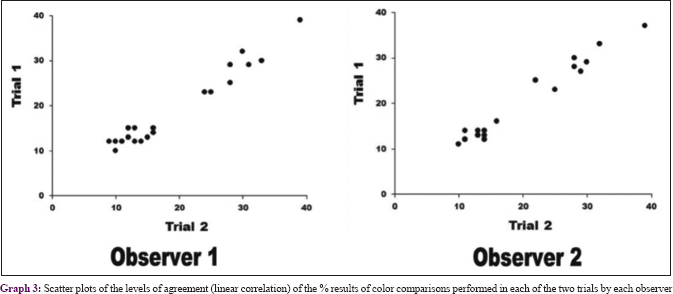
A statistically significant level of agreement was found between percentages of treatment results in the used lesion models obtained by the two observers (r = 0.995, P < 0.001). This agreement was reflected in the color difference measurement technique [Graph 1] and in the two trials done by each observer (r = 0.977 for observer 1 and 0.985 for observer 2; P < 0.001 for both observers) and important in implying the offered color difference measurement technique on selected lesion models [Graph 2]. There was also a statistically significant level of agreement between the percentages of treatment results obtained and the assessment of lesions selected from bilaterally symmetrical body portions (P < 0.001; r = 0.962) [Graph 3].
Discussion
There is currently a lack of consensus over the standardization of measurements for outcome in vitiligo. This makes it difficult to compare the outcome of different studies and cam hamper evidence-based recommendations.[8]
When insufficient or contradictory information are available on a certain topic, consensus-based methods, such as a Delphi method, or appropriate methods are generally considered to determine the extent to which experts agree on a specific topic.[9] Our Delphi survey results showed no agreement on the best tool to assess target or global re-pigmentation. In another study, the same has been found; yet, it was suggested that this absence of agreement was related to the limitations of electronic surveys used to address clinical measurements.[10] This seems to be a misinterpretation, because in a review of 96 studies, no two studies used exactly the same method of scoring for re-pigmentation.[11] Moreover, there is no agreement between physicians and patients evaluation of lesions re-pigmentation. Patients scored the degree of re-pigmentation generally higher than their physicians or the digital image analysis techniques, which may reflect wishful thinking, and is in line with their higher treatment satisfaction in comparison with physicians.[12] An important aspect of the therapeutic response is how patients feel about their vitiligo after treatment because there is a psychological point aspect to the disease.[13] This means that our results reflect the real and confusing situation out there.
Although 72% of our panelists were satisfied with the methods used for serial vitiligo assessment during treatment, 96% of them were interested in the idea of using a new computerized tool in vitiligo follow-up. This may be because the methods they were using were subjective (Vitiligo Area Scoring Index and as digital photography evaluation). This was not surprising as some published papers have highlighted the limitations of the Vitiligo Area Scoring Index scale and Vitiligo European Task Force score for small detectable change.[14],[15] 72% of our panelists were willing to allocate extra time in order to achieve greater accuracy in treatment, and 80% would accept a commercially valid computerized instrument for treatment if it was easy-to-use.
Key indicators of the quality of a measuring instrument are based on the reliability and validity of the measures. The process of developing and validating an instrument focuses on reducing error in the measurement process.[16] To validate our technique for assessment of surface area of lesions, we used circles with a known surface area and manually drew on graded papers. In a similar validating pilot study, authors had drawn their circles on the dorsa of hands of a number of volunteers,[4] but we believe that on conversion to a two-dimensional representation, there will be always an impossible-to-resolve trace of the third dimension even with very flat surfaces of the body.[17] Taking this into consideration, real skin was removed from the background in such validations; a wise decision as the frank areas of the drawn circles had to be free from biases resulting from eliminating the third dimension from the measurements.
