
Translate this page into:
Cutaneous melioidosis presenting as multiple abscesses
Corresponding author: Dr. Arpita Nibedita Rout, Department of Dermatology, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India. arpitanrout1988@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rout AN, Sirka CS, Mohanty S, Garg S. Cutaneous melioidosis presenting as multiple abscesses. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_1404_2024
Dear Editor,
Melioidosis is caused by Burkholderia pseudomallei. It can affect multiple organ systems and is most commonly encountered in immunocompromised individuals.1 Cutaneous involvement can occur primarily or secondary to dissemination from other organ involvement.2 The cutaneous lesions may present with varied morphologies, such as abscesses, cellulitis, ulcers and nodules. Hence, they can mimic many other common cutaneous infections. We describe a case of multifocal cutaneous abscess due to Burkholderia pseudomallei in a patient with breast carcinoma.
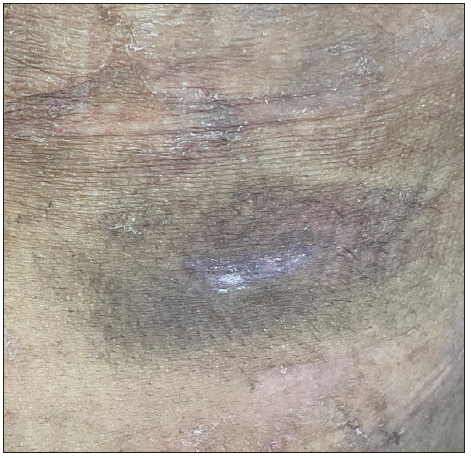
A 51-year old housewife, a patient with metastatic carcinoma of the breast, presented with multiple skin swellings with mild pain, developing over a week. There was no history of fever or other systemic symptoms. She had completed chemotherapy for the malignancy two years ago and had received one cycle of radiotherapy. She did not recall any history of trauma or outdoor activity prior to the development of the lesions. On examination, there were multiple well-to-ill-defined abscesses, with an indurated surface at the outer portion with apparently normal-looking skin and a central area showing erythema, distributed over the trunk and extremities [Figure 1]. On palpation, the swellings showed softening in the central part with minimal tenderness. She was admitted with a provisional diagnosis of bacterial abscess. Routine tests were normal. Aspirated pus was sent for culture and sensitivity testing, and showed growth of Burkholderia pseudomallei sensitive to ceftazidime, meropenem and cotrimoxazole [Figures 2a, 2b, and 2c]. Pus was negative for the cartridge-based nucleic acid amplification test for Mycobacterium tuberculosis. Complete blood counts were within normal limits. The blood sample was negative for culture and sensitivity A final diagnosis of multifocal cutaneous melioidosis was made. She received intravenous meropenem for three weeks and oral cotrimoxazole for two months. Few of the abscesses necessitated incision and drainage [Figure 3]. All the lesions had healed completely with post-inflammatory hyperpigmentation by the two-month follow-up. The patient was advised to continue oral cotrimoxazole for an additional four months.

- Right buttock showing skin-coloured to erythematous nodular swelling with erythema limited to the central part only.
![Image showing classical safety pin appearance of the Gram negative organism. [Gram stain, 100x].](/content/126/2025/0/1/img/IJDVL_1404_2024-g2.png)
- Image showing classical safety pin appearance of the Gram negative organism. [Gram stain, 100x].

- Pink colonies of Burkholderia pseudomellie on MacConkey agar.
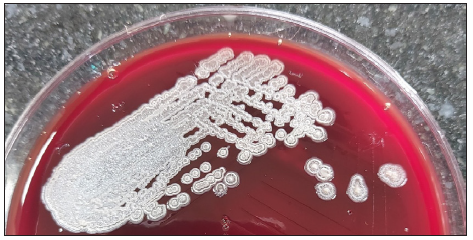
- Cream-coloured colonies of Burkholderia pseudomellie on blood agar.
- Complete healing of the lesion at two months follow-up.
Melioidosis is one of the emerging pathogens which can affect almost all organ systems. Immunocompromised individuals are more likely to develop all forms of cutaneous melioidosis.
The causative organism is found in water and soil in the endemic areas. Minor skin abrasions usually act as the point of entry and can result in primary localised cutaneous melioidosis. Multifocal lesions may result from the hematogenous dissemination.
