
Translate this page into:
Dermoscopy of Bowen’s disease: A case series of five patients
Corresponding author: Dr. Rashmi Kumari, Department of Dermatology, Venereology and Leprosy, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry, India. rashmi.sreerag@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Behera B, Kumari R, Thappa DM, Gochhait D, Srinivas BH, Ayyanar P. Dermoscopy of Bowen’s disease: A case series of five patients. Indian J Dermatol Venereol Leprol 2021;87:576-80.
Sir,
Bowen’s disease, a premalignant tumor of the elderly, usually presents as a slowly enlarging, well-defined, skin-colored, erythematous to pigmented scaly and/or crusted plaque often on the chronically sun-damaged skin. The plaque may be pigmented or non-pigmented and rarely can be eroded or ulcerated.1,2 Early and accurate diagnosis of Bowen’s disease is essential for preventing its malignant transformation.2 Dermoscopic examination improves the diagnostic accuracy of Bowen's disease.1-3
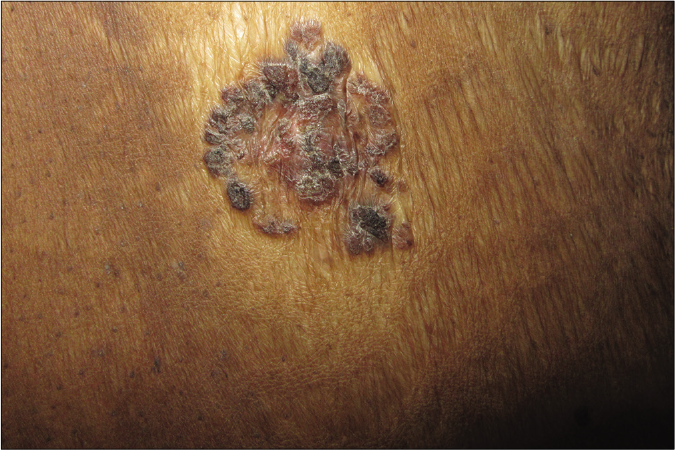
The five patients in our series belonged to skin phototype IV and V. The clinical and dermoscopic details of all the cases [Figures 1-12] are mentioned in Table 1. All the lesions were pigmented [Figures 1, 5,6 and 9], except for one [Figure 11]. The diagnosis of Bowen’s disease was established by histopathological examination.

- Well-defined, thin, brown, crusted plaque with a thread-like border on a scar
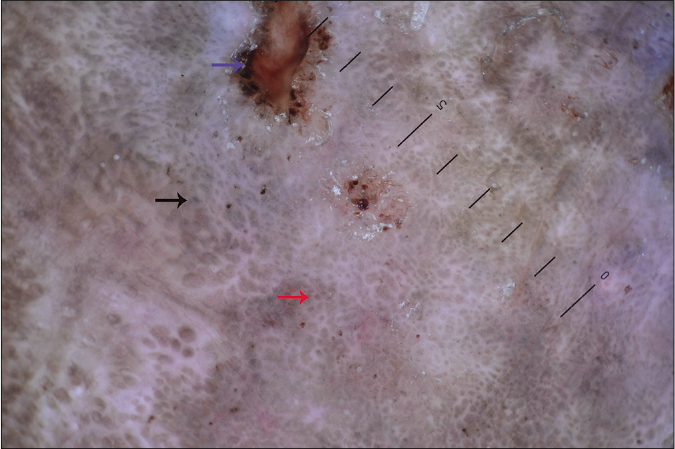
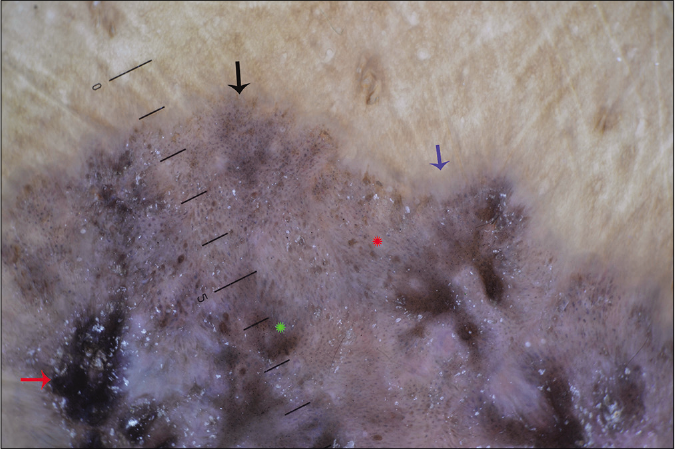
- Dermoscopic examination (HEINE DELTA20® Dermatoscope, ×10) under non-polarized mode showing ulcer (blue arrow), white network (red arrow) and blue-gray globules (black arrow)
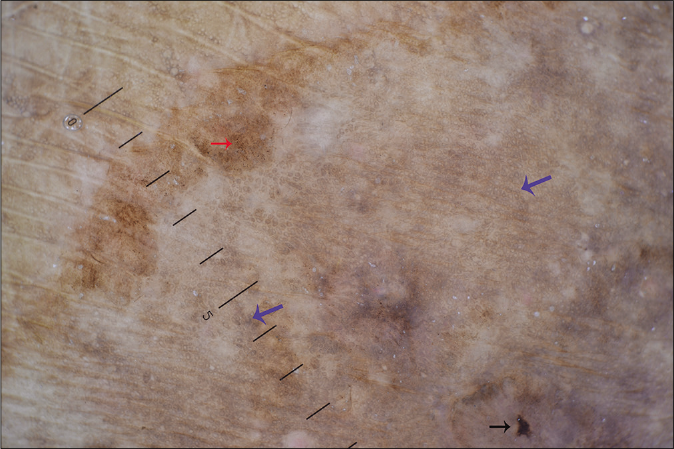