In the present study, while all of the tested methods for surface area measurement showed significant accuracy when compared to the gold standard (P > 0.05 regarding all of the three techniques), simple visual observation was revealed to have the highest possibility of bias. It should be noted that simple visual observation was repeatedly reported to be an inaccurate technique of surface area assessment for skin lesions. Significant alterations were detected in the obtained measurements when compared with the gold standard, either during the vitiligo assessment [18],[19] or in other skin lesion assessments such as wounds.[20]
As for the point-counting technique, promising results were obtained using this simple technique (with all differences being < 1.5 cm2). The point-counting technique is considered a semi-objective method that can be used to assess depigmentation in vitiligo lesions.[7] When compared to visual assessments by the physician and/or analysis of photographs taken before and after treatment under visible or ultraviolet light, the point-counting technique can be considered more objective.[3]
The digital image analysis for surface area technique, had the least bias (all differences were < 1 cm2). Digital image analysis has the ability to overcome the inevitable differences between observers, which are intrinsic to a visual grading method.[12] One factor that could compromise the objectivity of C-DIAS is poor standardization of the position of the affected limbs or trunk at each visit. Poor standardization of the position could, in theory, alter the size of vitiligo lesions captured by the camera. Positioning the green marker adjacent to the vitiligo lesion and on difficult to photograph areas of the body i.e.with prominent curvature, eyelids, breasts and pretibial area could also lead to a lack of standardization.[21] A three-dimensional camera is ideal for such purposes and should be a subject for further research.[22]
Moreover, on comparison, when analyzing the risk of bias in the surface area reduction with the use of each technique, digital image analysis for surface area exhibited the best sensitivity, with the least bias being seen in digital image analysis for surface area (mean major bias ± standard deviation = −0.034 ± 0.74 cm2, with 95% of agreement from −0.26 to 0.2 cm2). Comparatively, simple visual observation showed the highest bias (a mean major bias ± standard deviation = −0.4 ± 1.34 cm2; with 95% of agreement from −0.3 to 2.24 cm2). Simple visual observance is more sensitive in detecting minor changes in pigmentation. Owing to its sensitivity, the technique is able to capture the small re-pigmentation progression, enabling physicians to assess and monitor therapeutic response over a smaller timeframe.[21]
As for color measurement, significant levels of agreement were found between the percentage of treatment results assessed in both inter- and intraobserver, with reliability of the offered method standing at r > 0.95; P < 0.001, regarding all tested domains. A strong correlation was also found regarding agreement between bilaterally symmetrical lesion responses (r = 0.96; P < 0.001). Given these findings, it was noted that the designated color analysis method could be appropriate for this task.
Although the topic “Methods of vitiligo case assessment” involves many titles, methodological literature has not come to any agreement on which tools are the most efficient in the treatment of this disease area. What is perhaps more worrisome is that there is no clear consensus regarding the objectivity of these techniques, either.
In addition, a quick review of the most recognized tool, the Vitiligo Area Scoring Index, confirms that the index does contain an element of subjectivity. The same is true of the Vitiligo European Task Force quantitative score. However, some tools are proved objective, such as digital image analysis. They can also provide data which could be a reference for dermatologists for universal assessment and can help for more objective comparisons between different studies, which may be better than simple visual observation and simple manual procedures such as the point-counting technique. In fact, in interobserver comparisons to detect the risk of bias in the surface area reductions with using each technique, digital image analysis for surface area exhibited the best sensitivity with the least biases being encountered.
Moreover, a fair concordance could be recognized among many authorities regarding the parameters examined during the assessment session of vitiligo lesions, mainly the surface area of the lesion and evident color improvement.
In this study, we tried to find a reasonablye simple quantitative tool that could deal with parameters to get a numerical representation of each of them.
Though most dermatologists are familiar with digital cameras, many of them lack the definite understanding of the basic concepts about digital images, cameras and imaging techniques. Improving their knowledge would be useful to their clinical practice.[23]
Conclusion
Based on this study, we found it relevant to offer a quantitative score to be used for complete evaluation of every case of vitiligo. Incorporation of our methods tested in current work have proven efficient. We proposed a five-log quantitative score [Table - 3] that took into consideration most of the literature reviews covering vitiligo patient's assessment. Depending on the first letter of each log, we called it the NANCY score (Nines, Area measurement, Naked re-pigmentation, Color analysis and Years of stability).
