Translate this page into:
Cream-yellow and firm nodule in finger pad
2 Department of Pathology, the First Attached Hospital of Hebei North University, No. 12, Changqing Road, Zhangjiakou City, Hebei Province, 075000, China
Correspondence Address:
Li-qiang Zheng
Department of Dermatology, the 251st Hospital of Chinese PLA, No.13, Jian'guo Road, Zhangjiakou city, Hebei Province, 075000
China
| How to cite this article: Zheng Lq, Han Xc. Cream-yellow and firm nodule in finger pad. Indian J Dermatol Venereol Leprol 2012;78:522 |
A 62-year-old male came with 1 week history of multiple cream-yellow, pus-like, firm nodules in the finger pads of his left thumb, index and middle finger, measuring 2 to 5 mm in diameter [Figure - 1]. He had pricking sensation and red swelling over the distal interphalangeal joints on the left hand. He had past medical history of hypertension (20 years duration), treated with enalapril maleate (10 mg, q.d, p.o), of type 2 diabetes mellitus (6 years), treated with metformin hydrochloride (250 mg, b.i.d, p.o) and of cerebral infarction (5 years) without timely treatment. His blood pressure and fasting blood glucose were well-controlled while left hemiplegia sequelae persisted.
 |
| Figure 1: Cream-yellow firm nodule, pus-like, measuring 2 mm in diameter in his thumb on the left hand |
His serum uric acid was 8.63 mg/dL (normal ≤ 7.0 mg/dL), creatinine 1.17 mg/dL (normal 0.36 ~1.10 mg/dL), CRP 91.2 mg/L (normal 0~8 mg/L), erythrocyte sedimentation rate (ESR) 44 mm/h (normal ≤ 20 mm/h) and urinary α1 microglobulin 22.4 mg/L (normal 0~12.8 mg/L). Plain X-ray of left hand and ultrasonography of kidney were unremarkable.
Biopsy was performed, and specimen suspicious of calcification was fixed in formaldehyde. Histopathological examination indicated that plenty of crystals deposited in the dermis and were surrounded by multiple foreign body type giant cells, fibrous tissue hyperplasia and inflammatory elements [Figure - 2]a. Clusters of needle-like crystals were mostly dissolved by formaldehyde, leaving some characteristic basophilic granular deposit [Figure - 2]b.
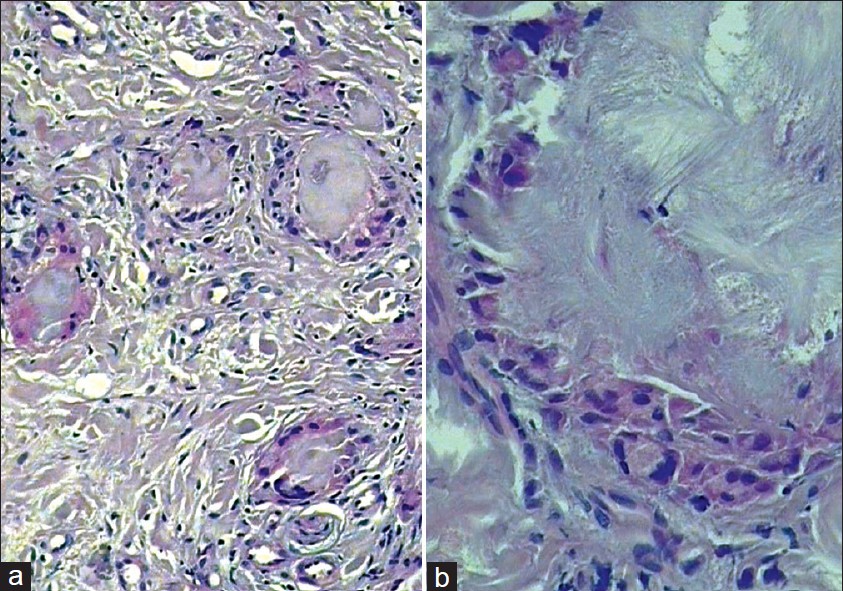 |
| Figure 2: (a) Plenty of crystals were deposited in the dermis and surrounded by multiple foreign body type giant cells (H and E, ×200). (b) Crystals were mostly dissolved by formaldehyde, leaving some characteristic basophilic granular deposit (H and E, ×400) |
What′s your diagnosis?