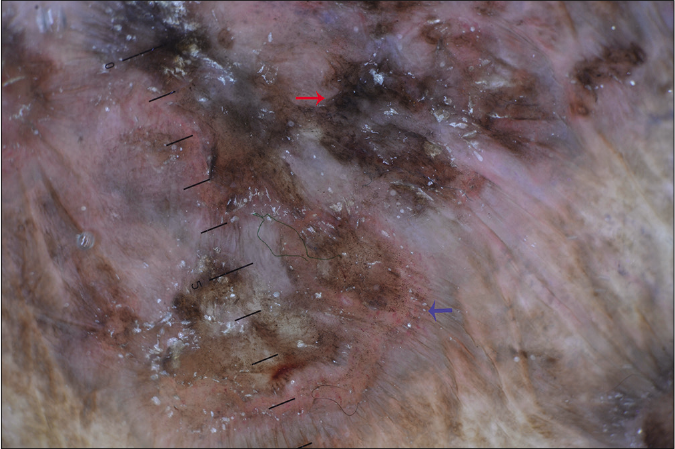
- Dermoscopic examination (HEINE DELTA20® Dermatoscope, ×10) under non-polarized mode showing ring-like pattern (blue arrows) and clustered brown dots (red arrow) at the periphery
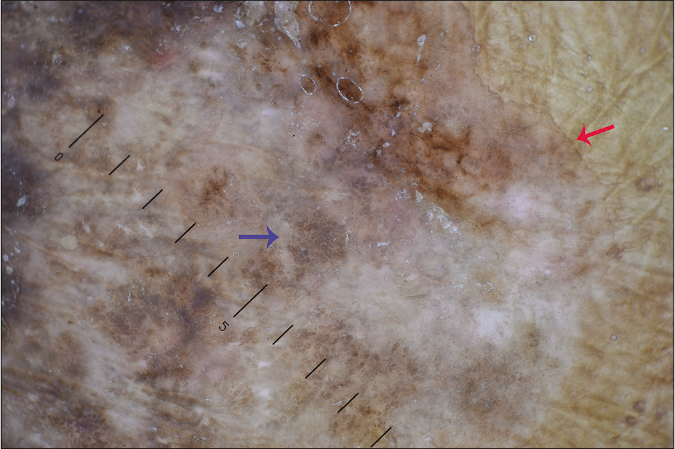
- Dermoscopic examination (HEINE DELTA20® Dermatoscope, ×10) under non-polarized mode showing clustered ring-like pattern (blue arrows) and well-defined thin brown outer border (red arrow)
- Well-defined, thin, erythematous-to-brown, crusted plaque with a thread-like border
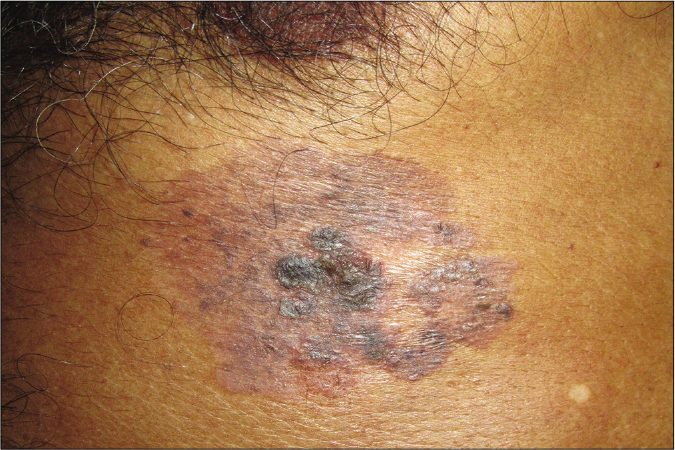
- Multiple grouped, erythematous, crusted papules coalescing to form a plaque
- Dermoscopic examination (HEINE DELTA20® Dermatoscope, ×10) under non-polarized mode showing the dark brown keratotic structureless area (red arrow), gray-white homogenous area, clustered brown (fluorescent Asterix) dots, blue-gray dots and globules in a linear (red asterix) and clustered arrangement (black arrow), scales and an ill-defined gray outer border (blue arrow)
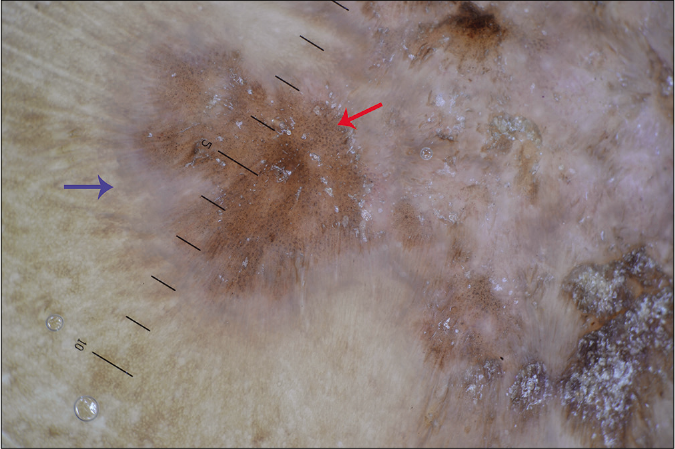
- Dermoscopic examination (HEINE DELTA20® Dermatoscope, ×10) under non-polarized mode showing the brown keratotic structureless area (red arrow) and corona of glomerular vessels (blue arrow)

- Ill-defined, reddish-brown, crusted plaque
- Dermoscopic examination (HEINE DELTA20® Dermatoscope, ×10) under non-polarized mode showing brown homogenous area, blue-gray peppering (red arrow), gray-white homogenous area and ill-defined gray outer border (blue arrow)
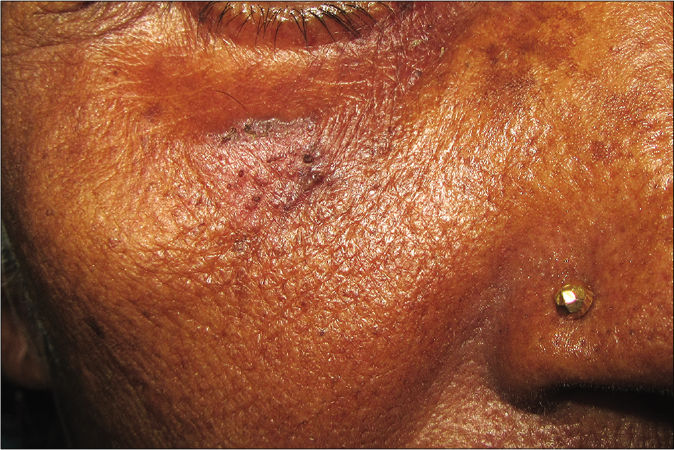
- Thin, erythematous plaque with an elevated border
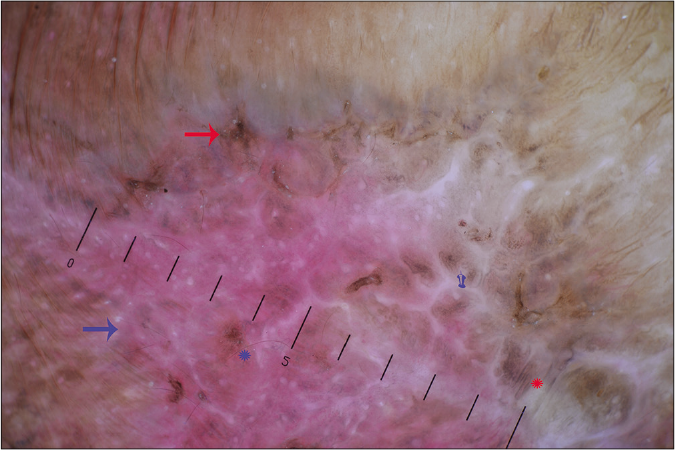