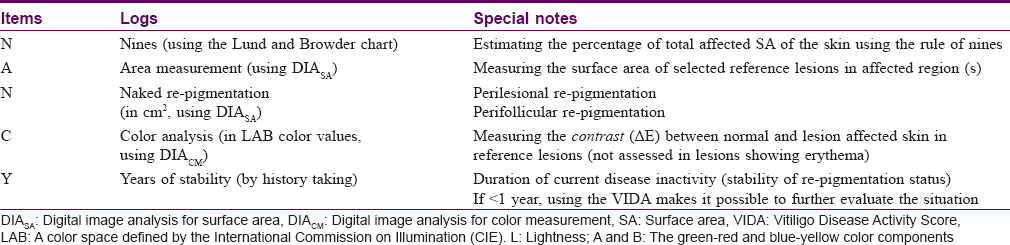
- The logs of the score:
- The log “nines”: The log uses the same methodology tracked by the Vitiligo European Task Force quantitative score to detect the extent of the disease; a criterion known to influence therapeutic decisions regarding generalized (nonsegmental) vitiligo
- The log “area measurement”: In designing the log, we used the recommendations of the Vitiligo European Task Force score approving the combination of Vitiligo European Task Force quantitative scores and a quantitative assessment of some target lesions (selected as references for follow-up) through computer analysis of digital images.
We recommended using “digital image analysis of photographic traces” to fulfill the log. Although implicating “digital image analysis of scanned traces” is more accurate, the former technique has a comparable accuracy and reliability in comparison to the latter one. The other causes for this choice were that:
- Using digital image analysis of scanned traces involves using extra-equipment (i.e., transparent sheets, black marker and a scanner of reasonable resolution) in addition to computer gadgets
- The third and fourth score logs require the presence of a photographic trace, so measuring the surface area using the same trace type is a reasonable choice.
- The logs “naked re-pigmentation” and “color analysis”:
There is concordance in dermatological literature that the pattern by which vitiligo lesions re-pigment in response to therapy can be identified through one of the three patterns:
- Marginal re-pigmentation (accentuated pigmentation at the edge of the lesion)
- Perifollicular re-pigmentation (areas of normal skin color around hair follicles)
- Diffuse re-pigmentation (reformed hue of the depigmented area of the lesion in response to therapy to gradually acquire a normal skin hue)
These three patterns were first accessed using clinical indicators. We perceived the first and second patterns as surface areas, which could be measured. Regarding the third pattern, in order to provide quantitative representation, the pattern should be assessed using an accurate and reliable color measurement technique (we speculated that digital image analysis for color measurement would be reasonable).
In terms of the fourth log, “color analysis,” when using pre- and posttreatment values, one can get a “per cent” representation of treatment results, across time intervals.
- The log “years' of stability”:
The stability of vitiligo is the single most important criterion in case of selection for surgical modalities. This is particularly true, given that unstable (i.e. progressive) lesions are known to have poor outcomes.
To qualify as “stable,” the re-pigmentation state must be maintained for a period of not < 1 year (which is why the “years” log is essential to the value scale). We found it reasonable to affix a specific log to determine current disease stability. This log is used primarily in the initial assessment session, when a decision is made about the most suitable therapy for the case at hand.
As vitiligo is a chronic condition, a document that carries information about previous period (s) of stability (or activity) of the disease regarding a case may be a worthy entity in the future (i.e. for long-term follow-up and future therapeutic decisions).
If the period of activity is < 1 year, it might be valuable for the dermatologist to score the period using a reasonable scale, to allow for both therapeutic decisions and to help in keeping track of changes (if any), in addition to the best courses of therapy. We recommend using Vitiligo Disease Activity Score (VIDA) to overcome assessment and treatment challenges. The benefits of this log go beyond the initial assessment session, to involve the planned upcoming sessions as well.