The morphological presentation may be varied; and can thus lead to confusion and delay in diagnosis. Various presentations include nodular lesions, abscesses, cellulitis, and ulceration. Such lesions may be caused due to a large number of pathogenic organisms. Hence, history of evolution and clinical morphology may help in diagnosis. We have compiled the various characteristic features of these differentials in Table 1.
| Causative organism/Symptoms | Bacterial abscesses | Tubercular gumma | Atypical mycobacterial abscess | Cutaneous melioidosis |
|---|---|---|---|---|
| Duration (average) | Few days (1-7 days) | Few weeks (one to two months) | Few days (7-14 days) | Few days (7-14 days) |
| Local symptoms | Severe pain | No pain/very minimal pain | Moderate pain | Minimal pain |
| Systemic symptoms | Fever | Fever, loss of appetite, loss of weight, night sweats | Usually absent | Usually absent if only cutaneous abscess |
| Evolution | Ruptures spontaneously in 4-7 days | Usually requires assisted rupture, or ruptures late (after few weeks) | Ruptures after 1-10 days | Ruptures rarely, requires incision and drainage |
| Discharge | Profuse purulent discharge | Sero-purulent, minimal | Sero-purulent, moderate amount | Purulent discharge, profuse |
| Morphology | Erythematous nodule with central/tip showing purulent discharge | Subcutaneous nodular lesions with sinuses and ulceration with perilesional hyperpigmentation, puckering scar | Subcutaneous nodules with erythema, sinus and ulceration | Erythema limited to the centre part of the lesion |
| Diagnosis | Bacterial culture and sensitivity and Gram stain | CBNAAT positive, Quantiferon TB Gold | Culture, PCR | Gram stain and culture, VITEK |
| Treatment | Antibiotics (empirical or as per culture sensitivity) | Antitubercular therapy | Minocycline, fluoroquinolones, amikacin | Meropenem, ceftazidime, cotrimoxazole |
Our case had multiple abscesses, with only the central part of the abscess showing erythema with minimal pain. Fever was absent. This presentation may be labelled as a partially cold abscess. Identifying this morphological pattern may help in differentiating melioidosis abscess from other causes of cutaneous abscesses.
Diagnosis of melioidosis is by isolation of the organism in the clinical samples, using various methods, such as culture media like blood agar, MacConkey agar, or selective media like Ashdown’s medium or Burkholderia pseudomallei selective agar.1,3 VITEK medium can identify the organism with 99% probability.1 16SrRNA and groEL gene sequencing, identification by polymerase chain reaction, indirect hemagglutination assay, enzyme-linked immunosorbent assay, lateral flow immunoassay, and matrix-assisted laser desorption ionisation time-of-flight mass spectrometry (MALDI-TOF MS) are few of the newer diagnostic techniques, but the utility of these methods is limited due to non-availability in resource-poor centres.3,4 Once the diagnosis is established, the treatment comprises of two phases: intensive phase of intravenous administration of meropenem or ceftazidime, followed by a continuation phase of oral cotrimoxazole for six months.
Our case showed that the lesions started as skin-coloured swellings with induration, and there was gradual evolution of erythema and softening in the central parts of the abscess. This finding was consistent in all the lesions. Hence, such evolution and morphological presentation may indicate melioidosis being the causative factor.
We report this case to highlight the importance of identifying the cutaneous morphology and establishing the evolution of the lesions in the diagnosis of cutaneous melioidosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
References
- Melioidosis complicating lepromatous leprosy with type 2 lepra reaction: A rare case report. Leprosy Rev. 2019;90:450-5.
- [CrossRef] [Google Scholar]
- Cutaneous melioidosis. In: Mohapatra PR, ed. Clinical melioidosis: A practical guide to diagnosis and management (1st edition). Florida: CRC Pressl; 2023. p. :125-130.
- [Google Scholar]
- Laboratory diagnosis of melioidosis: Past, present and future. Exp Biol Med (Maywood). 2015;240:742-51.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Comprehensive approaches for the detection of Burkholderia pseudomallei and diagnosis of melioidosis in human and environmental samples. Microb Pathog. 2022;169:105637.
- [CrossRef] [PubMed] [Google Scholar]