- Dermoscopic examination (HEINE DELTA20® Dermatoscope, ×10) under non-polarized mode showing red-white homogenous area (blue arrow), multiple erosions (red arrow), interconnecting white lines, brown to blue-gray dots in a clustered (blue asterisk) arrangement and blue-gray radial lines (red asterix) and fine peppering (pin)
| Cases | Age in years/ gender | Site | Clinical morphology | Differential diagnosis | Dermoscopic features |
|---|---|---|---|---|---|
| 1 | 70/M | Left thigh (on a preexisting scar) | Gray-brown thin polycyclic plaque with well-defined thread-like border and overlying crusting | Superficial BCC, BD |
Brown keratotic structureless area Brown and blue-gray dots in a clustered and linear arrangement Ring-like structures in a diffuse or clustered arrangement Homogenous brown and white area (multifocal) Brown(fine) peppering(dots without circumscription) Ulceration Negative pigment network Scales Well-defined thin brown outer border Clustered glomerular vessels Blood spots |
| 2 | 48/M | Left inframammary area | Well-defined erythematous to brown thin plaque with thread-like border | Superficial BCC | Gray-brown keratotic structureless area Blue-gray (coarse) peppering Brown dots arranged in a clustered arrangement Well-defined thin brown outer border Scales |
| 3 | 66/F | Suprapubic area | Multiple grouped erythematous crusted papules | Discoid eczema | Light to dark brown keratotic structureless area Gray-white homogenous area Brown to blue-gray dots and globules in a linear and clustered arrangement Ill-defined gray outer border Scales Glomerular vessels in the periphery Hairpin vessels |
| Left thigh | Well-defined thin light brown plaque with verrucous surface | Brown keratotic structureless area Brown and blue-gray dots in a cluster arrangement Gray-white and brown homogenous area Ill-defined gray outer border Scales Glomerular vessels in a cluster arrangement Blood spots |