- Proposals about the ideal use of the score and the offered modifications:
By designing the NANCY score, we tried to provide a quantitative worksheet for assessment of vitiligo patients.
The logs of the score were designated after carefully reviewing the methodological literature and outlining the advantages and disadvantages of each proposed and/or tested technique. We also took into consideration the expected results of the tested quantitative tools as part of the current study.
In the NANCY score, we quantitatively accessed nearly all criterion for assessment of a case of vitiligo; both initially and in follow-up. We believed that the score would be ideal for use in both clinical sessions and in research drives.
The score was intended to be a flexible tool. One can voluntarily cancel a log if it is not suitable for the assessed case or medication. An example would be a study comparing two types of topical remedies. The main concern in such a study would be the effect of the studied topical medications on individual lesions; therefore, there would be no need for the first log score. The same can be held true for segmental vitiligo and vitiligo of the lips and extremities.
However, it is recommended to fulfill every log whenever possible because, as previously mentioned, documentation of comprehensive data is very important for nearly every case of vitiligo. This is particularly important as the condition is known to be chronic with possible exacerbation, following a satisfactory remission (might be after a period of years).
Finally, we must not allow ourselves to be constrained by the presence of a computer gadget in using the score. The logs that require software tools can be adjusted to be used in simple manual forms. The point-counting technique could be a feasible alternative to digital image analysis for surface area. In addition, the digital image analysis for color measurement procedure can be replaced by matching the observed vitiligo lesion color with a color check chart, which contains analogous patches of all possible skin tones. These tones cover both diseased and normal skin with the procedure being repeated in every follow-up visit, to observe if any changes have occurred. Such a chart can be generated and printed using a reliable software tool.
Limitations
Many dermatologists lack the definite understanding of basic concepts about digital images, cameras and imaging techniques. The study does not include a traditional assessment method such as using Vitiligo Area Scoring Index.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Batchelor JM, Tan W, Tour S, Yong A, Montgomery AA, Thomas KS. Validation of the vitiligo noticeability scale: A patient-reported outcome measure of vitiligo treatment success. Br J Dermatol 2016;174:386-94.
[Google Scholar]
|
| 2. |
Oh TS, Lee O, Kim JE, Son SW, Oh CH. Quantitative method for measuring therapeutic efficacy of the 308 nm excimer laser for vitiligo. Skin Res Technol 2012;18:347-55.
[Google Scholar]
|
| 3. |
Dicle O. Assessment methods in vitiligo. J Pigment Dis 2015;2:160.
[Google Scholar]
|
| 4. |
Molnar JA, Lew WK, Rapp DA, Gordon ES, Voignier D, Rushing S, et al. Use of standardized, quantitative digital photography in a multicenter web-based study. Eplasty 2009;9:e4.
[Google Scholar]
|
| 5. |
Feily A. Vitiligo extent tensity index (VETI) score: A new definition, assessment and treatment evaluation criteria in vitiligo. Dermatol Pract Concept 2014;4:81-4.
[Google Scholar]
|
| 6. |
Marrakchi S, Bouassida S, Meziou TJ, Turki H, Zahaf A. An objective method for the assessment of vitiligo treatment. Pigment Cell Melanoma Res 2008;21:106-7.
[Google Scholar]
|
| 7. |
Alghamdi KM, Kumar A, Taïeb A, Ezzedine K. Assessment methods for the evaluation of vitiligo. J Eur Acad Dermatol Venereol 2012;26:1463-71.
[Google Scholar]
|
| 8. |
Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. Lancet 2015;386:74-84.
[Google Scholar]
|
| 9. |
Prinsen CA, Vohra S, Rose MR, King-Jones S, Ishaque S, Bhaloo Z, et al. Core Outcome Measures in Effectiveness Trials (COMET) initiative: Protocol for an international Delphi study to achieve consensus on how to select outcome measurement instruments for outcomes included in a 'core outcome set'. Trials 2014;15:247.