Answer
Diagnosis: Finger pad tophi
Discussion
Gout, "the king of diseases and the disease of kings", is an inflammatory arthritis caused by deposition of monosodium urate (MSU) crystals in articular or peri-articular tissues and in the kidney. [1] It affects 1% - 2% of adults in developed countries. [2] The formation of MSU crystals depends on local concentration of urate, which is tightly correlative with the articular hydration state, temperature, pH, concentration of cations and the presence of extracellular matrix.[3] Peripheral joints with low temperature (i.e. the dorsal aspect of the proximal interphalangeal, metacarpophalangeal joints and the dorsal toes) are the predilections of gouty tophi. It is generally believed that gout and hyperuricemia are clinically associated with diabetes mellitus, hypertension, metabolic syndrome, renal and cardiovascular diseases. [2]
Generally speaking, there are 4 stages in the development of gout: Asymptomatic hyperuricemia, the gouty attack, the intercritical period and chronic gouty arthritis. [4] In fact, there are no clear boundaries between them. In some cases, hyperuricemia can exist for many years before the first clinical attack of gout, and skin manifestations may appear in any stage even without a prior history of gout. So far, few reports on dermatologic features as the first attack of gout was documented, especially in the finger pad. [5]
The pathological features of our case were similar to those of the reported gouty tophi in finger pad, except for unilateral lesions and concomitant multiple systemic diseases. The diagnosis of gout is certain by its specific histopathologic features although specimen fixed in formaldehyde and further inspection by polarized light microscopy is not employed due to limited facilities in our hospital. Without the consent of the patient, biopsy from another lesion fixed in absolute ethanol was not performed.
It is difficult to distinguish the initial lesion from acroscleroderma, cutaneous calcification, septic arthritis, rheumatoid nodules etc. Tophi can also take the form of intradermal superficial collections, resembling pus in the finger pad. Other differential diagnosis includes other crystal-induced forms of arthritis such as pseudogout / chondrocalcinosis with deposition of calcium pyrophosphate dehydrate crystals and oxalosis arthropathies.
The acute symptoms subsided gradually with the treatment of allopurinol (100 mg, t.i.d, p.o) for 2 weeks. Our patient did not receive any drug, which could have decreased an excretion of uric acid. Finally, the serum uric acid and creatinine level were re-evaluated, and the results were normal. No further flares of gout occurred again.
As gout itself becomes more common, so too will the cutaneous manifestations. [4] Hence, the dermatologist must be poised and sensitive while making an initial diagnosis of gout.
| 1. |
Wortmann RL. Gout and hyperuricemia. In: Firestein G, editor. Kelley's Textbook of Rheumatology. 8 th ed. Philadelphia: Saunders Elsevier; 2008. p. 1481-524.
th ed. Philadelphia: Saunders Elsevier; 2008. p. 1481-524.'>[Google Scholar]
|
| 2. |
Richette P, Bardin T. Gout. Lancet 2010;375:318-28.
[Google Scholar]
|
| 3. |
Choi HK, Mount DB, Reginato AM. Pathogenesis of gout. Ann Intern Med 2005;143:499-516.
[Google Scholar]
|
| 4. |
Falasca GF. Metabolic diseases: gout. Clin Dermatol 2006;24: 498-508.
[Google Scholar]
|
| 5. |
Holland NW, Jost D, Beutler A, Schumacher HR, Agudelo CA. Finger pad tophi in gout. J Rheumatol 1996;23:690-2.
[Google Scholar]
|
Fulltext Views
21,313
PDF downloads
3,321





![[Figure - 1]](#fig_ijdvl_2012_78_4_522_98107_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_4_522_98107_u2.jpg){kind=link}