|||
| Left thigh | Ill-defined reddish-brown crusted plaque | Brown keratotic structureless area Brown and blue-gray dots and globules in a clustered and linear arrangement Gray-white homogenous area Scales Glomerular vessels in a clustered arrangement |
|||
| Left knee | Well-defined verrucous plaque | Gray-white keratotic structureless area Scales Ill-defined gray outer border |
|||
| 4 | Abdomen | Erythematous to a pigmented thin plaque with thread-like border | Superficial BCC, BD |
Homogenous red-white, brown and blue-gray area Brown and blue-gray dots in a clustered arrangement Brown and blue-gray(fine) peppering Ill-defined gray outer border Blood crust |
|
| 5 | 51/F | Right infraorbital area | Thin erythematous plaque with an elevated border | Superficial BCC | Red-white homogenous area Multiple erosions Interconnecting white lines Brown to blue-gray dots in a clustered and linear arrangement Blue-gray radial lines and(fine) peppering |
BD: Bowen’s disease, BCC: Basal cell carcinoma
Pigmented Bowen's disease is rare, and constitutes 1.7– 6% of the cases. It is commonly described in dark skin individuals and on the sun-protected areas.3,4 In our series, except for one case, all lesions were pigmented and occurred on the sun-protected areas. The close clinical mimics of pigmented Bowen’s disease include melanocytic lesions including melanoma and non-melanocytic lesions such as pigmented actinic keratosis, basal cell carcinoma, especially the superficial variant, seborrheic keratosis and lentigo. A pathological examination is often necessary to arrive at a diagnosis of Bowen’s disease.