[Google Scholar]
|
| 10. |
Gan EY, Eleftheriadou V, Esmat S, Hamzavi I, Passeron T, Böhm M, et al. Repigmentation in vitiligo: Position paper of the vitiligo global issues consensus conference. Pigment Cell Melanoma Res 2017;30:28-40.
[Google Scholar]
|
| 11. |
Whitton ME, Pinart M, Batchelor J, Leonardi-Bee J, González U, Jiyad Z, et al. Interventions for vitiligo. Cochrane Database Syst Rev 2015;CD003263.
[Google Scholar]
|
| 12. |
Linthorst Homan MW, Wolkerstorfer A, Sprangers MA, van der Veen JP. Digital image analysis vs. clinical assessment to evaluate repigmentation after punch grafting in vitiligo. J Eur Acad Dermatol Venereol 2013;27:e235-8.
[Google Scholar]
|
| 13. |
Kawakami T, Hashimoto T. Disease severity indexes and treatment evaluation criteria in vitiligo. Dermatol Res Pract 2011;2011:750342.
[Google Scholar]
|
| 14. |
Lim HW, Grimes PE, Agbai O, Hamzavi I, Henderson M, Haddican M, et al. Afamelanotide and narrowband UV-B phototherapy for the treatment of vitiligo: A randomized multicenter trial. JAMA Dermatol 2015;151:42-50.
[Google Scholar]
|
| 15. |
Komen L, da Graça V, Wolkerstorfer A, de Rie MA, Terwee CB, van der Veen JP. Vitiligo Area Scoring Index and Vitiligo European Task Force assessment: Reliable and responsive instruments to measure the degree of depigmentation in vitiligo. Br J Dermatol 2015;172:437-43.
[Google Scholar]
|
| 16. |
Kimberlin CL, Winterstein AG. Validity and reliability of measurement instruments used in research. Am J Health Syst Pharm 2008;65:2276-84.
[Google Scholar]
|
| 17. |
Orrite-Urunuela C, del Rincon JM, Herrero-Jaraba JE, Rogez G. 2D silhouette and 3D skeletal models for human detection and tracking. Pattern Recognit 2004;4:244-7.
[Google Scholar]
|
| 18. |
Van Geel N, Vander Haeghen Y, Ongenae K, Naeyaert JM. A new digital image analysis system useful for surface assessment of vitiligo lesions in transplantation studies. Eur J Dermatol 2004;14:150-5.
[Google Scholar]
|
| 19. |
Aydin F, Senturk N, Sahin B, Bek Y, Yuksel EP, Turanli AY, et al. A practical method for the estimation of vitiligo surface area: A comparison between the point counting and digital planimetry techniques. Eur J Dermatol 2007;17:30-2.
[Google Scholar]
|
| 20. |
Keast DH, Bowering CK, Evans AW, Mackean GL, Burrows C, D'Souza L. MEASURE: A proposed assessment framework for developing best practice recommendations for wound assessment. Wound Repair Regen 2004;12:S1-17.
[Google Scholar]
|
| 21. |
Shamsudin N, Hussein SH, Nugroho H, Fadzil MH. Objective assessment of vitiligo with a computerised digital imaging analysis system. Australas J Dermatol 2015;56:285-9.
[Google Scholar]
|
| 22. |
Kohli I, Isedeh P, Al-Jamal M, DaSilva D, Batson A, Canfield D, et al. Three-dimensional imaging of vitiligo. Exp Dermatol 2015;24:879-80.
[Google Scholar]
|
| 23. |
Kaliyadan F, Manoj J, Venkitakrishnan S, Dharmaratnam AD. Basic digital photography in dermatology. Indian J Dermatol Venereol Leprol 2008;74:532-6.
[Google Scholar]
|
Fulltext Views
4,806
PDF downloads
2,241





![[Table - 1]](#tbl_ijdvl_2019_85_5_466_251834_t1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2019_85_5_466_251834_t2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2019_85_5_466_251834_t3.jpg){kind=link}