The number of studies describing the dermoscopic features of pigmented Bowen’s disease is far less than that for non-pigmented Bowen’s disease. Buggati et al. described the presence of a multicomponent global pattern, dotted vessels and a scaly surface to be the characteristic features of Bowen’s disease.5 Later, Zalaudek et al. described the presence of a scaly surface with glomerular vessels in non-pigmented Bowen’s disease and additional pigmented small globules and/ or homogeneous pigmentation in pigmented Bowen’s disease, to be the specific features.2 A similar observation was noted by Mun et al.6
In pigmented Bowen’s disease, we observed a combination of Bowen’s disease-associated pigmented structures such as brown keratotic structureless area, homogenous area of different shades (focal/multifocal), brown to blue-gray dots/ globules (in a peripheral clustered or linear arrangement) and brown to blue-gray peppering (fine and coarse) along with scaling and focally clustered glomerular vessels [Figures 7,8 and 10]. In two lesions, glomerular vessels were arranged peripherally outside the keratotic structureless area [Figure 8]. A similar observation was named as the corona of glomerular vessels by Payapvipapong et al.7 In the present series, the vascular structures were obstructed from the dermoscopic visibility either due to pigmented structure or severe overlying hyperkeratosis. No vessels were visible in the brown keratotic structureless area or brown homogenous area [Figure 8]. In our series, the only non-pigmented Bowen’s disease was dominated by the presence of a red-white structureless area with superficial erosions. It lacked a structureless keratotic area and glomerular vessels [Figure 12], making it difficult to distinguish it from superficial basal cell carcinoma. We did not notice any pigment streaks, or pigment network in our series, although one case showed a white network-like area [Figure 2].
There is considerable variation in the description of the dermoscopic structure that clinically corresponds to the brown crusting. The various terms used are irregular diffuse pigmentation, blotch, structureless brown and blue-gray pigmentation with keratosis, hyperkeratotic scaly area and verrucous structure.6-10 We termed it as brown keratotic structureless area, as the area is structureless and keratotic and different from the brown homogenous area. Similarly, we used the term peppering, both fine and coarse [Figure 10], for pigmented structures that are not round or circumscribed and are different from dots and globules. Some authors have used the term peppering, while others used different names such as dust-like gray dots.1,7
We observed three new dermoscopic features. In a diffuse or clustered arrangement [Figures 3 and 4], a ring-like pattern was observed in one case that possibly correlated to the hyperpigmented epithelial cells in broadened rete ridges and the keratinocytes above the dermal papillae without hyperpigmentation. A well-defined thin brown outer border [Figure 4] and an ill-defined gray outer border [Figures 7 and 10] were observed in four and three lesions of Bowen’s disease, respectively. A double-edge border, two parallel pigmented lines at the periphery, was described by Yang et al. correlated to the acanthotic epidermis interrupted by regions of the relatively thinner epidermis and loss of rete ridges.1
In conclusion, we describe eight Bowen’s disease’s dermoscopic features in five patients with skin phototype IV and V. Furthermore, we report new dermoscopic features such as ring-like pattern, ill-defined gray outer border and well-defined thin brown outer border in pigmented Bowen’s disease. The presence of brown keratotic structureless area, clustered brown to blue-gray dots and globules, scales and clustered glomerular vessels in dark skin should raise a suspicion of Bowen’s disease.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest.
References
- What's new in dermoscopy of Bowen's disease: Two new dermoscopic signs and its differential diagnosis. Int J Dermatol. 2017;56:1022-5.
- [CrossRef] [PubMed] [Google Scholar]
- The specific dermoscopic criteria of Bowen's disease. J Eur Acad Dermatol Venereol. 2006;20:361-2.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopy clues in pigmented Bowen's disease. Dermatol Res Pract. 2010;2010:464821.
- [CrossRef] [PubMed] [Google Scholar]
- Dermatoscopy of pigmented Bowen's disease. J Am Acad Dermatol. 2010;62:597-604.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopic observation of Bowen's disease. J Eur Acad Dermatol Venereol. 2004;18:572-4.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopic features of Bowen's disease in Asians. J Eur Acad Dermatol Venereol. 2010;24:805-10.
- [CrossRef] [PubMed] [Google Scholar]
- Corona of glomerular vessels: A diagnostic marker of hyperkeratotic Bowen's disease. Dermatol Surg. 2013;39:1395-8.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical and dermoscopic features of pigmented Bowen disease. Actas Dermosifiliogr. 2008;99:419-20.
- [CrossRef] [Google Scholar]
- Accuracy of dermoscopic criteria for the differentiation between superficial basal cell carcinoma and Bowen's disease. J Eur Acad Dermatol Venereol. 2018;32:1914-9.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between dermoscopy and pathology in a case of clonal-type pigmented Bowen's disease: Observation with vertical-view dermoscopy. J Dermatol. 2019;46:436-9.
- [Google Scholar]




